
Abstract
Introduction
With the striking evidence of a world population growth from 2 billion in 1940 to 7 billion in 2011, to bring about the inclusion of a huge percentage of previously excluded human beings from a modern health system and a growing healthcare professional deficit, the only way to reach the United Nations Millennium Goals is through the use of current advances in information and communication technologies (ICTs). The massive use of the Internet, nowadays available to the vast majority of people and just declared by the United Nations as a human right, is the cornerstone of our telemedicine experience.
Many countries have reported the development of telemedicine programs and projects that account for outstanding publications and well-documented plans that have never been implemented, precluding the most needed from the benefits telemedicine can bring. Our experience arises from the bottom of the healthcare pyramid and from the most distant and isolated parts of the jungles of Venezuela to reach the highest healthcare level.
Background and Experience in Maniapure for Over 15 Years
Our experience originated in the Maniapure Project 1 in the 1960s when family adventure trips brought us to this distant region of extraordinary beauty. Early visitors established a close relationship with the local population (indigenous groups and native “creoles”) by providing support for educational purposes and aid to cover some of the population's basic needs. Since then healthcare professionals visited the region during summer vacations, which enabled regular seasonal healthcare to be provided.
In 1995, a small clinic and a physician serving a mandatory rural year began activities, and they were hired to provide year-round medical care under the umbrella of the Maniapure Program, currently known as Fundación Proyecto Maniapure (FPM). 2,3
One of the basic and innovative features of the Program was the relevance of telecommunications to provide support to the remote physician from distant urban high-level health centers:
1 From 1995 to 1997, two-way radio communications was used.
2 In 1997, the satellite phone connection was introduced (enabling fax transmission of images, graphics, electrocardiograms, etc.).
3 After 1999, the availability of the satellite Internet connection was a turning point.
With the use of the information superhighway, the remote physician overcame the feeling of isolation through connection to his or her peers and subspecialists. Additionally, availability of a permanent physician made the center attractive to senior students in health-related careers such as medicine, dental care, nutrition, and laboratory clinicians, who are required to serve a 16-week internship. By mid-2011, over 1,100 students have served their internship at these centers.
Materials and Methods
Shortly after Maniapure's telemedicine services became news, CANTV, Maniapure's telecommunications ally, presented that experience at the International Telecommunication Union's (ITU's) annual conference in Geneva, Switzerland. The Project was perceived as a success. As a result, the ITU donated two additional satellite antennas to be used for the same purposes in two of Maniapure's neighboring locations. Leaders of other indigenous groups from the Canaima National Park, specifically from the Kamarata community, a region very distant from Maniapure, requested information and support to establish their own telemedicine system. This initiative involved meetings with 11 indigenous group leaders.
Using the methodology we had had in place for over 10 years, we learned that this could be reproduced in just 3 months. In a short time, four new telemedicine points were established: in the towns of La Urbana and El Guarray, within the Maniapure Region, as well as in Kamarata and Wonken, within the Venezuelan Guyana.
In total, 23 sites (Fig. 1) have been established and are operating with the approval of the regional and national health authorities.

Map of Venezuela indicating rural telemedicine sites.
Project Operation Model
The Maniapure Program developed an effective store-and-forward solution for:
• Improving healthcare standards by enhancing access to more experienced subspecialty physicians from rural populations that otherwise did not have access.
• Facilitating recruitment of healthcare professionals by eradicating the feeling of isolation with availability of an Internet connection.
