
Abstract
Introduction
Approximately 285 million people worldwide live with visual impairment. 1 Of these, 39 million people are blind (defined as best corrected vision of less than 3/60 in the better eye), and low vision in approximately 117 million people is due to uncorrected refractive errors. 2 Morever, 80% of global blindness is avoidable (i.e., readily treatable and/or preventable by known, cost-effective means). The number of blind persons in India is currently over 18 million. This estimate is 50% more than the figure of 12 million from a decade ago and amounts to approximately one-fourth of all the blind people worldwide. 3
Cataract is still the major cause of avoidable blindness in India. However, considering existing prevalence and projected incidence of cataract blindness over the period 2001–2020, elimination of cataract blindness may not be achieved by 2020 in India. 4 With the increase in cataract surgery rates, other conditions such as diabetic retinopathy, glaucoma, and childhood blindness are emerging as major causes of avoidable blindness as evidenced by recent epidemiologic surveys. 5.6 In such instances, treatment initiated at an appropriate stage can prevent permanent visual loss. Hence, a holistic approach is required to address the current situation, and concentrating on cataract blindness alone would be a limited approach.
Barriers to utilization of eye care services, concentration of ophthalmologists in urban settings, and lack of resources in terms of capital as well as adequately trained manpower are a few important reasons for the high magnitude of avoidable blindness in India. In order to overcome these hurdles, there is a need to design comprehensive yet sustainable eye care programs that must be easily accessible to the rural and underprivileged population. In addition, these must ensure quality, especially in terms of screening vision-threatening diseases, referral services, and affordable, rapid rehabilitation of refractive errors.
Teleophthalmology has unlocked a new frontier in screening of common ophthalmic diseases and can reduce the need for travel and provide access to a superspecialist. Imaging modalities aid diagnosis in a wide variety of clinical scenarios by virtue of which ophthalmology lends itself easily to telemedicine. If utilized to its full potential, it promises that no region of the world will be too remote or too poor to receive high-quality medical care. Screening of diabetic retinopathy has been revolutionized by the advent of teleophthalmology. 7,8 Recently there has been experimentation with some other conditions such as screening of retinopathy of prematurity and orbital/adnexal diseases. 9 –11 The concept of mobile teleophthalmology is a new one and has not been explored to its true potential as yet. Besides a report on teleophthalmology screening for diabetic retinopathy through mobile imaging units within Canada by Boucher et al., 12 there are no substantial data detailing application of teleophthalmology.
Sankara Nethralaya (SN) is a tertiary eye care center in south India and is committed to patient care, ophthalmic research, and training at all levels for over three decades. With the aim of providing comprehensive and quality eye care to the rural population, a unique program implementing a mobile teleophthalmology unit was designed at SN with the help of the Indian Space Research Organization (ISRO) and launched in 2003. The scope of this venture has expanded in terms of expertise, equipment, and successful partnerships.
This study gives an overview of the current process of conducting comprehensive eye camps with emphasis on teleophthalmology consultation as well as reviews results of this endeavor over the past 1.5 years.
Subjects and Methods
Retrospective chart review of all the camps were done as a part of the SN rural teleophthalmology project during the period of April 2009–September 2010. This study period was chosen as camps were carried out at regular intervals every month and good medical records were available for documentation. To successfully carry out a comprehensive eye camp, one needs a good understanding of the various epidemiologic aspects of blindness in the targeted population, skilled manpower, and enormous logistic/technological support. Teleophthalmology camps involve the following activities: identifying the camp location, planning the camp, conducting eye camps, teleconsultation, providing low-cost spectacles to the rural population, referral of surgical cases to the base hospital, and conducting counseling/awareness programs.
Identification of Camp Location
Villages over four different states in India were chosen to provide comprehensive eye examination under the directives of the head of the department of teleophthalmology. Choice of villages depended upon certain important factors, with distance from the base hospital being an important one (within 150 km of the base hospital in the particular state). Prevalence of district-wise blindness as published by the District Blindness Control Society (DBCS) of India was also considered. The DBCS is a government organization, and its purpose is to plan, implement, and monitor all the blindness control activities in the district under overall guidance of the state/central organization for a national prevention and control of blindness program. Economic feasibility was also an important factor in deciding the camp site. After the districts and villages were identified, the permission of the head of the DBCS was obtained in all states.
