
Abstract
Introduction
Advances in technology are improving the ease and cost-effectiveness of remote communications. Several studies in the past have provided evidence for cellular communications as an option to improve patient care. 1 –3 Given the significant penetration of cell phones with text messaging (or short message service [SMS]) capabilities into the societies of the developed and developing world, 4,5 their potential for use or misuse is difficult to estimate.
The degree of acceptance and constraints on that acceptance by patients and healthcare providers must be understood to appropriately develop standards, policies, and protocols involving these forms of communication. Effective and appropriate ways to communicate with this tool have been addressed in some studies, 1,6 –8 including patients as young as 8 years of age. 9,10 The acceptability of communicating with parents was studied by Kharbanda et al., 11 but communicating directly with the pediatric patient was not examined. The acceptability of this form of communication in the pediatric setting remains poorly understood.
The development of future studies, policies, and standards involving the pediatric population needs greater clarity than currently exists. Although this is a broad topic, even coarse data will provide a starting point for more refined examinations of the depth and constraints of acceptability of text messaging with pediatric patients. The purpose of this study was to obtain preliminary data on the acceptability and feasibility of this form of electronic communication in the pediatric setting.
Subjects and Methods
After Institutional Review Board approval, two populations at our large urban pediatric clinics were asked to participate in this survey. All levels of healthcare provider in our clinics were recruited, including medical assistants, nurses, nurse practitioners, physician assistants, Ph.D.s, and physicians. The healthcare providers were approached electronically via either individual e-mails or official staff communication tools. These communications included a description of the survey and a link to complete the survey. No identifying data about those completing the electronic survey were collected. In total, 246 healthcare providers completed the survey.
Parents of children coming for clinic appointments were also recruited. The cancer care and radiology clinics were not included in this survey because of their separate locations, but all other clinics offered at our facility were. The parental survey was performed for 1 month, to ensure coverage of clinics that did not operate every day. Forms were available in English and Spanish, each including a description of the survey, its intent, and the elective nature of participation. Initially, parents were asked to complete the survey as they checked in for their appointments, but this produced a very low response rate. Subsequently, with Institutional Review Board approval, the surveys were included in the packet of papers given to families at check-in. This dramatically increased the survey completion rate. Again, no identifying information was collected on these forms, and completed forms were returned to several collection boxes throughout the clinics. Parental forms were completed and returned by 517 guardians.
Healthcare providers were asked questions regarding the level of care they provided and length of time they have been providing pediatric care. Subsequent questions asked their level of comfort with SMS-based messaging (texting) as well as instant messaging (IM), in case they were not users of SMS. Appropriate ages and uses for SMS were questioned as well. These uses were grouped as appointment reminders (Appointment), medication reminders (Medications), home testing reminders (Testing), home testing result transmission (Results), patient activity (Activity), and updates such as pain scores (Updates).
Parents were asked the age of their child being seen, whether they felt their child (regardless of age) was capable of using text messaging, and if their child had any neurological or physical limitations that would prohibit their use of SMS technology. Questions about approval of their child communicating with healthcare providers were also given. Categories of topics for communicating with healthcare providers included reporting who the patients were with (Who with), what their recent/current activities were (Activities), the results of home health tests (Tests), and their health status, such as pain scores (Status). Next they were asked at what age it would be reasonable for their child to have a device capable of using text messaging, and whether they currently possessed such a device. Parents were finally asked if they had devices capable of using text messaging and what their level of comfort was in answering questions about their child's health status on behalf of their children (as proxy).
Data from parental surveys were collected via a paper survey, with data being entered into an electronic database manually. The provider survey was performed electronically using Catalyst Tools (Web-based communication/collaboration tools) hosted by the University of Washington. A free-text field was available for description of "other" uses for which text messaging may be appropriate, but several respondents used this field to add other comments. All approval ratings are scored from 0=not at all to 4=completely.
