
Abstract
This article analyzes wireless communication protocols that could be used in healthcare environments (e.g., hospitals and small clinics) to transfer real-time medical information obtained from noninvasive sensors. For this purpose the features of the three currently most widely used protocols—namely, Bluetooth® (IEEE 802.15.1), ZigBee (IEEE 802.15.4), and Wi-Fi (IEEE 802.11)—are evaluated and compared. The important features under consideration include data bandwidth, frequency band, maximum transmission distance, encryption and authentication methods, power consumption, and current applications. In addition, an overview of network requirements with respect to medical sensor features, patient safety and patient data privacy, quality of service, and interoperability between other sensors is briefly presented. Sensor power consumption is also discussed because it is considered one of the main obstacles for wider adoption of wireless networks in medical applications. The outcome of this assessment will be a useful tool in the hands of biomedical engineering researchers. It will provide parameters to select the most effective combination of protocols to implement a specific wireless network of noninvasive medical sensors to monitor patients remotely in the hospital or at home.
Introduction
Monitoring of vital signs is an essential element in intensive care units, ambulatory monitoring, and emergency rooms. Medical sensors such as pulse oximeters, noninvasive blood pressure monitors, or electrocardiographic devices are currently wired to bedside monitors, which analyze, interpret, and present the patient's vital waveforms, numeric values, and alarm conditions to an interested user. 1
The focus of this study is wireless body area networks (WBANs) (i.e., networks of small, thin, light sensors distributed in, on, or around a human body with the purpose of monitoring body functions and the surrounding environment). A WBAN provides long-term health monitoring of patients under natural physiological states without constraining their normal activities 2 and allows doctors to monitor key vital signs while outside of specialized hospital areas. 3 In addition, physicians could monitor several patients remotely at the same time, instead of just one at a time, as it would be in traditional medicine. This improves the quality of care and the quality of life and allows for a significant reduction in the costs of treatment and monitoring.
Furthermore, WBANs have the potential for early detection of abnormal conditions, and by storing sensor data related to these conditions, it is possible to detect future diseases using data mining.
There are many WBAN systems currently on the market. Corventis 4 and CardioNet 5 are two examples that allow the monitoring of vital signals and cardiac abnormalities. When an arrhythmia is detected, they acquire an electrocardiogram signal and transmit it (via zLink for Corventis) to the health monitoring center. Patients who subscribe to the CardioNet service are provided real-time electrocardiogram monitoring that is recorded continuously and automatically transmitted wirelessly via an integrated cellular modem from a personal data assistant. Electrocardiograms are screened 24 h a day by central station technicians, with immediate referral to the physician for evaluation of rate and rhythm changes and/or symptoms. 6 In a related project, the Interuniversity Microelectronic Centre in The Netherlands has developed an eight-channel wireless electroencephalographic system for a comfortable ambulatory monitoring headset, 7 which transmits data in real-time to a receiver located up to 10 m from the system and even a battery-free wireless two-channel electroencephalographic system powered using body heat and ambient light, which could be used to monitor brain waves after a head injury. 8 Evidently, a battery-free system is only possible when every component of the system operates at extremely low power levels.
Other real-time wireless applications were developed for the elderly, which, in addition to detecting vital signs, can also detect falls 9 or can localize people with Alzheimer's disease, autism, dementia, Down's syndrome, or other related cognitive conditions using a radiofrequency-based bracelet 10 or Global Positioning System tracking devices. 11 There are also other wireless easy-to-use products that help monitor the quality of sleep, 12,13 snoring, apnea, and even the intensity of bruxism. 14
Patients with chronic diseases can be continuously monitored in their home environments, transferring not only the patient's medical information, but also real-time environmental information. It is possible to achieve interoperability between different WBANs that monitor a given patient and/or other surrounding environmental sensors. This kind of interoperability is only possible, however, if standard communication protocols such as Wi-Fi, Bluetooth®, or ZigBee are used. An example is the work of Gupta et al., 15 in which they have developed a data exchange platform for storing, sharing, searching, visualizing, and analyzing data from heterogeneous devices, facilitating the interaction between them.
