
Abstract
Introduction
Telemedicine in the intensive care unit (ICU) (tele-ICU) dates back 2–3 decades, 1,2 with more rapid growth in the last decade following commercial development. 3 Tele-ICU includes complex systems like Philips/VISICU (Andover, MA), 3 –5 Cerner (Kansas City, MO), 6 and IMDsoft (Needham, MA) 7 and systems from Polycom (Pleasanton, CA), Tandberg (Oslo, Norway), and GlobalMedia (Scottsdale, AZ). Alternatively, “remote presence,” using medical robotics (InTouch Health, Santa Barbara, CA), 8,9 provides unique capabilities that add value in the chaotic environment of the ICU. From 2000 to 2010, a single design (Philips/VISICU) largely drove growth in the tele-ICU arena. As a consequence, the majority of the tele-ICU literature has evolved from the Philips/VISICU technology. However, recently, there has been significant growth with other vendors and technologies. As of 2011, robotic technology known as “remote presence” has been installed in more than 450 hospitals (information obtained from InTouch Health). The purpose of this article is to provide the first large-scale review of robotic “remote presence” technologies in the ICU.
The site from which ICU telemedicine services are delivered has been designated the tele-ICU. 10 –13 Growth of the tele-ICU has been driven by manpower maldistribution, 14 –17 shortage of intensivists, 18 –22 quality-of-care issues, 23 –26 success of the tele-ICU–structured care model, 27 –32 and measurable positive outcomes. 3,4,33 –35 More recently, a large study from the University of Massachusetts 36 indicated substantial improvement in mortality of patients managed with tele-ICU technology, largely the result of adherence to established standards of care. Following national political events in 2009 regarding healthcare reform, telemedicine has taken greater prominence as part of this evolution. 37 Furthermore, with a growing shortage of physicians expected to top 125,000 by 2020–2025, 38 maximizing efficiency of physicians is mandatory to include greater use of telemedicine technologies. Finally, with recommendations for further study of the tele-ICU concept, 39 we believe it is imperative to examine other modalities for the delivery of remote care in the ICU.
Process
Technology
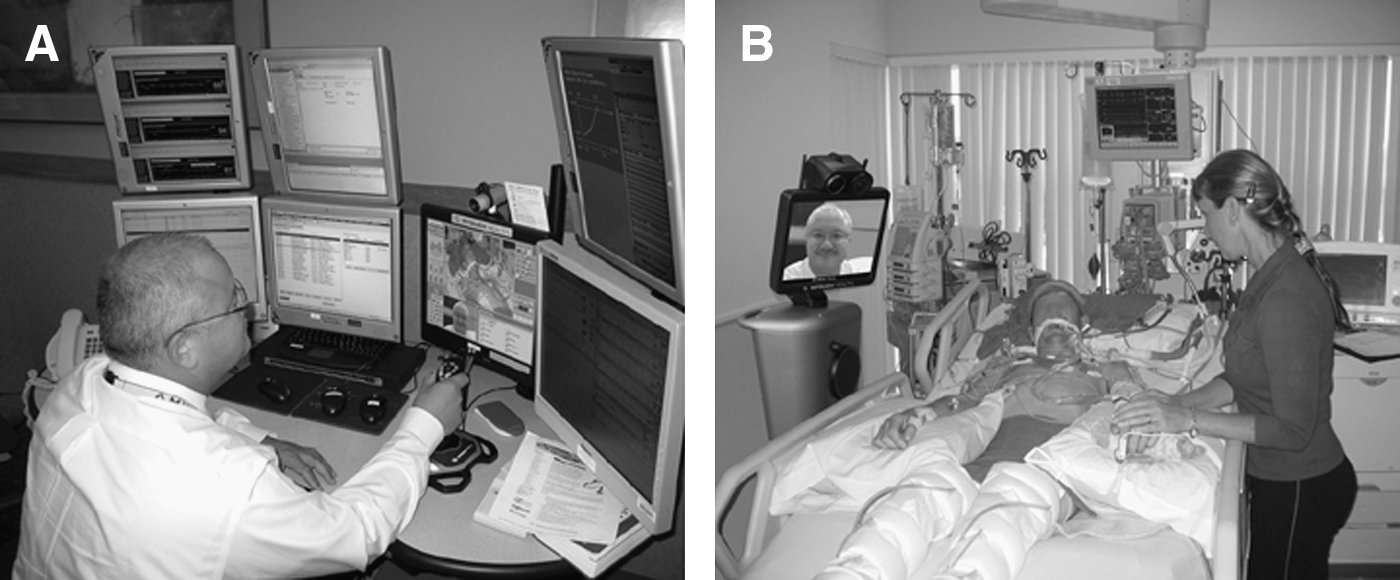
The technology used is a semi-autonomous, Internet-enabled, real-time, two-way audiovisual telecommunications platform that moves about in a wireless environment. The devices are casually referred to as “robots” providing “remote presence.” The robots are under the control of a remote clinician who can drive the device to the bedside, maneuver around the bed, perform visual physical examination, coach and observe a “surrogate” 40 examiner, and review graphical information on monitors, ventilators, balloon pumps, etc. (Fig. 1).
