
Abstract
Introduction
Telehealth is defined as the use of communication and information technology to deliver health and health care services, information, and education when participants are separated. 1 The British Columbia Cancer Agency's Vancouver Island Centre (BCCAVIC) is located at the southeastern tip of Vancouver Island in the city of Victoria, BC, Canada. Half of the 750,000 people on Vancouver Island are separated from Victoria by a small mountain called the Malahat, making travel to Victoria difficult for oncology patients, especially during the winter. Therefore in 2004, two of the authors conducted (Research Ethics Board-approved) a study to look at the problems that might be associated with performing oncology consultations through telehealth. 2 Following this study, a study to understand the barriers to the use of telehealth for oncology was undertaken (supported by a grant from the Michael Smith Foundation for Health Research). 3 This study identified that patients enjoyed the telehealth experience, although oncologists slightly less so (Table 1). Oncologists primarily saw follow-up patients on the telehealth portion of the study. Therefore, one of the major barriers identified in the previous study was the reluctance of the oncologists to use the technology.
Percentage Satisfaction Scores of Patients and Oncologists with Face-to-Face and Telehealth Encounters
Our hypothesis for this observational study was that oncologists would adopt telehealth in the normal practice of seeing patients, after the modality had been introduced through a study and the positive patient response was made available.
Methods
This was an observational study. Through the Vancouver Island Health Authority Information Technology Department, telehealth units (as well as grant funding and Lion's Club donations) had been set up in the hospitals and community clinics outside Victoria.
In the cancer center, the units were set up in the outpatient area, so that oncologists would see patients via video in the normal functioning of their clinic. Following closure of the grant-funded study in September 2007, statistics were kept on the number of people seen through telehealth, the types of cancers represented, and the types of oncologists seeing the patients (radiation or medical). Any difficulties with the booking procedures and technical difficulties were also noted.
One of the concerns prior to the study was the loss of intimacy in the clinical encounter. Therefore, each oncologist was encouraged to present a very brief biography of himself or herself for both face-to-face and telehealth patients during the trial. Some oncologists continued to practice this after the trial was over.
Results
The following results were noted in Table 2: 67% of all telehealth visits consisted of breast, colorectal, or lung cancer patients. Similar to the 2006–2007 telehealth study results, colorectal cancer patients had the highest rates of telehealth encounters, both follow-up appointments (39.3%) and new patient appointments (1.5%). Approximately 90% of all telehealth encounters occurred with a medical oncologist. Nearly 97% of telehealth visits were conducted with follow-up patients. Levels of telehealth uptake for encounters with breast, colorectal, and lung cancer patients have increased by 134.6% since the 2006–2007 study. Medical oncologists conducting appointments with breast cancer patients alone demonstrated an increase of 20-fold.