Medical Sensor Networks
As a consequence of the increasing interest in the applications of WBANs, several survey articles dealing with different aspects of such systems have been published recently. One of the latest examples is by Jain. 16 Although this article brings into discussion aspects of WBANs that have often been overlooked, such as power consumption and interoperability, and suggests the application of context-aware sensing in WBANs, it still focuses mainly on the WBAN as a personal server-centric entity and as such discusses most of the network infrastructure from that perspective. In this work, on the other hand, we emphasize the necessity each node has to operate autonomously in order to reduce power consumption hotspots and facilitate interoperability, and as such we focus on the requirements of such architecture and the technologies that may enable it.
In fact, as opposed to most previous works, which solely discuss and analyze the requirements of individual WBANs, in this article we consider the characteristics of what we deem a medical sensor network (MSN), that is, the collection of WBANs monitoring multiple patients as well as the additional devices used for storing, transmitting, presenting, and interpreting the medical data, such as personal medical servers, network gateways, or remote medical servers. These networks consist of a large number of sensor nodes, each capable of some limited computation, communication, and sensing, operating in an unattended mode with limited energy.
17
The critical requirements of such networks are as follows: • Physical characteristics of sensor nodes: minimal weight, miniature form-factor, low-power operation, seamless integration into a WBAN, standards-based interface protocols, and patient-specific calibration, tuning, and customization.
18
• Medical data transfer privacy: data transfers require encryption of all sensitive information related to personal health.
19
• Fault tolerance: in case a sensor node stops working, a back-up node in the immediate neighborhood can take on the role of that node, so that critical measurements are not missed.
17,20
• Network quality of service: it is essential that medical data be transmitted and received without error and in a timely manner.
21
• System integration: the potential of WBANs can only be fully explored if they can interoperate securely and seamlessly. Interoperability should take place at the neighborhood level among the WBANs of a given patient and surrounding environmental sensors.
22
Ultimately, interoperability implies that it should be straightforward to use devices from different manufacturers in the same WBAN in a plug-and-play approach, that is, without the necessity of complicated configuration procedures.
23
Power Sources and Management
When a WBAN is controlled by the main processor of a mobile platform (i.e., personal server), the entire system cannot operate for long periods of time because this type of processor is not designed for continuous operation. 22 This problem can be mitigated by making the WBAN self-organizing so that the individual sensor nodes can operate without constant interventions from the personal server. In that case, the personal server would assume a more secondary role as a simple repository for the information collected locally as opposed to that of the coordinator of the network.
The main obstacle for wider adoption of wearable health monitoring is current battery technology. 22 Long-life batteries for WBAN sensors are highly desirable, especially when the replacement of the battery needs to be done surgically. To resolve this problem there are new developments in the market for WBAN's batteries. One of these is the case of printed batteries, which are especially suited for thin and flexible products like medical sensors in which they can be easily integrated. 24
Recently, the Interuniversity Microelectronic Centre has developed an economical radio chip for WBANs. The transceiver has ultra-low-power consumption (0.687 mW in receive mode and 2.5 mW in transmit mode), data rates between 64 kilobits per second (Kbps) and 1 megabits per second (Mbps), and transmission range of up to 30 m. 25
Moreover, there are already WBAN applications that use sophisticated energy harvesting mechanisms. Some common energy sources are the human body, from which vibrational or thermal energy is collected, 26 or the surrounding environment, where ambient electromagnetic fields may provide the necessary energy. 27 These technologies enable wireless sensor users to collect more data over time and offer more opportunities to operate autonomously in diverse environments.
In a WBAN, most energy-saving operations use duty-cycling approaches that periodically turn off the nodes so that they can operate in ultra-low-power modes for prolonged periods of time and be in active mode only when necessary, thereby achieving great energy savings. 28 Evidently, such techniques strongly depend on time synchronization mechanisms. For this reason it is also important to evaluate in every communication protocol which mechanisms it uses to achieve the synchronization between sensors and how effectively its wake-up and turnoff cycles are implemented.
The Federal University of Technology of Paraná's Ad Hoc MSN
At the Federal University of Technology of Paraná we implemented an ad hoc MSN in which in real-time the patient's body temperature is collected by custom sensor nodes equipped with model LM35 temperature sensors. 29 In addition, with this network it is possible to monitor the administration of intravenous substances using custom sensor devices, which use white light light-emitting diodes to measure substance flow. Any possible failure in substance administration can thus be immediately detected. 29 Information obtained from both temperature sensor and the flow sensor is routed through the network, crossing a gateway computer, to reach a data server, where the information is stored for later retrieval. This information may be made available on the Internet for remote access through a Web-based gateway application, which processes data packets received from the ad hoc network so that they can be transmitted over an Ethernet network and finally reach a Web server on the Internet.