The “robots” are enhanced with electronic stethoscopes (Fig. 2 shows a telephonic stethoscope from TeleHealth Technologies [Viera, FL]) and may be further enhanced with lights to illuminate the retina, pharynx, ear canal, or tympanic membrane. In some cases, the devices have been enabled to transmit bedside ultrasonography in real time.

“Robot” with electronic stethoscope mounted on back. Use requires an on-site assistant such as a nurse to place the stethoscope over the heart, lungs, airways, or vascular structures.
The robots are controlled real-time by a remote physician at a “control station.” The control stations may be either portable or stationary. Portable control stations are laptop computers enhanced with necessary software, cameras, and headsets. Additionally, the laptops have “joy-sticks” for real-time control of the robot body and head and its direction of movement. All laptops are further equipped with WiFi cards, and some are further enhanced with cellular broadband capability.
Nonportable systems are traditional desktop computers with the above capabilities and generally with dual-view or triple-screen systems. Desktop systems generally have simultaneous access to hospital clinical information system and digitized radiography.
To provide care, networks are developed to accommodate local manpower supply and staffing patterns. Generally, one of two network patterns may be deployed: “centralized” or “decentralized” systems. 40,41 In general, the centralized programs supported multiple facilities, whereas the decentralized programs may have had the physicians rendering care to a single hospital.
Connectivity between the robot and hospital network is via an IEEE 802.11a, b, or g WiFi. Connectivity between physician control stations and hospital networks uses the bidirectional User Datagram Protocol (UDP). When institutional firewalls block UDP connections, communications servers broker the connection using Transmission Control Protocols. Data are encrypted with AES 256-bit symmetric encryption protocols. Video is captured at 30 frames/s and optimally requires 600 kilobits per second (Kbps) both up and down but will provide satisfactory performance at 400 Kbps and unsatisfactory performance at less than 250 Kbps. Optimization of available bandwidth and compression/decompression (CoDec) is provided by corporate proprietary methodology. Video CoDec is H.264 compliant and standards based. All control stations have echo-cancellation technology.
The remote presence robot is compliant with the Food and Drug Administration (FDA): Medical Device Data System Final Rule. Specifically, the device complies with FDA Class II requirements for devices that transmit, store, or display medical device information intended for immediate clinical action by healthcare providers. 42
Data Collection
The Fleet Monitoring System (FMS) is a proprietary (InTouch Health) corporate tool for tracking utilization and functional characteristics of remote presence robots in real-time, 24 h/day for every deployed device. The FMS provides status reports for robots and control stations by monitoring characteristics like battery strength, signal strength, software version, most recent use, most recent failure, and last report to the FMS. The FMS also monitors utilization and supports a database search to tabulate frequency of use by care provider, date and time, duration, etc. Finally, the FMS alerts the remote technical support team to take corrective action when a device experiences a failure such as a loss of connectivity or has reached a low battery level.
Remote presence robotic utilization and deployment were reviewed for a 12-month interval, from June 1, 2009 to May 31, 2010, via the FMS. Only robots known to be exclusively deployed in ICUs were studied. Users designating utilization primarily for stroke, emergency medicine, acute long-term care, translation services, or undefined services were excluded from review. Data were analyzed by facility, robot, month, and time of day. The study group was restricted to users accounting for 90% of the activations (the bottom 10% were not studied based on the assumption that they were in the training phase of technology acquisition). Data are presented by time of utilization. All data were de-identified as to facility or site.
Physician Survey
A Web-based survey was performed using “Survey Monkey” (Survey Monkey, Palo Alto, CA). The survey had 30 listed questions, with some of the questions having as many as seven embedded questions. The survey was validated internally. The questions were divided into six general categories: (1) Demographics of Tele-ICU Remote Presence Users; (2) General Utilization of Remote Presence; (3) Description of ICUs with Deployed Robots; (4) Application and Impact of Remote Presence in the ICU; (5) Physician Perspective and Views; and (6) an Optional section for identification.
Users and directors of the designated ICUs with remote presence robots deployed were identified. The identified individuals were e-mailed three times at weekly intervals and finally 4 weeks later. When possible, phone calls were made directly to nonresponders. Data were analyzed with Survey Monkey proprietary software.