Our operational model (Fig. 2) is focused on three healthcare levels 4 :
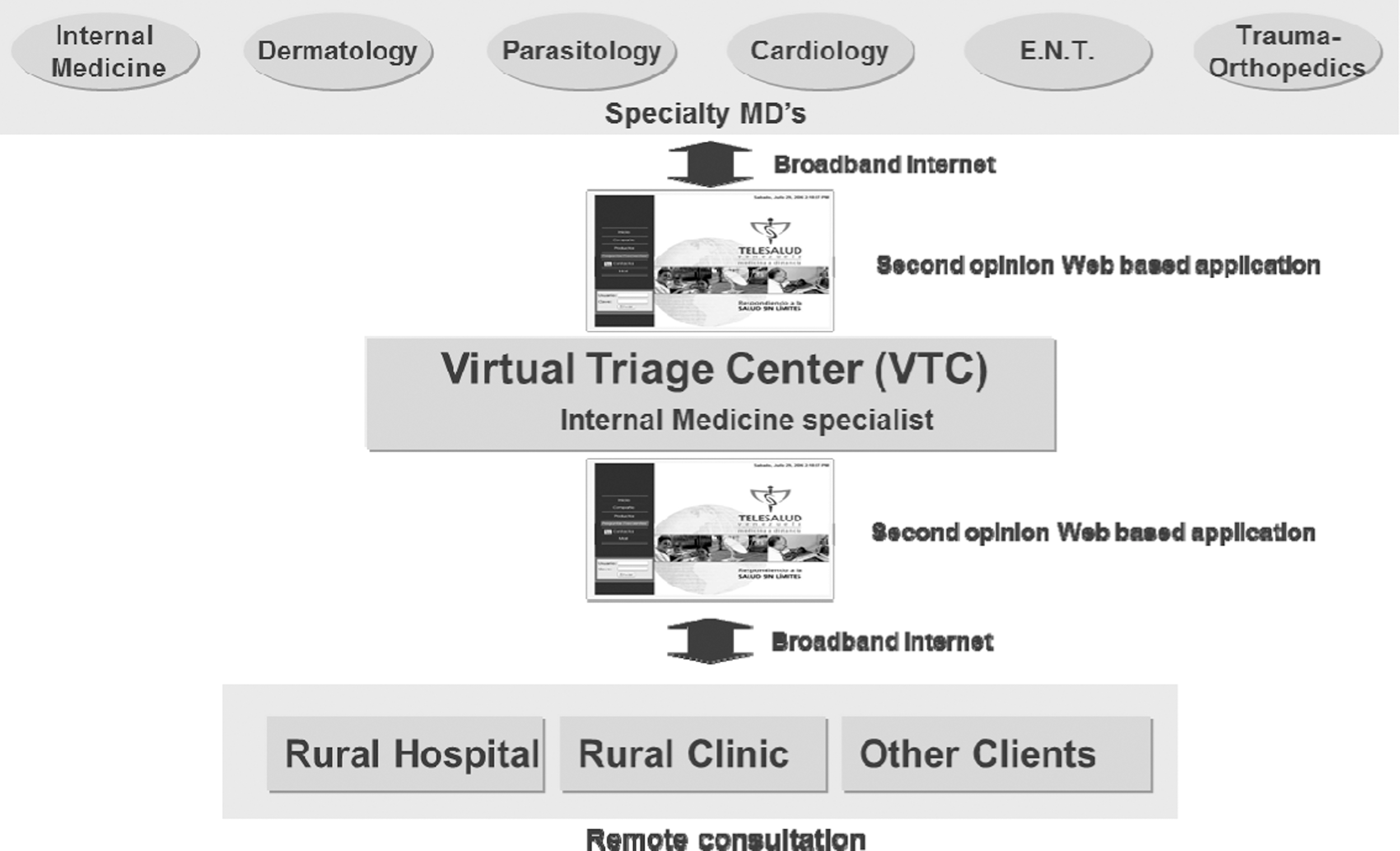
Healthcare levels in our operational model.
1. A remote consultation coming from distant healthcare centers or rural outpatient facilities where an inquiry for a particular medical consult is generated and forwarded to the virtual triage center (VTC).
2. VTC (contact center) Internet-based consultations. Internist physicians or registered nurses at the VTC receive the inquiry, examine the case, and provide adequate advice. If they are unable to give an appropriate answer, the inquiry is forwarded through the Web to the subspecialty physicians.
3. Specialty M.D.s, who can be reached online wherever an Internet connection is available, provide adequate medical advice to the remote primary-level healthcare provider through the VTC.
To fulfill the needs for reliable, secure, friendly, and recordable communications, a store-and-forward Web application was developed in a 2-year effort.