A proof-of-concept network was deployed using an ad hoc Wi-Fi architecture. So far, initial small-scale experiments of this network have been carried out only in the university laboratory, but they have demonstrated the ability of the network to fulfill its goals. We are currently working in the improvement of this network to allow monitoring of patients' other vital signs such as heart rate and blood pressure as well as the use of environmental sensors for monitoring ambient temperature, for example. In addition, based on the conclusions presented herein, we intend to replace the Wi-Fi nodes by low-power embedded nodes that communicate using a suitable wireless communication protocol.
The ultimate purpose of the Federal University of Technology of Paraná's ad hoc MSN is to monitor patients wirelessly and send this information to a medical server, where specialists can monitor the patients and be alerted when a parameter presents an abnormal value. Figure 1 illustrates the design of the proposed network. In Figure 1 it is possible to identify three subnetworks comprising the system. The first level is formed of WBANs, one for each patient; the second level is the set of WBANs or other surrounding environmental sensors. We call this network the wireless MSN. Finally, a wireless local area network is used to connect the wireless MSN to the Internet.
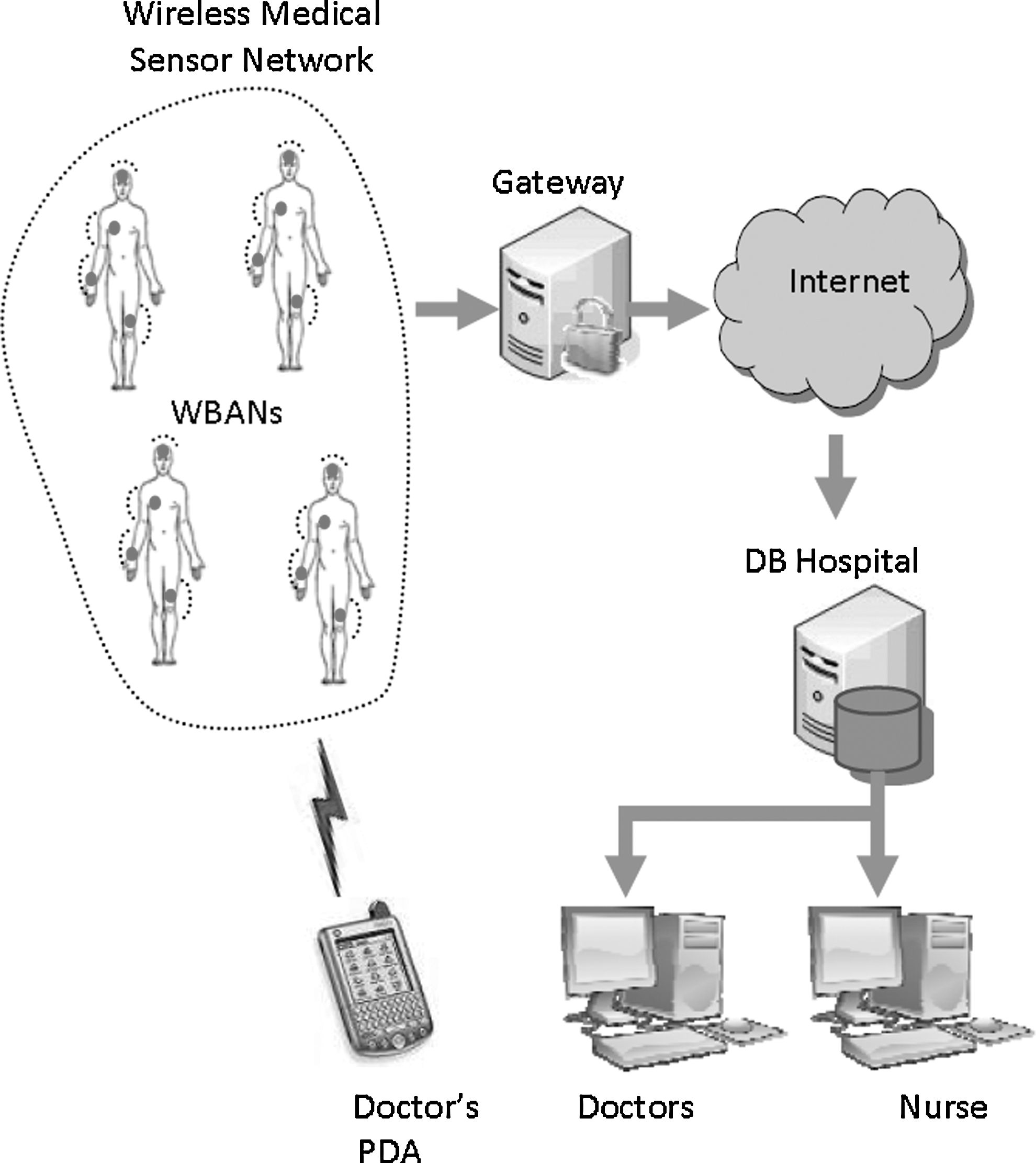
Proposed wireless medical sensor network architecture. PDA, personal data assistant; WBAN, wireless body area network; DB, hospital database.