Results
FMS Data
Review of the FMS data (June 1, 2009–May 31, 2010) revealed that there were approximately 350 remote presence robots deployed in North America; of these, 56 robots were dedicated to ICUs in 25 North American facilities. Because of the rapid growth of the market, some robotic devices have been included in the survey but only recently installed and therefore have minimal or no patient-related utilization. When there was less than 12 months of utilization, despite relatively high utilization for a short period (training and mock activations), the programs were excluded from analysis (Program 10). Programs outside North America were eliminated. Therefore, only the facilities with higher-level utilization were analyzed, which limits the analysis to 13 programs.
One program represents six facilities (Program 1), and another represents five facilities (Program 3). Otherwise, programs have one or two robots deployed and represent one or two facilities. Data are presented per robot. For example, Program 1 had 2,612 activations over six robots. Therefore, the average from Program 1 calculates to 47 sessions/month/robot. In summary, the programs included are Programs 1–9, 11, 13, 15, and 16.
During this 12-month period, there were 10,872 robotic sessions. Once the bottom 10% plus new/developing programs were excluded, 13 programs performed 10,065 activations (92.5%). The general overview of robotic utilization is presented in Figure 3.
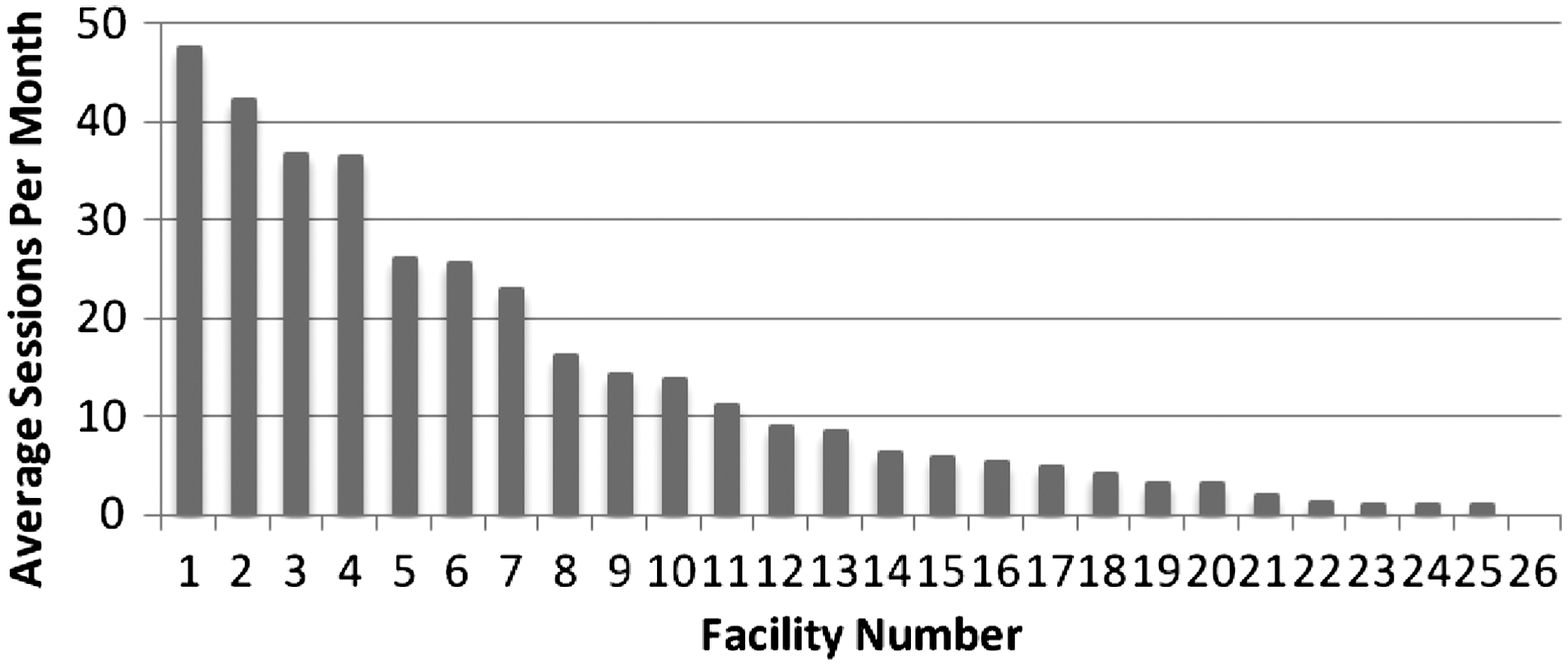
Intensive care unit–designated use of remote presence robotic technology presented as average number of sessions per month per facility. All specific facilities were de-identified.