As technology has advanced, more medical capture devices became available and can be attached to a remote computer (Fig. 3). All data being captured are sent to the VTC through a broadband Internet connection. The better the information received, the better the diagnostic scope and recommendations.
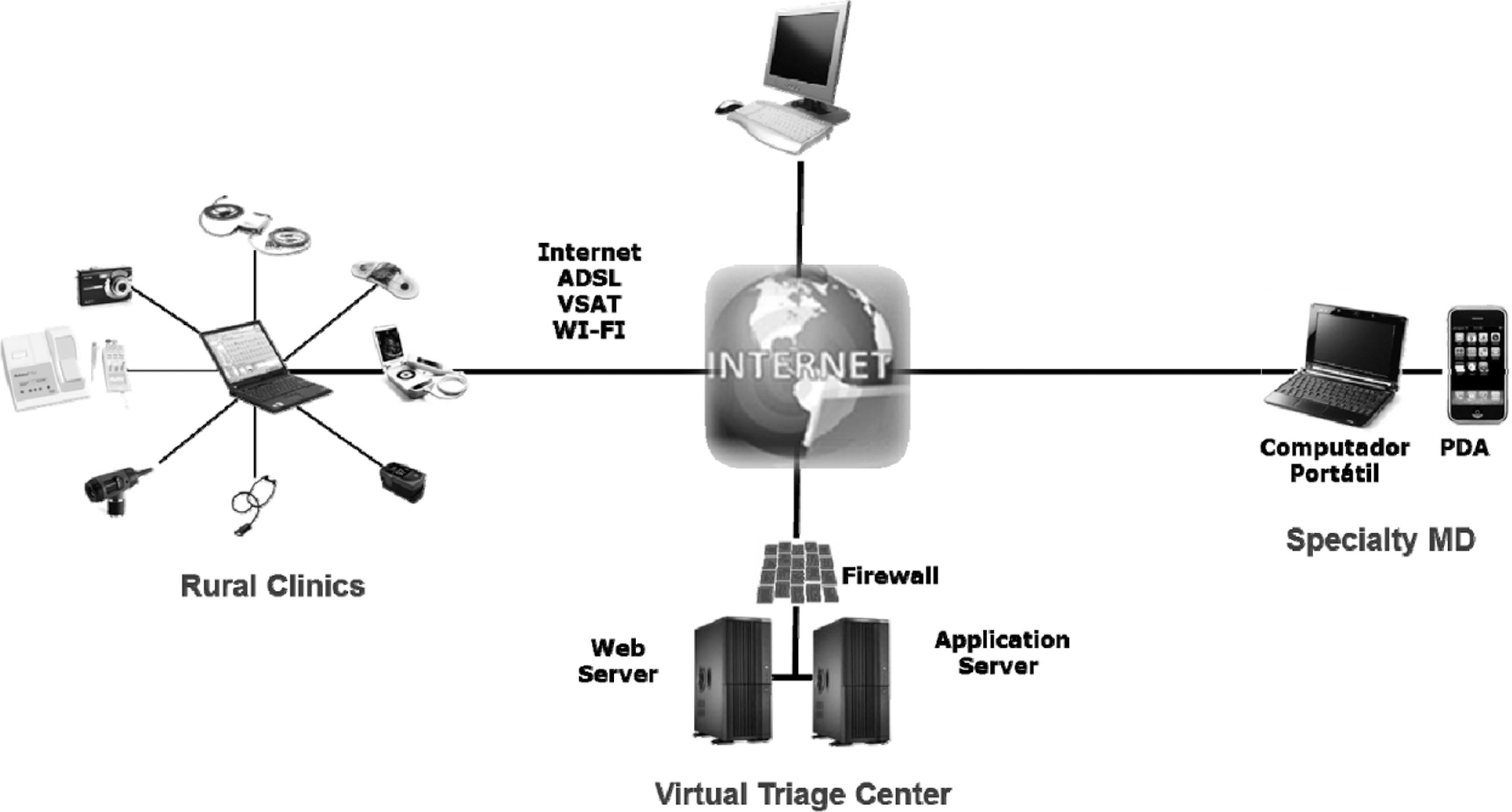
Types of medical data captured and sent over the Internet to the virtual triage center.