Types of Cancer Patients Seen
About 80% of the medical oncologists and 50% of the radiation oncologists in the clinic have used telehealth at some time. From 2007 until the present the absolute numbers of follow-up telehealth patients have continued to increase so that now over 1,000 encounters per year are done through telehealth (Fig. 1).
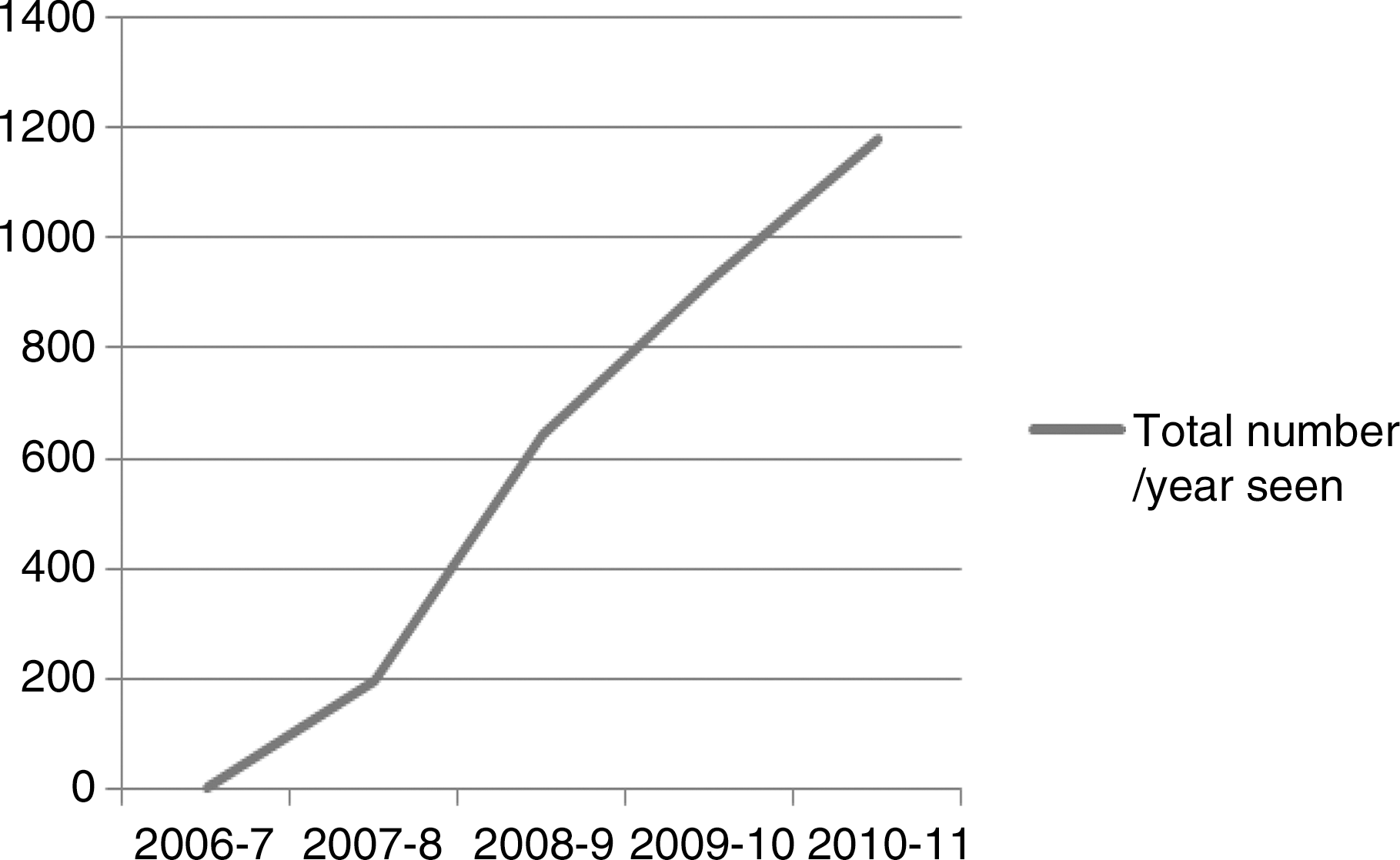
Total numbers of oncology patients seen by telehealth in the years after completion of the initial telehealth study.
Conclusions
The data we have obtained following the closure of our telehealth study 3 demonstrated that the use of telehealth increased sharply following the trial. Medical oncologists were heavier users of the technology. Medical oncologists typically have more follow-up patients and see them over a longer period of time than do radiation oncologists, who may only see a patient once after treatment. In addition, because all patients have to come to the BCCAVIC to receive radiation there is often little to be gained by seeing the patients through telehealth. It is clear however, since the usual method of new patient consultation consists of doing a history and a physical exam, oncologists wish to continue this practice, as the vast majority of telehealth visits are follow-ups.
It is noteworthy that 80% of oncologists in the clinic have used telehealth to see patients at some time. This happened within a year of the study closure. This is in contradistinction to a sister clinic within the British Columbia Cancer Agency, where telehealth is frequently used but has a much lower uptake by the majority of oncologists in the clinic. The introduction of the technology in an ethically approved study, the enthusiastic response by patients, and the placement of the telehealth units in the clinic have likely lead to the fairly widespread acceptance of the technology.
Patients rated the telehealth encounters as high or higher than the face-to-face encounters. It saved them time and money and was green. 4 So why then is not this readily adopted by the physicians? Physicians are used to performing a consultation on patients by taking a history and doing a physical examination. When we set up our study 3 we reviewed the literature to see examine the evidence for a physical exam meaningfully increasing accuracy or yield an oncology encounter. 5 –10 Most studies 5 –10 demonstrated that 71% of findings were found on history and that additional imaging studies were more accurate and effective than the physical exam in documenting recurrences or nodes. Reality today has specialists and subspecialists concentrated in major centers with ill patients sometimes traveling hours to see them. If we wish to concentrate on patient-centered care, we need to design a new system of patient encounters rather than relying on the system (advanced for its day) developed in the 1800s. 11 Telehealth is one of those modalities that can deliver specialty and subspecialty care close to home.
Footnotes
Disclosure Statement
No competing financial interests exist.