Upon review of each facility, three patterns of use emerged. The first pattern is usage primarily during the early nighttime hours as seen in Figure 4. Two different facilities with almost identical patterns of usage yet substantially different programmatic structure were discovered: Program 2 is a large urban, tertiary academic medical center, whereas Facility 6 is a small urban, private, nonacademic hospital with intensivists in-house only during daytime hours only.

Total number of sessions, expressed as utilization by time of day, for
The second utilization pattern is high level during the daytime hours with minimal to no utilization during the evening and nighttime hours. Of the 13 institutions reviewed, 6 institutions fit the daytime-only utilization. Five of these six programs are large academic tertiary medical facilities. Figure 5 demonstrates one of the six programs with a typical daytime usage pattern.
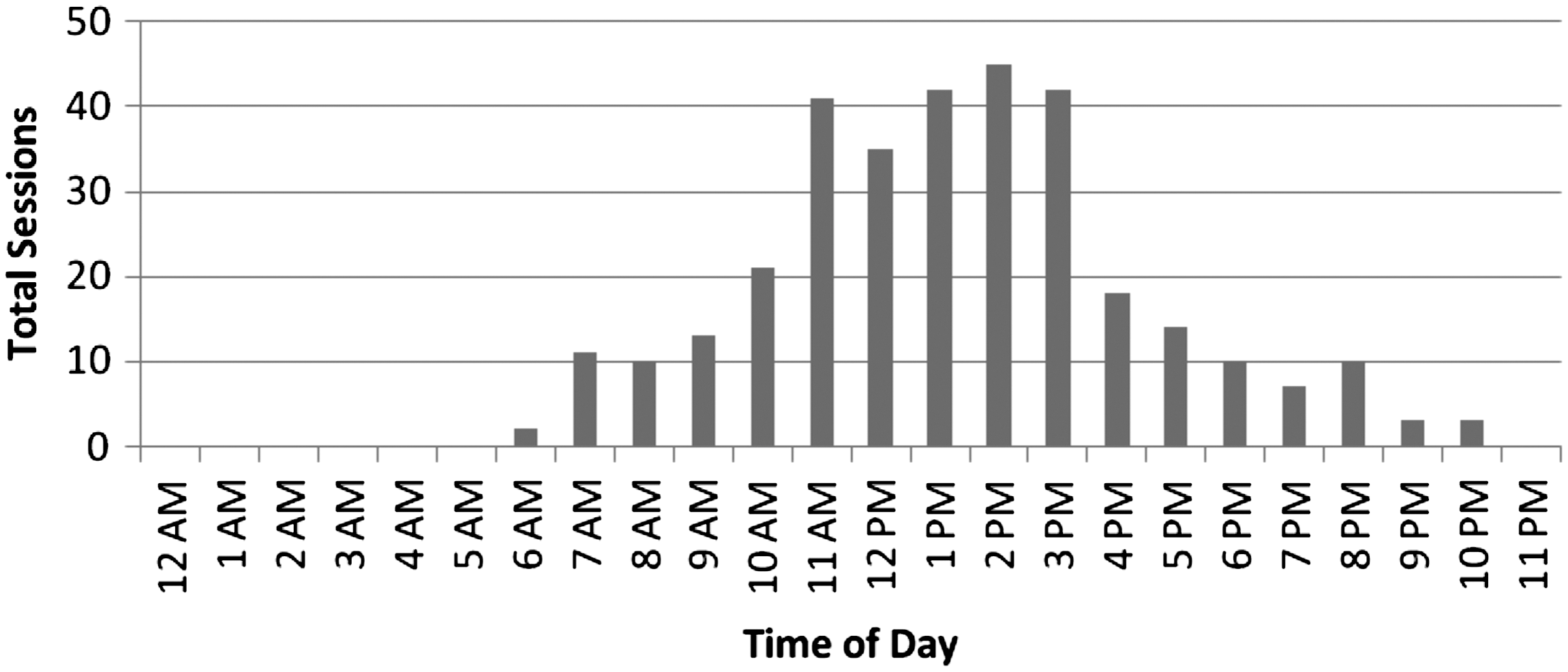
Total number of sessions, expressed as utilization by time of day, for Facility 4, a large, Northeast, tertiary academic hospital. The daytime-only utilization pattern of remote presence technology, peaking during typical maximal intensive care unit activity, suggests that the remote presence is used to support on-site staff during times of maximal load.