Our organization (Telesalud Inc.) currently provides over 20 subspecialty consultations: dermatology, pediatrics, hematology, dental medicine, general and plastic surgery, pneumonology, internal medicine, nephrology, gynecology/obstetrics, cardiovascular and thoracic surgery, ear/nose/throat, cardiology, tropical medicine, ophthalmology, gastroenterology, trauma/orthopedics, neurology, infectious disease, urology, and radiology. Our experience has shown that any subspecialty can be included once needed. The most common teleconsultations are dermatological, which represent 40% of our cases.
Search for Sustainability
After a 10-year telemedicine experience at Maniapure and a 1-year experience at four additional locations, FPM became aware that there were not sufficient funds even to operate ideally within the Maniapure Region. Furthermore, to continue spreading the telemedicine initiative to benefit other populations, a self-sustainable organization was required. 5 –7
This led to the creation of the TeleSalud Corporation, whose objective was to reproduce the Maniapure telemedicine initiative with funds coming from the social responsibility agendas of public and private entities.
The telemedicine system stakeholders (Fig. 4) include:
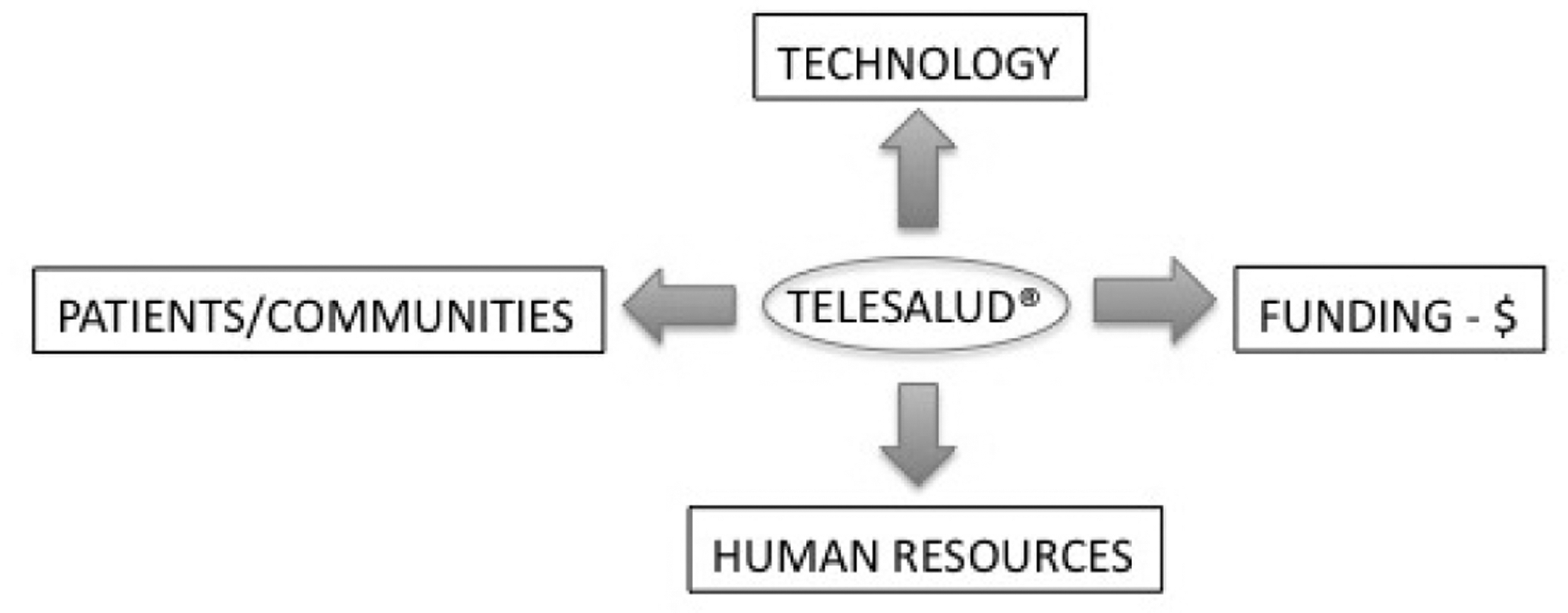
Telemedicine stakeholders.