The single Ph.D. respondent was grouped with the M.D./D.O. respondents for analysis. Medical assistants (M.A.s) and registered nurses (R.N.s) were analyzed as a single group, as were A.R.N.P.s (Advanced Registered Nurse Practitioners) and P.A.s (Physician Assistants). Similarly, levels of experience providing care to children were grouped into fewer than 5 years, between 5 and 10 years, and over 10 years.
Statistical analysis of this survey was based on frequency of responses using SPSS software (version 19.0.0; IBM, Armonk, NY). In responses where the data were incomplete, the samples were analyzed without the missing data. A value of p<0.05 was considered statistically significant. An independent-samples t test was used for comparisons within healthcare provider and parental groups. One-way analysis of variance for comparisons between groups and Spearman's ρ was used for correlations within groups.
Results
Demographics of parental respondents and the child patients are presented in Table 1. Among all guardians completing the survey, 13.6% reported developmental delays or physical limits that would prohibit their child's use of text messaging as a communication tool. This included 7.6% with both physical and developmental limits and 6% reporting either one of those issues. A majority (94%) of respondents reported having a phone capable of text messaging, while reporting 42% of the child patients did. The distribution of children with a phone by age is illustrated in Figure 1.
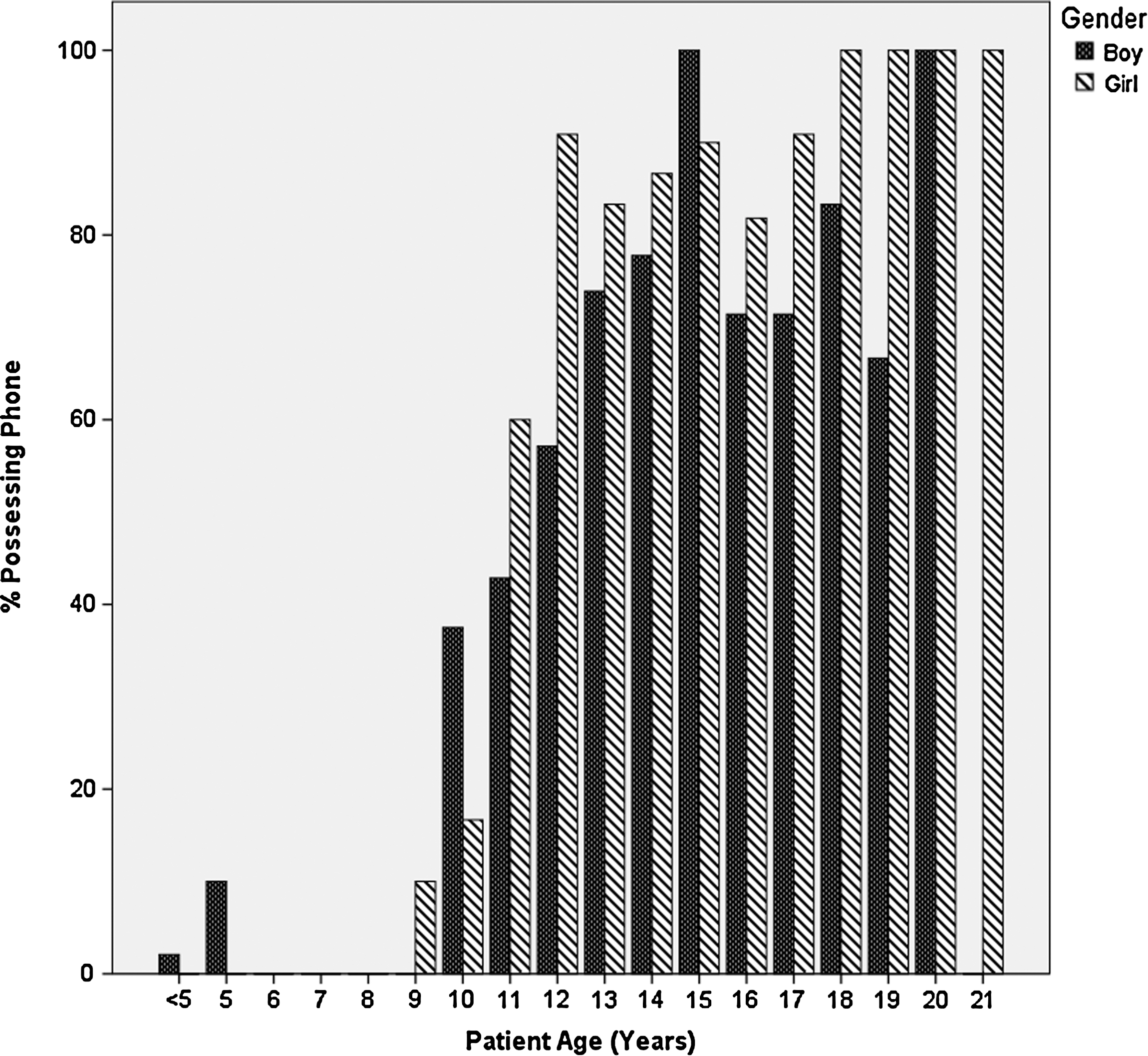
Children possessing short message service–capable phones.
Guardian Survey Demographics