The third pattern of utilization is 24-h coverage. The 24-h pattern was discovered in five programs. Two of the programs have 24/7 contractual relationships with multiple facilities to cover multiple ICUs. These two contractual programs provided the two highest utilization rates of 2,612 and 2,199 tele-ICU sessions per year. Another program (Program 9) is the center of a statewide program providing acute services, and Program 15 is a multi-institutional program. Figure 6 demonstrates the near-continuous nature of remote presence utilization. Of note, even in the “continuous coverage” pattern, there is a very substantial slowdown during the hours from midnight to 5:00 a.m.

Total number of sessions, expressed as utilization by time of day, for
When all utilization data from all programs are combined, a pattern emerges of diurnal variation with maximum utilization midday (from approximately 9:00 to 16:00 h) and a second rise in the evening (approximately 20:00 through 23:00 h). In all patterns, the utilization is remarkably low during the hours from 00:00 to 05:00 h (Fig. 7).
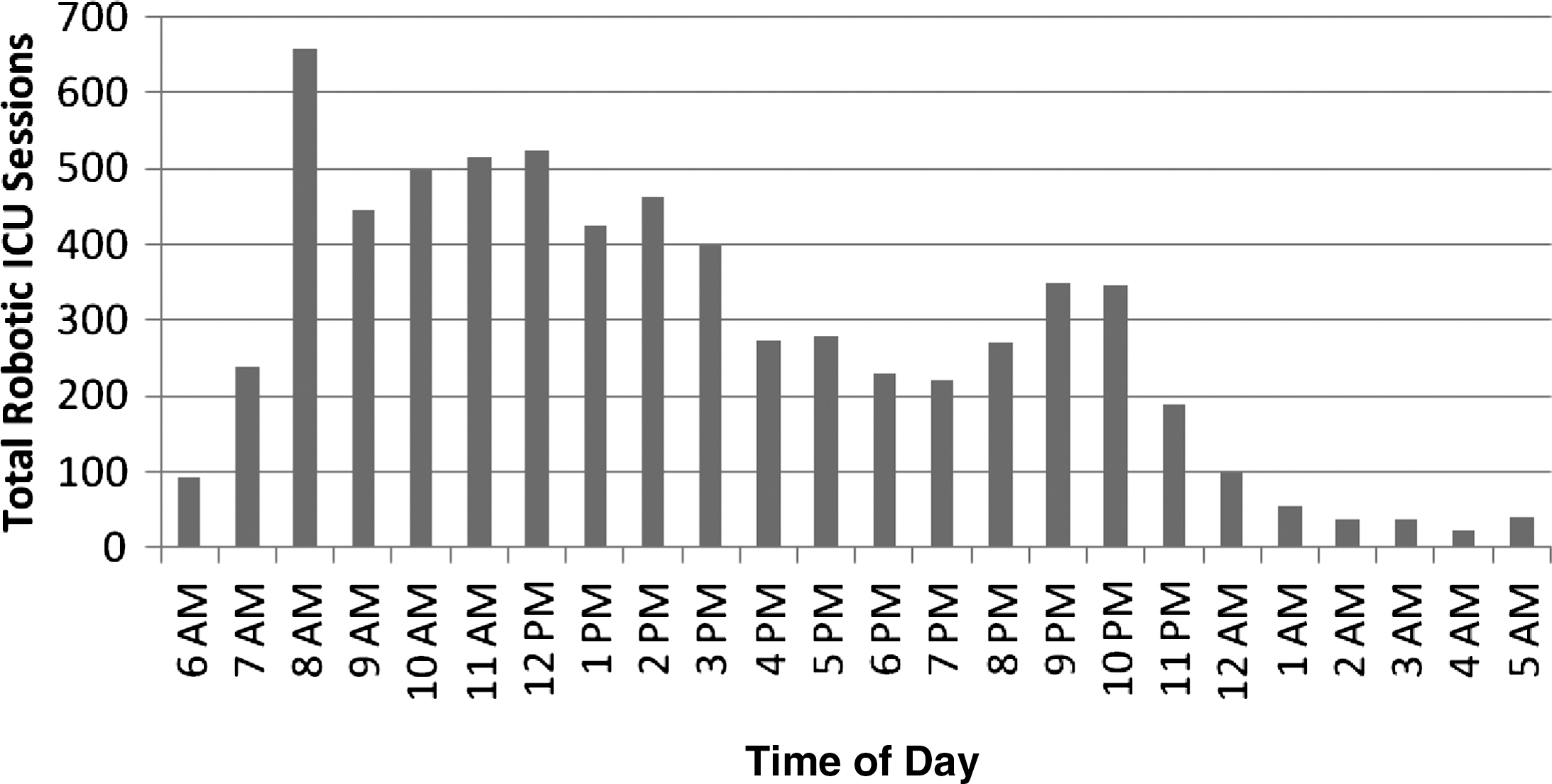
Overall remote presence robotic utilization in the intensive care unit by time of day combining data from “high users” during a 12-month period. Note the diurnal pattern of variation and minimal utilization during the hours from midnight to 5:00 a.m.