Planning the Eye Camp
Once the villages were identified, detailed census information about the districts/villages and amenities of the villages was used in planning the camp. The camp team included four social workers (one of whom worked as the camp planner), four optometrists, one optician, and a driver who helped in crowd management at the camp site. If electronic medical registration (EMR) was possible at the camp site, two more information technology team personnel were added. They carried six tablet personal computers/laptops, one server computer, and one wireless modem to interconnect these computers along with them to the camp site.
Role of social worker
After a village was selected for screening, a social worker, in charge of planning, went to the village 2 months prior, to lay out the program details. He had a preliminary meeting with the village heads to explain the purpose and benefits of the teleophthalmology program and gain their support. The social worker also interacted with heads of local non-governmental organizations (NGOs) and other potential camp organizers to provide food and manpower support for the planned activities. The planning social worker also identified the locations for holding camps such as high schools with large open grounds. The feasibility of the teleophthalmology unit to enter such venues was also taken into consideration as per the requirement of each mobile unit. The social worker was also responsible for publicizing the camp schedule in the villages. Once the heads of the villages and the organizing NGOs were in agreement of the camp, a “letter of interest” was signed by the camp organizer. Based on this, a tentative camp schedule was prepared by the social worker.
Another visit was made to the village by the same social worker 1 month prior to the camp, to finalize the visit of the team, location, and the people who would benefit from the camp. Patients were first identified by door-to-door enumeration or prepublication with handbills and auto announcements and informed of the day and date of the arrival of the mobile unit by personnel from SN and the sponsoring NGO. At the camp site, the social workers were responsible for patient registration, counseling patients, spectacle billings, awareness programs, and general camp management.
Publicizing the camp schedule in the villages
Publicity means used were as follows: 1. Banners displayed at strategic locations 2 weeks before the camp 2. Public announcements using microphones mounted on autorickshaws (small three-wheeler vehicles), 1 or 2 days before the camp 3. Handbills/leaflets for those registered at the camp clearly highlighting the features of the camp in vernacular language so that they could clearly understand the features of the camp
Role of NGOs in camp organizing
NGOs were needed to organize the camp in the following ways: 1. Win the confidence of the local community to participate in the program 2. Help the SN team with sponsorship for the camp related prepublicity expenses, like printing banners and handbills and advertisement costs 3. Sponsor lunch for the team during the working hours of the camp
Conducting the Teleophthalmology Camp
Patients were registered by social workers with the support of local volunteers in the EMR. This was not possible in all camps because of lack of electricity backup. Patients registered on the EMR were then given printed identity cards. If EMR was not possible, we issued paper registration cards, and this patient information was entered into the SN server on returning from the camp site.
This was followed by refraction using an autorefractor (model KR 8900, Topcon, Tokyo, Japan) and comprehensive clinical examination by a trained optometrist including case history, best subjective correction on logMAR charts or Snellens distance charts, slit lamp examination, pupil reaction, cover test for distance and near and intraocular pressure measurement using applanation tonometry. Fundus images were obtained for all patients using a non-mydriatic fundus camera (model TRC NW 200, 5 megapixels, Topcon) by the optometrist. In the event an abnormal finding was detected in the fundus image, a dilated retinal image was obtained and sent to the ophthalmologist at the base hospital (SN) for evaluation. Figure 1 shows the work flow at a representative camp site. All patient records were converted and stored on the EMR format at the base hospital.

Work flow at a teleophthalmology camp site.