1. Patients or communities in need of healthcare. Patients are never scarce. This can be easily found in our Latin American societies and many other countries of the world.
2. Technology. Technology evolves through giant leaps in the areas of ICTs. It is purchasable and continuously becomes more available and affordable.
3. Human resources. Human resources are available from our universities, which offer high-quality education and training in ICT and healthcare. Telemedicine staff require training and must be encouraged to make this technology “their own.”
4. Funding. The operation of the overall system is indeed limited by the lack of funds. In the 21st century, organizations committed to socially responsible behaviors are found everywhere. Building credibility and operating with transparency make funds available.
FPM, as a telemedicine service provider, maintains a close interaction with the telemedicine system stakeholders and offers training, maintenance, and follow-up limited to the Maniapure Region. TeleSalud provides telemedicine services in all other regions.
Results
The lack of physicians, forecasted in the 1970s, 8 has grown to a deficit of almost 3 million worldwide. Furthermore, physicians are not proportionally distributed among the global population; matters of concern are migrations for financial, technical, and political reasons that decrease the healthcare capacity of the country emigrated from.
Trying to find solutions with the use of ICTs we have learned some lessons:
Effects of Geography
Our telemedicine solutions render best results in regions or countries with large areas, that are underpopulated, and where geographical features or distance make healthcare difficult to deliver. These areas are common in Latin America. Moreover, its population lives in poverty and cannot afford to travel for specialty consults so the population excluded from the healthcare system is increased.
Stakeholders
The end user, whether an individual or a community, is the most important stakeholder and driving force that keeps the system running. If there is no organizational group to make the telemedicine system “its own” by promoting its operation and verifying the proper use and maintenance of the hardware, the chances for the system to fail are high.
Numbers of Patients Who Need Teleconsults
Just a small number of patients from a remote healthcare facility require telemedicine consults (Fig. 5).
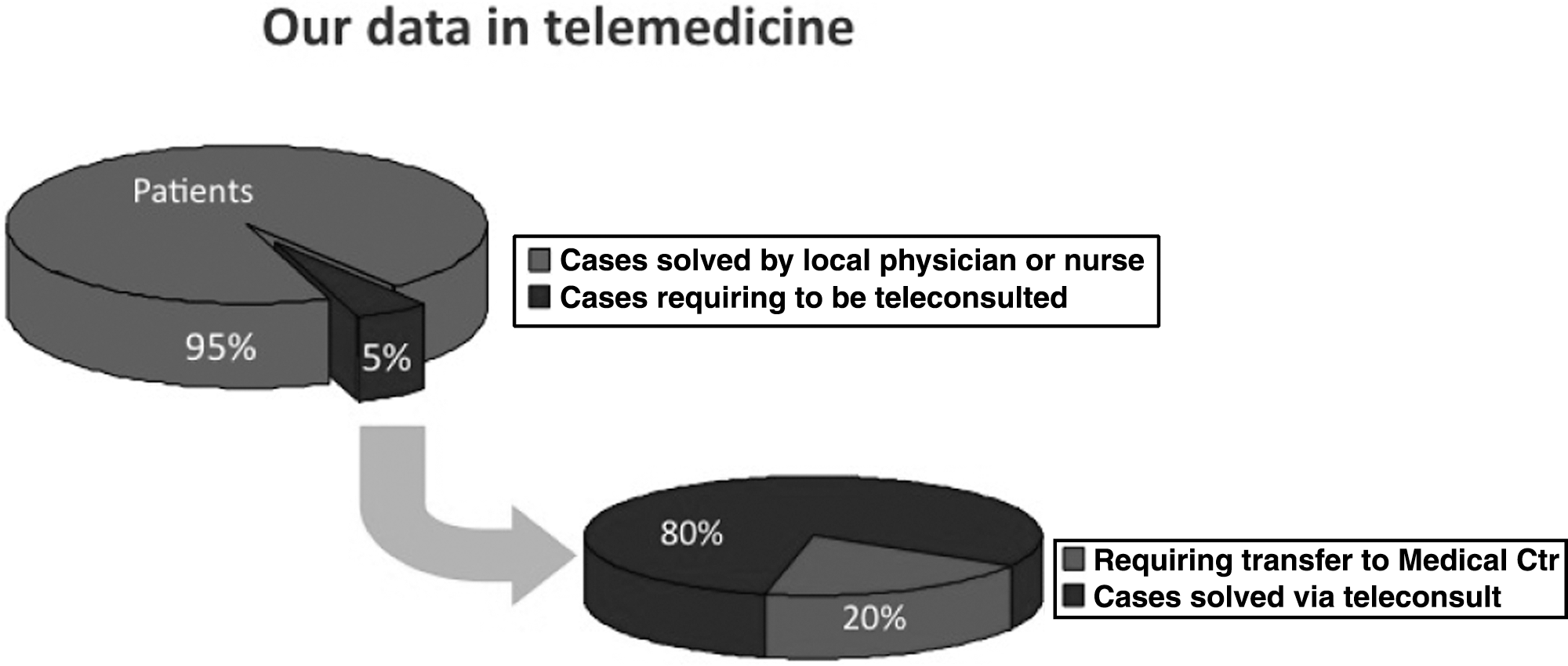
Distribution of our data used in telemedicine consults.
In our most rural and remote experiences the population ranges from 4,000 to 10,000 people. Maniapure has nearly 10,000 population; Kamarata, Wonken, and La Urbana have approximately 5,000 each. Over the last 10 years, we have surveyed the frequency of teleconsults (second opinion/referrals requested from one general M.D. to a specialty M.D.) performed by our rural physicians in the Maniapure Clinic and other active rural centers where the numbers of medical consults average 400 per