Closer analysis of the utilization patterns segregated by “day-shift,” “evening-shift,” and “night-shift” has been performed in Table 1.
Breakdown of Robotic Activations by Shift
Each program is defined based upon pattern as “evening-shift,” “day-shift,” or “24-h” coverage.
Overall, the vast majority of the utilization of remote presence occurs during the “day-shift.” On the other hand, the utilization during the “night-shift” is extremely small, at 4% of the total utilizations. Even within the two commercial programs (Programs 1 and 3), with contractual agreements for 24/7 coverage, the “night-shift” utilization is 5% and 6%, respectively.
Physician Survey
The physician survey yielded the following results. For the 25 institutions, 56 individuals were polled with 22 respondents.
Demographics
Of the survey respondents, approximately two-thirds of the care providers were trained in internal medicine, and one-fourth had surgical training. Over 80% had additional training in straight critical care medicine, and about one-sixth were pulmonary trained. Over 75% of the physicians were over 41 years of age. Approximately 60% of the care providers had more than 16 years in the general practice of medicine, while nearly 50% had been focused strictly in the field of critical care for 16 years or more. Regarding focus in critical care medicine, 59% dedicated 75–100% of their clinical practice to critical care medicine. In summary, the clinical staff is more likely internal medicine based, critical care trained, senior, and highly dedicated to critical care medicine.
Utilization
Over 70% of the respondents have been using remote presence robotic devices for more than 3 years, with half of those more than 5 years. Over 70% use only one device. Only one respondent indicated utilizing both “Robots and Carts.” Eighty percent of the physicians initiated remote presence robotic care from home, and additionally 17 of 22 respondents also initiated remote presence robotic care from a medical facility, suggesting that many have multiple control stations located at multiple sites.
In general, 87% of remote presence physicians are located in cities with a population >50,000, but surprisingly 80% of remote presence patient encounters are also in cities >50,000. Two-thirds of the clinicians provide service to only one ICU, but another combined 26% provide coverage to two or three ICUs. In summary, the remote presence programs are relatively matured and operate in a decentralized architecture from multiples sites. For the most part, remote presence physicians are located in larger cities, and remote care is provided in cities that are at least midsized.
ICU Descriptors
Of the primary sites where remote critical care services are delivered, 46.6% are either academic centers or university affiliates. Most of the remaining 53% are described as “community” facilities. As programs reach further out, there is a progressive shift to fewer or no academic facilities and predominately community facilities. Only three facilities were identified as critical access hospitals. Functionally, the vast majority of the ICUs were described as “Mixed Medical Surgical,” whereas only two sites were listed as neurosurgical and two as trauma. Of the 15 respondents, only 1 program was covering five ICUs simultaneously, with 33% covering two or more, 25% covering three or more, and only 20% covering four or more. Table 2 shows the spread of covered ICU beds and average number of beds.
Beds Covered by Robotic Remote Presence Among the 15 Respondents
ICU, intensive care unit.
The survey further revealed that within these ICUs, at the primary (first listed) ICU, 80% of the respondents provide both on-site and remote care. In summary, a significant amount of remote care is provided to academic facilities and/or university affiliates. Otherwise, essentially all care is rendered at community facilities and generally not in specialty care units. A majority of physicians provide remote and on-site care at the primary covered ICU, but the further removed the ICU is, the more likely that care will only be delivered remotely.
Application and Impact of Remote Presence in the ICU
Sixty percent of the respondents indicated that they use the robotic remote presence technology for routine “rounds” either very often or regularly. When rounds are performed, they are “scheduled” (73%), and over one-half of these scheduled rounds are in the evening. Otherwise, there was an even spread of rounding for “work,” “collaboration,” “teaching,” or “safety” rounds. Urgent response was performed either very often or regularly in 53%. Using the robotic technology for education was evenly spread across the spectrum, from 21% “very often” to 21% “never.” Family meeting were judged as “sometimes” among 53%. Two of the respondents indicated using the robotic technology for ICU “Triage” and “Consultation.”
Regarding perceptions of impact, 100% of respondents believe that remote patient care is either “very valuable” or “valuable” in improving patient care and patient/family satisfaction. Seventy-eight percent believe there was an associated reduction in ICU length of stay. Ninety-three percent (93%) believe remote presence improves compliance with best practices, and 87% feel that it improves nursing education. Impact upon physician quality of life was less certain, with 43% believing they had experienced an improvement, whereas 50% recognized no benefit. The data have been included in Table 3.