Teleconsultation
Teleconsultation indications
Indications for teleconsultation were as follows: 1. Unexplained visual loss 2. Glaucoma suspects and glaucoma cases 3. All patients with diabetes and hypertension 4. Strabismus cases 5. Optic nerve head abnormalities seen on fundus imaging 6. Infections of the conjunctiva or cornea 7. Uveitis and retinal pathologies 8. Cases where vision did not improve with pin hole and best possible refraction, other than cataract, and cause of visual loss is undetermined 9. Any history of previous ocular surgeries associated with visual impairment 10. Any case where either the optometrist has a doubt or if the patient would like to interact with the ophthalmologist at our base hospital
The mobile teleophthalmology unit
The mobile unit had three compartments. The front portion of the unit was for the driver and staff during travel to remote areas. The middle portion held the videoconferencing apparatus, including an IP satellite console, antenna controller, eight-port network switch, access point, P-4 computer with 1GB ram and 40GB hard disk with 10/100 network card or Wi-Fi adaptor and flat bed scanner and ink jet printer, Sony™ videoconferencing camera, and Prognosis PACS cum telemedicine software with Picture Grabber card, PC to video converter, 2-KVA uninterruptible power supply, and cables. Software packages used were Windows XP/MS Office Package for the PC and Windows 2003 for the server (Microsoft®). Upload and download speeds available were approximately 256–384 kilobits per second (Kbps) (15 frames/s). This part of the bus was fully air conditioned for optimal performance of the equipment. The rear portion of the bus was for storage of one additional set of ophthalmic equipment, pamphlets, chairs, cleaning equipment, and luggage of the teleophthalmology team; it also housed two 5-KVA diesel generators (for captive power supply). Equipment outside the bus included a satellite dish antenna (i.e., very small aperture terminal facility) on top provided by the ISRO. Figure 2 shows mobile units used during the study period. In Maharashtra, camps were conducted near the village resource center of the M.S. Swaminathan Research Foundation, which was equipped with a satellite dish provided by the ISRO. Teleconsultation was done using these satellite dishes. Hence, a teleconsultation mobile unit was not required.

Teleophthalmology mobile units.
The process of teleconsultation
After the initial basic examination by the optometrist, patients requiring teleconsultation were identified. External photographs were taken using a digital camera having a resolution of 3.2 megapixels (Canon USA Inc.). Photographs were also taken using the slit lamp imaging system, which provided 96 pixels/inch resolution (Appaswamy Associates, Chennai, India). After pupillary dilatation, a single 45° digital fundus photograph centered midway between the center of the macula and the disc was taken with the Topcon TRC NW 200 camera. These images were converted to Digital Imaging and Communications in Medicine standard and transferred to the base hospital by a satellite link using the very small aperture terminal with the store-and-forward technology and also real-time videoconferencing when possible. The transmission rate ranged from 256 to 384 Kbps. At the base hospital, an ophthalmologist evaluated the photographs and clinical data provided. Real-time interaction with the examining optometrist as well as the patients was then established using the videoconferencing system (Sony, Japan). The examining optometrist then carried out any further examination felt necessary by the ophthalmologist. Medical treatment advised was then dispensed in the outreach facility, and patients needing further investigations or surgical treatment were transported back to the base hospital.
Providing Low-Cost Spectacles
An additional van donated by Essilor, India accompanied the mobile unit in all camps and was responsible for housing the spectacle dispensing unit. It also had three compartments. The first was for the driver and any other personnel travelling to the camp site. The second compartment was air-conditioned and held the Delta Edge lens grinding unit, a frame warmer for making spectacles, and a lensometer. The third compartment had a spectacle display unit and space for storing stock of plastic lenses provided by Essilor, India. After the comprehensive eye examination, patients were provided spectacles on the spot for nominal charges.
Referral of Patients to the Base Hospital
All patients with significant cataract and other disorders requiring surgical intervention or other investigations as deemed fit after teleconsultation were issued registration slips and advised to attend the appropriate subspeciality clinics at the base hospital without any charge.
Awareness Activities and Counseling
Short PowerPoint (Microsoft) presentations and banners were displayed at the campsite at the end of the day to spread awareness among people. A few short films on primary eye care, cataract, glaucoma, diabetic retinopathy, and eye donation were also screened whenever possible. These presentations and films had popular citizens of the community such as film actors and politicians delivering important messages to the audience to make an impact. All through the program, our refractionists and social workers were available to answer questions. The number of people who benefited because of attending these activities was recorded.
Results
Over the 1.5-year study period, in total, 872 camps were conducted, covering villages in 25 districts over four states in India using three different teleophthalmology mobile units. Electronic medical records were maintained in about 10% of the camps. Three districts (Kanchipuram, Vellore, and Thiruvallur) in the state of Tamil Nadu as well as three districts in the state of Andra Pradesh (Chittor, Nellore, and Cuddapah) were covered by the same teleophthalmology mobile unit, while other mobile units were dedicated for Karnataka (six districts), Maharashtra (Vidharbha Region), and Rameshwaram. Teleophthalmology camps were comprehensive eye examination programs and not merely screening camps. Because of the rigorous work-up involved in comprehensive ophthalmic evaluation for each patient in this program, each optometrist was able to see about 35 patients in a day. In most instances, each unit had four optometrists, enabling them to see approximately 140 patients per day.