month. From these original medical consults, the numbers of teleconsults have ranged from 15 to 25 per month. This yields an average of 4–6% of patient visits that require a specialty medical consult by these young, well-trained doctors. Once the Internet is available to them, many initially consult their peers in other regions and/or their teachers by mail with images and data; 50% of their original 15–25 monthly teleconsults are performed initially through our Website where consultations and answers are documented and registered as a formal service. By mail, we cannot keep track of what questions are asked or how they are answered. We keep working on that process to increase consults through our formal Website from the beginning of any new telemedicine location.
We conclude that 95% of the patients are given adequate care by the primary healthcare provider, whether a physician or other healthcare professional. Nearly 5% of the cases may not be diagnostically or therapeutically clear to the primary healthcare provider, requiring referral to the VTC with access to updated information or to a specialty physician. With the opinions of the VTC and specialty physicians, 80% of teleconsults may be given proper care locally, and 20% require traveling to a higher-level healthcare center such as a hospital. If so, only 1–2% of the total number of patients require transportation; all other cases may be cared for locally, which results in huge savings in terms of travel.
Telemedicine Services are Often Underused
Resistance to change is commonly seen among healthcare providers, particularly physicians, who tend to believe that they are “doing it right” and “technology offers little help.” Motivation and training on teleconsulting are critical aspects that must be part of a nurse's, paramedic's, and rural physician assistant's extended training, as they are usually powerful “motivators” for physicians to use this technology. Being the first to witness results, these professionals are often enthusiastic about the system. 9
Proper Spaces to Facilitate the Healthcare Deliverer's Work are Required
The telemedicine computer, scanner, and camera must be located in the examination room. If they are located at a distance, the volume of teleconsultations will be low, and usage will most likely cease.
Teleconsulting May Increase Consult Time by 50–100%
Usually people not familiar with the telemedicine system say that “telemedicine is a computer-based process that can be done in no time..so do it in your spare time!” If a case raises a doubt for a physician or healthcare provider, he or she will need to “reorganize” his or her thoughts, re-examine the patient to confirm the first impression and/or take good-quality images, and then complete the relevant consult forms. This is a time-consuming process. Nevertheless, it is important to point out that such additional time may result in huge transportation savings, improved medical care, and an increase in the efficiency of the main healthcare system.