Respondents' Perception of Impact of Remote Presence Robots in the Intensive Care Unit
LOS, length of stay.
Physician Perspective and Views
The vast majority of physicians (87.5%) perform robotic remote presence without additional compensation. Sixty-six percent (66%) perceived the robotic technology as a “blessing,” 33% see the technology as a mixed “blessing and burden,” while none perceived the robotic technology as only a “burden.” Despite these perceptions, 100% of the respondents intend to continue to deliver services by robotic remote presence.
Discussion
To date, this represents the largest study of the applications of “robotics” in the ICU. This study of robotic utilization is designed to develop a descriptive picture of how robots are currently being deployed in ICUs. The FMS-derived utilization represents relatively hard data derived from an electronic database. However, the data only report the activation of the robotic device and do not offer insight into what is being done once it is activated. Therefore, it was imperative to add the user's description of the critical care environments and how the devices were being used. In addition, we have added the subjective element of how the user views the impact upon patient care, patient/family interactions, education, and impact upon the physician.
This is not an efficacy study. There are no objective data reflecting changes in mortality, morbidity, or length of stay. Despite the lack of objective data, there is a stunningly high and consistent impression from the care providers of improved patient care, shortened length of stay, greater adherence to best practices, and impact upon social issues such as patient and family satisfaction. This study did not query whether there are internal hospital data to support such impressions. Knowing that facilities in the United States are mandated by regulatory agencies 43,44 to collect, analyze, and retain quality data, it is presumed that internal data do exist that could support clinicians' impression of positive impact upon care.
Regarding the FMS utilization data, we have recognized three different utilization patterns based upon visual recognition. The pattern described as the “evening-shift” is most recognizable and objective, with very little daytime activity and a significant peak in the early evening hours. A “day-shift” pattern is recognized with little evening or nighttime activity and a dominant peak in utilization during daytime hours. The third pattern is characterized by 24-h activity. There may be some overlap between the “day-shift” pattern and the “24-h” coverage pattern. In certain cases, the pattern blurred between these two groups, and a judgment call was made by at least two observers/co-authors. The clinical significance of the various patterns is unclear except that the pattern paints a picture of how the robots are being used. In fact, it is unknown if the patterns reflect clinical needs or reflects programmatic design to satisfy some study or “pilot” evaluation.
What is remarkable is the high utilization of robotics by “day-shift” programs at academic and university affiliate centers, environments that would be assumed to be more than adequately staffed. In this review, approximately 50% of the covered facilities were academic centers. Perhaps this speaks to the ongoing shortage of specialists in critical care despite the otherwise well-staffed environments. In support of this concept, Lafit et al. 45 reported, in abstract form, an evaluation of robotics in an environment known to be heavily staffed and yet demonstrated a positive impact when remote clinicians provided an additional remote structured review of “best practices.”
When all the utilization data are combined, a distinct diurnal pattern evolves with two peaks of utilization: morning and evening. The ICU typically functions around an established diurnal flux of activity. Morning rounds with the intensivists, consultants, etc., lead to substantial activity as the days' plans are activated. However, the evening peak of activity may be driven more by nursing than physicians. ICUs are typically staffed with 12-h nursing shifts. With the transition to the evening, nursing staff typically review patients again and develop questions, leading to a secondary flux of activity.
The robotic utilization pattern imitates this waxing and waning of ICU activity, suggesting that the remote presence clinicians are closely mimicking on-site reality or needs. Furthermore, while nursing activity remains high during the late night, 46 physician activity seems to be minimal during the late night hours from midnight to 5:00 a.m. (Table 1). This may be pertinent from the perspective of administrators staffing a remote tele-ICU. Specifically, staffing could be heaviest during the day shift, intermediate during the evening shift, and “skeleton” for the night shift. Despite multiple articles in the literature describing work flow, 47 –49 to our knowledge, this is the most descriptive pattern of physician work flow or demands in the ICU.
In review of the physician survey data, staff working in a robotic remote presence–based “tele-ICU” are more likely internal medicine based, more senior by years of practice, and highly focused on critical care medicine. The greater adoption of the tele-ICU technology by senior staff has been recognized before 50 and may represent different clinical commitments in different generations, different views of the systems by senior staff, or lack of financial incentive for the younger staff. Most of the programs are also relatively mature, existing generally more than 3–5 years, and generally are single-ICU programs operating a single robot. All but one “tele-ICU” programs are decentralized, in that “rounds” or consultations may be provided from a multitude of different sites. This contrasts with the Philips/VISICU, Cerner, or iMDSoft programs with large, centralized tele-ICUs. The Web or Internet-enabled technology of the robotic remote presence devices supports an “open architecture” network 41 versus the more commonly used “closed architecture” of the Philips/Cerner/iMDSoft programs.