In total, 54,751 patients underwent comprehensive ophthalmic evaluation during the study period. Out of these, 31,951 patients (58.4%) had some form of visual impairment (presenting visual acuity <6/18), and 1,397 patients underwent specialized teleconsultation with an ophthalmologist. The commonest cause of visual impairment was uncorrected refractive error, seen in 18,911 subjects (59%). Cataract affected 30.3% and diabetic retinopathy affected about 3.3% of patients with visual impairment. Figure 3 shows prevalence of diseases contributing to low vision in our patient population during the study period.
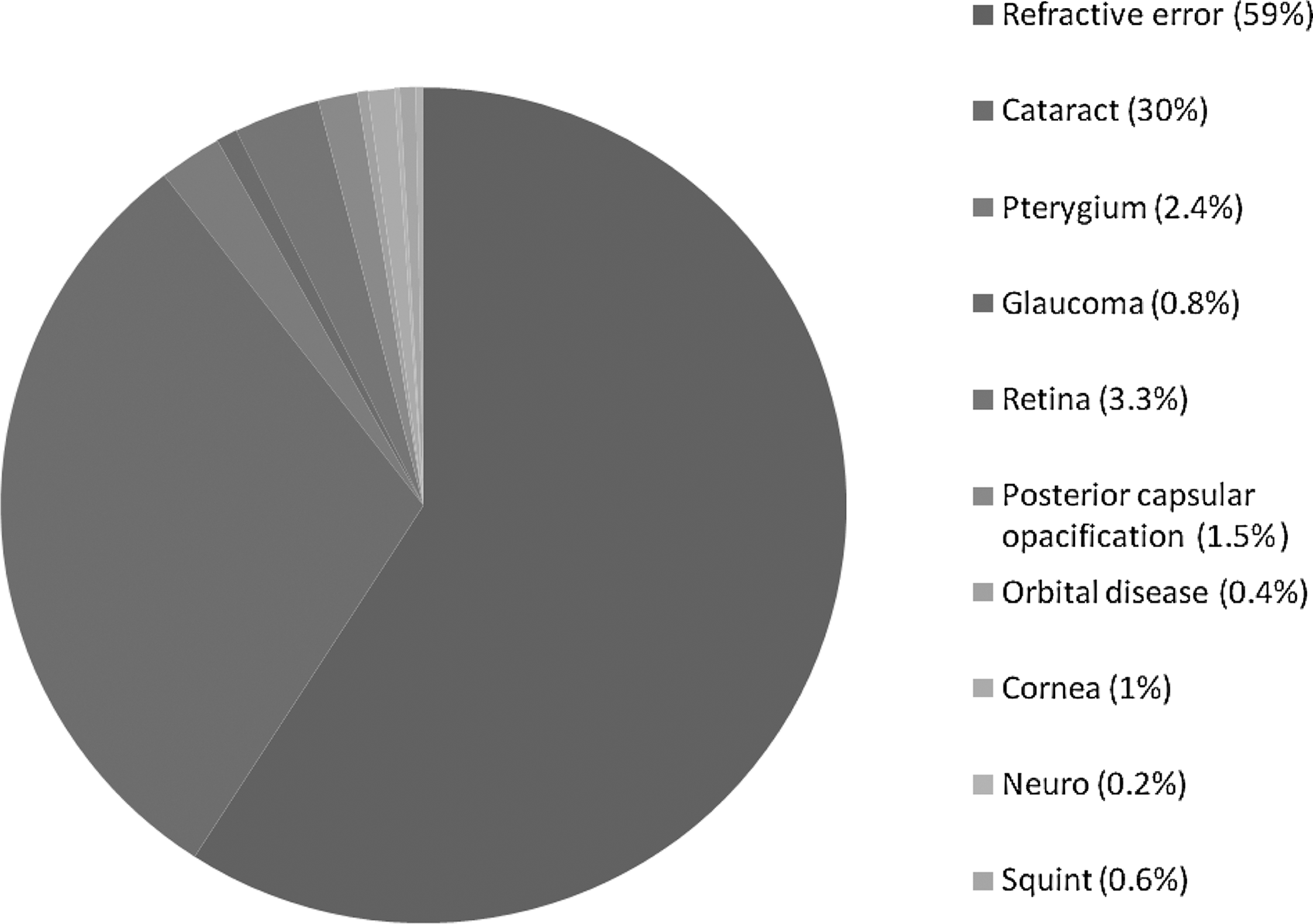
Prevalence of diseases contributing to low vision over 1.5 years.