When the answers are seen by guardians, approvals (Activity, 2.86; Who with, 2.51; Health Tests, 2.87; Status, 2.97) were higher (p<0.05 for all questions) than when the answers children provided could not be seen (Activity, 1.89; Who with, 1.67; Health Tests, 1.98; Status, 1.98). Approval for parental proxy reporting (Activity, 3.02; Who with, 2.77; Health Tests, 3.00; Status, 3.00) was higher than children reporting themselves, whether or not the parent/guardian would see answers the children provided. The difference in acting as a proxy reported between those with prohibitive disabilities and those without was not significant except in the case of reporting health tests, which was lower in the group with disability (2.58 versus 3.07, p=0.03). The approval for possessing a cell phone for text messaging of personal and health use is illustrated in Figure 2. There were no statistically significant difference between boys and girls for age to possess phones or approval for reporting (whether self- or proxy reporting).
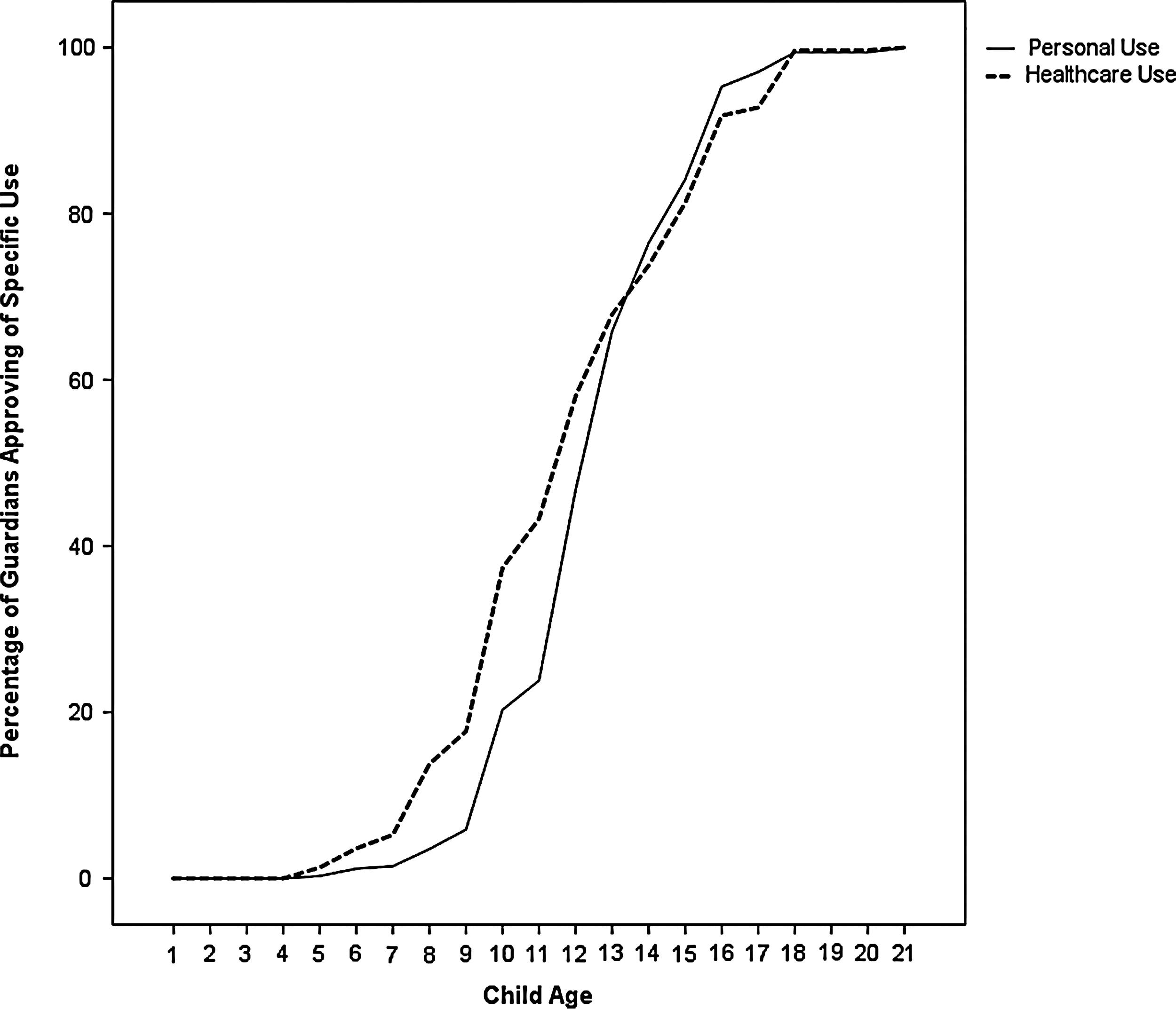
Approval by guardians of children possessing a cell phone for text messaging for personal or healthcare use.
Those respondents using the Spanish version of the form had some differences in their responses. They were less approving of providing status updates when they could not see the child's answer, but more willing to report who the children were with when acting as their proxy (p=0.036, 2.01 versus 1.00; and p<0.01, 2.74 versus 3.56, respectively). There were too few respondents on the Spanish form to separately analyze those with and without disabilities.