Regarding where services are delivered, remote care is more often delivered to moderately large cities (population >50,000) and generally to community facilities. Critical access hospitals, generally thought to be the most likely to deploy such remote technology, actually represented a minority of sites. We have previously observed and reported 51 a similar phenomenon in that a federally designated “Medically Underserved” facility may exist within a large urban environment, literally blocks from major medical centers. In fact, surprising numbers of facilities were “academic” or “university affiliated,” suggesting the locations would be urban. Finally, most were described as “Mixed Medical-Surgical” ICUs, while very few were specialty ICUs.
Physician work patterns indicated that most provide remote presence to a single ICU and that over 80% provide both on-site and remote care to those ICUs. Most of the rounds are scheduled and in the evening. This may suggest that the same physician who knows the patient by day could be performing some sort of routine or scheduled follow-up on patients in the evening. If this is indeed the case, the physician carries the patient “database” mentally with him or her. Therefore, large databases such as those found with the VISICU/Cerner/iMDSoft systems, which are necessary for staff covering unknown patients, would be less necessary for this cadre of physicians.
Physician perceptions of impact are highly positive despite lack of objective data. It is unknown whether there are internal hospital data supporting these perceptions, and the survey failed to interrogate for such supporting data. However, all these programs require financial investment and are unlikely to continue to exist without some sort of “value added.” Most facilities will search for a return on investment and may demand hard outcomes such as reduced length of stay but may also accept soft data such as patient/family/staff satisfaction. Therefore, it is assumed that value to the facility exists, but we failed to establish that value in an objective fashion. In final summation of physician perspectives, 33% reported the technology as a mixed “blessing and burden,” none reported getting extra compensation for robotic remote presence rounds, yet 100% intend to continue to deliver medical care via this technology.
A primary intent of this study was to determine the number of remote patient encounters or beds covered. We felt it important to generate an estimate to provide the reader with a general sense of the actual magnitude of remote patient encounters. To do so, the following assumptions have been made to create lower and upper estimates: 1. During the day shift, all patients are seen in each ICU. 2. During evening rounds, only one-half of the patients are seen. 3. During the night shift, only one patient is seen per activation. 4. The ICU has 80% occupancy.
The upper estimate is then generated using an upper average number of beds covered as 10 (rounded upper averages in Table 2). The lower average is taken as 5 (rounded lower average from Table 2) and is shown in Table 4.
Estimated Patient Encounters During 1 Year of Robotic Remote Presence Utilization
ICU, intensive care unit.
Of note, critical care services may be delivered in a variety of sites within the hospital to include the ICU, Emergency Department, and postanesthesia care unit or on the general medical or surgical wards, particularly during a “Rapid Response.” This review of utilization of the robotic technology for critical care services was designed only to assess critical care services performed within the ICU and therefore will underestimate the total volume of critical care services.
Conclusions
The robotic remote presence has substantial utilization in the ICU environment. The utilization includes a wide spectrum of types of ICUs to include large academic and referral centers and community centers. It is surprising that very few “critical access” hospitals are covered. The time-utilization pattern seems to mimic the natural ebb and flow of routine on-site activities of an ICU, suggesting that the robotic remote presence technology is supplementing typical day-to-day ICU activities.
The physicians involved in robotic remote presence tend to be more senior and have a high dedication to the field of critical care medicine. The physicians tend to be internal medicine based with additional critical care medicine training. There is a strong belief in impact on both clinical and social issues. Despite receiving no extra salary for services rendered by the robotic remote presence, most intend to continue using the robots.
The networking structure is greatly different from the larger centralized “hub and spoke,” closed architecture, networks. Clinicians using robotic remote presence technology tend to use a reverse hub-and-spoke configuration with a decentralized, open architecture network and may work from multiple different sites. Despite the absence of hard data, the number of actual patient encounters seems quite substantial.
Footnotes
Acknowledgments
The authors would like to thank Intouch Health for access to the data from the Fleet Monitoring System.
Disclosure Statement
E.M.R. had a 3-month employment as a summer intern with InTouch Health and has had no subsequent financial or working relationship. A.G., T.W., and M.F. are full-time administrative employees of InTouch Health. H.N.R. is a non-paid member of the Board of Clinical Advisors of InTouch Health and is a full-time staff member of the R. Adams Cowley Shock Trauma Center.