During heavy rains with cloud cover, image quality was suboptimal in terms of image quality and transmissibility. As good-quality access to satellite connectivity requires fields open to the sky, camps held in rural areas with dense forestation led to poor satellite connectivity and suboptimal images. During such events, the images were stored and transmitted to the base hospital the next day, and the medical advice was communicated to the patients.
Discussion
Telemedicine applied to ophthalmology may represent a paradigm shift in screening for common but vision-threatening diseases that have the potential to pose major public health problems. Ophthalmologists are accustomed to diagnosing diseases asynchronously from two-dimensional colored imagery or angiograms. Thus, teleophthalmology lends itself easily for wider applications.
Comprehensive eye care delivery seems to be a natural progression from mere screening, which, most of the time, is aimed at target populations. A complete eye examination coupled with skill in obtaining high-quality photographs reduces chances of overlooking diseases that may be quiescent or at an early phase. Our data show that refractive error was the commonest cause of avoidable blindness in the population. Most population-based studies report cataract as the commonest cause of avoidable blindness in India. 13,14 However, these studies adhere to opportunistic screening and target population above the age of 50 years. Our study did not have these limitations and represents a cross-sectional survey of the situation in the community. We have encompassed four states and examined over 50,000 people, and our data may provide an overview of the current status of avoidable blindness prevalence over the country across all age groups. However, larger-scale studies covering larger geographic areas would be required to corroborate these findings.
From a population point of view, teleophthalmology greatly reduces travel time and capital, thereby facilitating utilization of eye care services even in the remotest of villages where such services are not freely available. Indeed, such activities are a boon to the underprivileged. Considering that refractive errors constitute a major portion of avoidable blindness, providing spectacles on the spot at affordable prices has the potential to reduce blindness prevalence dramatically. We were able to provide spectacles to nearly 30% of patients requiring them at the camp site itself.
The SN teleophthalmology project has been instrumental in screening a larger number of the patients across wide geographical areas of India. The integration of NGOs, ophthalmologists, and imaging technology was critical in establishing the model of teleophthalmology-based comprehensive eye care delivery described in this article. It has enabled us to maintain a high quality of care in addition to the quantity. Previous reports from our center have reported the cost-effectiveness of this model in screening for diabetic retinopathy and adnexal diseases. 15,16 We found these camps to be very efficient in detecting patients with sight-threatening diabetic eye disease such as proliferative diabetic retinopathy, severe diabetic macular edema, or a combination of these. 17 Patient satisfaction was also a vital factor for the continued success and support of our comprehensive camps. 18
Difficulties in implementing this model include obtaining high-quality images and compressing/digitizing them. Handling/maintaining imaging systems has a high learning curve and requires considerable expertise on the part of personnel at the camp site. Starting a mobile teleophthalmology unit requires considerable capital investment (approximately $96,000 U.S.) and good logistical support to maintain function at desired levels. Currently, there is little published outcome research that assesses the reliability of mobile teleophthalmology. More published results will help establish criteria, guidelines, and standards for teleophthalmology. Experience gained can be shared with the industry to adjust teleophthalmology system designs.
In conclusion, the model described in this article is efficient in delivering comprehensive eye care to the rural population of India. By comprehensive eye examination, we have adhered to the dictum of “prevention is better than cure.” If other governmental organizations and NGOs were to replicate this strategy, we might be able to achieve a reduction in the prevalence of avoidable blindness in the developing world. In addition to eye care delivery, the potential for distance learning, continued education, and clinical trial collaboration are some applications of teleophthalmology that should be explored in greater detail in the future.
Footnotes
Disclosure Statement
No competing financial interests exist.