When the guardian can see the answers provided by their child, the age of the patient correlated with the acceptance of all uses of text messaging, with the exception of status updates (correlation coefficients: Activity, 0.207, p<0.001; Who with, 0.195, p<0.001; Tests, 0.160, p=0.002). When the guardian was not able to see the answer provided, the age of the patient correlated with all uses of text messaging (Activity, 0.243, p<0.001; Who with, 0.254, p<0.001; Tests, 0.246, p<0.001; Status, 0.227, p<0.001).
Whether the child possessed a cell phone correlated negatively with approval for all uses of text messaging, whether the guardian could see the answers (Activity, −0.238, p<0.001; Who with, −0.188, p=0.001; Tests, −0.214, p<0.001; Status, −0.160, p=0.003) or not (Activity, −0.252, p<0.001; Who with, −0.192, p<0.001; Tests, −0.270, p<0.001; Status, −0.250, p<0.001). The guardian's possession of a cell phone only correlated with reduced acceptance of children reporting health test results (−0.133, p=0.013) and status updates (−0.143, p=0.008) when the guardian cannot see the responses.
Fifteen of the 517 parental surveys returned contained handwritten comments expanding upon responses. The most common (n=4) reported the age for healthcare use to be "when necessary" or when able to read/write. The next most common type noted approval for healthcare uses should be based on the purpose and times of communication or the questions being asked (n=2). There were comments either noting a preference for e-mail messaging (n=2) or just stating use of SMS was not at all appropriate (n=3). Two comments concerned security or privacy, and one was about the expense of text messaging.