Adequate Compensation is Required for the Telemedicine Providers
Staff from a healthcare facility and a VTC, as well as specialist physicians, should be compensated for their work. Before the introduction of advances in imaging techniques (computed tomography, magnetic resonance imaging, and cardiac catheterization laboratories), there was no time or space for them. This has changed, and today special rooms are available, and staff is hired specifically to operate these systems. Telemedicine is no exception and must be constructed like any other segment of the healthcare system. It is hard to imagine a hospital or healthcare facility that will not benefit in the near future from the use of ICTs to optimize patient management and improve cost-effectiveness.
Discussion
The global changes in healthcare are secondary to population growth and insufficient numbers of healthcare professionals. First world countries are not spared, and reports from the United States forecast a shortage of 130,000 physicians by 2025, 10 and currently there are reports showing limited access to specialist care in many regions. 11
The physician shortage is due to other various reasons, such as
• People earlier excluded from the healthcare system are now part of it, and the population's life expectancy has increased.
• The physician/patient ratio has lowered and so has the number of proportional specialty physicians.
Given the circumstances and the knowledge and expertise of each specialty physician, these specialists should be available to as many patients as possible. The use of ICTs seems to be the best way for specialty and subspecialty physicians to reach patients, regardless of their location. The VTC concept (contact center) has enabled a network of specialty physicians to interact with previously excluded communities and patients. More recently, in alliance with pharmaceutical companies, focus has been placed in suburban communities to provide specialized healthcare to overpopulated, low-income suburbs commonly seen on the outskirts of Latin American major cities, whose population is excluded from the main healthcare system.
Telemedicine Application on a Regional Scope
Many Latin American countries have set up expensive, aggressively advertised telemedicine systems that include well-equipped auditoriums occasionally used for online conferences with universities or multilateral agencies, bearing no benefit to the persons in need of healthcare.
Current technology enables management of diagnostic images such as computed tomography scans and robotic surgery. Such investments are made without considering the cost-effectiveness of caring for more easier-to-cure diseases such as tropical diseases, parasitic infections, and malaria. Telemedicine has an important place in prevention and cure in the tropics.
Both patient groups—those needing sophisticated diagnostic or therapeutic tools and those who need basic primary care—deserve optimal medical care and advanced technology, but public administrations should address the use of ICT to provide healthcare to the least protected population. Governments have the responsibility to provide adequate healthcare to the general population, and the best results are usually achieved through collaborative work with the public and private sectors of the society. 12 –14 Since Day 1, our telemedicine model has joined efforts with regional and national health authorities and has contributed with the State's sanitary and health policies.
Those who believe that investing in equipment for healthcare facilities is the answer are wrong. The use of technology and equipment depends much more on human resources. Motivation, training, maintenance, and follow-up will make the difference, and we believe this can be done if made part of or along with postsecondary education. In our case, a 20-year alliance with the Salesian Ladies Association has made this success possible. Alliances are the key to success.
Conclusions
Telemedicine is a very attractive term; it is trendy and relates to health, which is everyone's concern. People with a sense of health awareness and responsibility easily fall in love with telemedicine.
Proposals have been made to “quickly and massively spread its use by establishing hundreds of telemedicine centers at once.” This is the easiest way for a telemedicine project to fail. Why?
Limitation does not lie in technology, medical informatics, or telecommunication equipment, which despite being the backbone of the system are commercially available. The limitation lies in human resources and particularly in healthcare professionals whose recruitment has been the toughest endeavor.
This is followed by the lack of basic training on computers, Internet tools, the Web, and scientific digital imaging, which are required to get the most out of telemedicine.
Motivation, ongoing training and education, regular equipment maintenance, and management skill development will make a difference in healthcare delivery. Otherwise, we may waste years or even decades to reach a solution that is available to us today.
Footnotes
Acknowledgments
The Maniapure experience would not have been possible without the contributions of many public and private entities, local and international nongovernmental organizations, volunteers, employees, and socially responsible managers that have enabled the acquisition of equipment and training of local staff in the use of telemedicine technology.
Disclosure Statement
No competing financial interests exist.