The purpose of this article is to discuss the advantages and disadvantages of possible combinations of consumer market wireless protocols to interconnect these three networks. The protocols to be used must be secure (providing confidentiality and integrity of data), able to operate with each other, and easy to use.
Wireless Protocols
In this section we discuss some of the main characteristics of existing consumer wireless communication protocols that could be used for wireless MSNs.
IEEE 802.15.4-Based Zigbee
The IEEE 802.15.4 standard defines robust radio physical and medium access control (MAC) layers, and the ZigBee alliance defines the network, security, and application frameworks. The protocol operates at 2.4 GHz, 950 MHz, 915 MHz, 868 MHz, 780 MHz, 500 MHz, and 3.1–10.6 GHz frequency bands. 30 The capacity is 250 Kbps at 2.4 GHz, 40 Kbps at 915 MHz, and 20 Kbps at 868 MHz. Some modern devices have an indoor communication range of 50 m and an outdoor range of more than 500 m. 31
ZigBee allows the formation of mesh networks, which let all participating devices communicate with one or many others, acting as routers transferring data between devices. 20
When measurements obtained by multiple sensors must be accurately synchronized, as is the case, for example, with multichannel electrocardiogram sensors, we can use the IEEE 802.15.4 beacon-enabled mode. In this mode, the personal area network coordinator of the network broadcasts beacons periodically to synchronize devices and specify the structure of the superframe. When a device receives a beacon, it synchronizes with the superframe structure and transmits its data. 32
WI-FI—IEEE 802.11N
This standard provides secure, reliable, and fast connectivity and can be used to connect electronic devices to each other, to the Internet, and to wired networks that use Ethernet technology. It is indicated for applications such as wireless local area network connectivity, broadband Internet access, and healthcare, being currently the most widely used protocol in private households. 33 Wi-Fi can operate in the 2.4- and 5-GHz radio bands and is able to deliver data rates of up to 600 Mbps.
Bluetooth—IEEE 802.15.1
Bluetooth operates at 2.4 GHz, using a spread spectrum, full-duplex signal at a nominal frequency hopping of 1,600 hops/s. This frequency hopping adds protection against eavesdropping. The key features of the protocol are robustness, relatively high bandwidth, low latency, low cost, short range (10 m), and support for many mobile platforms. 22 This technology is indicated to provide connectivity among devices such as phones, personal data assistants, headsets, and laptop computers and is currently in widespread use in hospitals, medical offices, assisted-living facilities, and homes. However, its high power consumption, its limitation of only up to eight devices in a personal area network, its inefficient idle modes, and the long start-up times make Bluetooth an unattractive option for wearable long-term health monitoring applications. 22
The Bluetooth version 4.0, Bluetooth Low Energy (BLE) technology, provides ultra-low power consumption, a data rate of up to 1 Mbps, a range of 10 m, and a fast start-up time (few milliseconds compared to Bluetooth's seconds). 34 It consumes only 10% of the power consumed by Bluetooth, extending its battery life by sleeping and waking up when it needs to send data. 35 Time needed for connection setup and data transfer is less than 3 ms (classic Bluetooth needs 100 ms). 36 These features make it particularly suitable for latency-critical WBAN applications. 34 Although a promising technology, it is not yet supported by many devices and hence cannot yet be used in MSNs. 35
Wireless Protocols Security
Wireless sensor networks to monitor patients are becoming widely used in telemedicine. For that reason it is particularly important to protect the network against some typical wireless sensor network attacks. Attacks like sleep deprivation, the Sybil attack, or infinite loops attempt to exhaust the energy reserves of the sensors. There are other more traditional kinds of attacks where the information is intercepted by malicious users, such as eavesdropping, or even modified, by a man in the middle. Because the information travels wirelessly, attacks like jamming and sniffing are also easily performed. All previously mentioned attacks affect the transmission of information in different ways: occupying the available bandwidth of the network, consuming the energy of the sensors, and violating the integrity and confidentiality of the patient data. To protect the network from these attacks, network protocols must be secure, providing services such as encryption and authentication.