In computer-based IM, significant comfort differences were found between those with <5 years or 5–10 years of experience and those with 10 or more years (means, 3.16, 2.73, and 2.29; p<0.001 and 0.05, respectively). Additionally, those with fewer than 5 years of experience were more comfortable with SMS compared with those with more than 10 years (mean, 3.32 versus 2.74; p<0.01). The level of comfort using IM was significantly higher in the M.A./R.N. group compared with the A.R.N.P./P.A. and M.D./D.O./Ph.D. groups (p=0.033, 2.97 versus 2.44; and p=0.01, 2.97 versus 2.29, respectively), as was opinion of the age of being capable of using IM (p=0.037, 9.85 versus 9.09; and p<0.01, 9.85 versus 8.79). However, these differences in comfort level did not correlate with the age at which a child was felt to be capable of using text messaging or the age it was felt to be appropriate. Time providing care for children was mildly but significantly negatively correlated with the age personal use was appropriate (−0.182, p<0.01). The mean age providers felt children were capable of using SMS messaging was 9.2 years (±2.0 years). They felt personal use of SMS was appropriate at 12.45 years (±2.7 years), while healthcare-related use was appropriate at 14.6 years (±2.8 years).
When asked what were appropriate healthcare uses of SMS, the M.A./R.N. group showed significantly less belief than the M.D./D.O./Ph.D. group in the utility of text messaging to serve as a reminder for medication/treatments (p=0.025, 68% versus 83%) or for obtaining updates (p=0.041, 53% versus 68%). Other differences were nonsignificant. There was no correlation between years providing pediatric care and the appropriate uses for text messaging. Overall approval of SMS as an appointment reminder was 86%, and as a medication reminder it was 77%. Testing, Results, Activity, and Updates were less popular options (76%, 55%, 51%, and 63%, respectively), but only 7% of respondents thought none of these was an acceptable use of SMS technology.
Healthcare providers mentioned other uses not specified as an option several times. These suggestions included reporting nutritional information or blood pressure readings, reporting concerns or requesting calls from a provider, or providing follow-up information to/from the patient.
Concerns expressed in the free-text field included the level of sensitivity of the data transmitted as well as the security measures in place for any such system. Comments directed at a practical level included suggesting a centralized service for the clinics, rather than individual practitioners. There was also concern expressed that text message reminders could reduce the level of personal responsibility of the patients in taking care of themselves. On the other hand, it was mentioned that result-specific information should be followed up with a phone call.
Discussion
The results of the healthcare provider survey show staff in the pediatric clinics are generally comfortable with the use of IM and SMS technology. The M.A./R.N. group was more comfortable with IM use, while those providing care for a shorter time were most comfortable with both IM and SMS use. Comfort level did not correlate with the ages at which practitioners felt children were capable of using SMS nor when it would be appropriate for their use. There was significant agreement in the ages that healthcare providers felt patients would be capable of using SMS, as well as when they would be old enough to use it for personal and healthcare-related uses (about 9, about 11, and about 13 years old, respectively). The M.A./R.N. group felt patients would be capable of using SMS significantly earlier than their colleagues, however. Length of time providing pediatric care was negatively correlated with age for personal use, perhaps a reflection of less experienced staff (i.e., younger) being more comfortable with their personal use of SMS. All groups of practitioners rated appointment reminders highest as a potential use for SMS, while medication reminders and testing results were always in the top three. M.A./R.N. groups were significantly less optimistic than the M.D./D.O. group about the use of SMS for reminders or updates, perhaps reflecting the different interaction experience with patients.