Bluetooth and Wi-Fi technologies use data encryption in lower network layers. Bluetooth adopts the full Advanced Encryption Standard (AES)-128 encryption using Counter with CBC-MAC (for encryption and authentication) and a strong 24-bit cyclic redundancy check on all packets. 36 Devices using Bluetooth must establish a shared secret used for authentication and encryption. 37
The Wi-Fi Protected Access 2 security suite, based on IEEE 802.11i, is currently the most commonly used Wi-Fi security method. It is founded on two key protocols: AES and IEEE 802.1X/Extensible Authentication Protocol, a standard widely used in corporate networks to provide robust authentication and sophisticated network access control features. It also provides mutual authentication with the preshared key in personal mode. 38
ZigBee uses AES-128 encryption and encryption/decryption in hardware and has specific security features for rapid key generation and distribution, ensuring privacy and integrity. 20 It includes frame encryption, authentication, and integrity at each layer of the protocol. 39
BLE provides session confidentiality using the AES encryption with CCM counter mode. By using a 128-bit connection signature resolving key it is possible for BLE to send authenticated data over an unencrypted channel between two devices with a trusted relationship. 35
Conclusions
WBAN technology is starting to make its way into areas such as sports and fitness monitoring, mobile device integration, rehabilitation, monitoring patients suffering from Parkinson's or Down's syndrome, monitoring patients with heart problems, or even monitoring people with sleep problems like apnea, snoring, and bruxism.
Two very important characteristics to consider in choosing the WBAN sensors are power consumption and small size. It is important to achieve balance between these two features because they are generally conflicting, meaning that the more power a system demands, the largest the volume of its battery pack must be.
Using WBANs, patients may be comfortably monitored at home while going about their daily activities, and doctors can monitor more patients simultaneously. This benefits both the patients and the hospital, providing better, more comfortable, and personalized attention, while allowing lower costs of care.
Key to enabling technology to the creation of effective WBANs are efficient wireless communication protocols. The protocols analyzed in this article are market standards and are currently in use in healthcare environments. All of them can operate on the unlicensed 2.4-GHz Industrial, Scientific, and Medical frequency band. Bluetooth and ZigBee are wireless communication technologies used in relatively short-distance environments, whereas Wi-Fi is used in longer distances. Nonetheless, with a mesh topology, a ZigBee network can cover a wide area. ZigBee is the slowest (250 Kbps), compared with Bluetooth (1–3 Mbps), BLE (1 Mbps), or Wi-Fi (600 Mbps), but ZigBee's speed is generally sufficient for monitoring medical sensors.
Although BLE features make it a suitable solution for WBAN applications, its minimal support to other devices makes it undesirable because it would not be possible to establish interoperability between different WBANs on the patient and with other potential environmental sensors. It is important that the communication protocol used by the network be standard and simple and allow seamless interoperability between them. According to the information discussed on the present article, a suitable solution for a wireless MSN, such as the Federal University of Technology of Paraná ad hoc network mentioned above, is a network setup that combines ZigBee technology in order to connect closely located devices at a low cost and Wi-Fi communication for devices located further away and with higher bandwidth requirements for aggregated data.
To summarize, although many existing wireless technologies in the market could potentially be used in large-scale wireless MSNs, 802.15.4/ZigBee seems to be the one offering the most in terms of interoperability, low cost, and power consumption while satisfying all the additional requirements of WBANs. It is fundamental to use market standards in order to leverage on the reduced costs of mass production and on the constant evolvement of widely used technologies. Evidently, as mentioned above, we cannot expect a ZigBee network to cover extensive areas between, say, a hospital and a remote medical server. In this kind of scenario, as previously suggested, one should once again leverage on mature and widespread technology by establishing connections between the wireless medical sensor network and remote servers through the Internet via local ZigBee to Wi-Fi network gateways.
Footnotes
Disclosure Statement
This project was partially supported by the Coordination for the Improvement of Higher Education Personnel (CAPES).