There is a high penetration of cell phones in this population: 94% in parents and about 75% by the age of 13 years in pediatric patients. Approval for possessing cell phones rises dramatically at 10 or 11 years of age, while approval for personal use seems to lag behind healthcare use. Parental responses indicate acting as a proxy is preferred in communicating, followed by being able to know the answers their children provide, with not knowing the answers least preferred. Parents with phones were more cautious in their approval, but only in the areas of tests and updates (with unseen answers) did this reach significance. Patients who did not have phones and older patients both correlated with higher approval of the use of SMS. Gender of the patient did not seem to play a role in the guardian's approval of SMS use/cell phone possession. Guardians using the Spanish forms were similar in their answers, suggesting broad applicability.
Approval of the use of SMS technology by the healthcare providers and guardians was positive overall, with some variation based on provider type and experience. These could be seen as correlating with the provider's age, as younger staff are unlikely to have had time to complete higher degrees or accumulate years of experience. However, these data were not collected so conclusions based on this hypothesis cannot be drawn. Use of SMS for healthcare by pediatric patients seems to have approval at the age of 15 years, with 13 years being appropriate for personal use. Whether the results of this survey would be different in a research setting as opposed to routine healthcare use is uncertain. Other factors that may significantly alter guardian approval might be patients with chronic diseases or on sensitive topics such as sexual health. Parental approval for cell phone possession rises as the healthcare providers significantly increase their belief that personal use of SMS would be appropriate. However, guardians seem to approve of healthcare-related use of SMS sooner than personal use, perhaps presenting opportunities for use that the healthcare provider might otherwise miss. The high acceptance of SMS for appointment reminders, medication reminders, and obtaining testing results implies areas ripe for use in clinical practice, although clinical research on a variety of topics can also benefit from the use of SMS.
Earlier work in text messaging with adolescents has dealt not only with the technological aspects of using SMS but also with the social and cultural aspects. Alfvén 9 noted that in adolescents phones were not considered unusual, and actions such as notes for teachers can improve utility. It was also noted that language used in SMS must take into account the memory limits, attention span, and vocabulary of the participant. 9 Woolford et al. 12 evaluated the communication preferences of participants of a multidisciplinary weight management program. Furber et al. 6 noted no abuse of the system, although concern was raised about reporting personal information.
The high level of disability in this patient population may be a barrier to some uses of SMS, although parent proxy seems to remain an area of potential use of SMS. The potential for including these populations can be assisted with SMS technology as discussed for the deaf/hard of hearing by Power and the physically impaired using electromyography technology. 13,14 Parental readiness for the use of SMS was also examined by Kharbanda et al., 11 although in that case the parents were the targeted recipients of the messaging rather than the child patients. While parents felt SMS could be more effective in that study, Hart et al. 15 found that physicians were hesitant to implement an SMS reminder system and suggested it might be due to the lack of empirical evidence for such systems.
The use of SMS as a component of a clinical appointment reminder system has been examined in several clinic settings and nations, with positive results. It has also been used to evaluate patient satisfaction with care and as a component in a system for booking appointments, obtaining prescription renewals, and receiving core clinical summaries. 4,16 Of note is that it was found to be as effective but less expensive than phone calls. 2,17,18 Practitioner concerns about reminder systems and phone follow-up were previously touched upon by Saw et al. 19 in the context of transmitting critical laboratory results, while secure messaging was discussed in more detail by Prestigiacomo. 20
Variation in acceptance of SMS technology across the United States and the globe will need to be addressed further, as it is clearly being used. In Malawi it was used to reduce significant travel for healthcare 21 and assisted with highly active antiretroviral treatment management in Kenya. 5 It has been used to improve functioning in patients with schizophrenia as well as traumatic brain injury and in reducing indications of elevated blood sugar in diabetics. 10,12,22
This report provides the results of a parental and a caregiver survey in a large, urban pediatric clinic. Clear weaknesses of such a study include poor control of participants enrolling, such that these data may not be able to be extrapolated to the population across the United States or internationally. In this case, the age of the patients was skewed. Whether this biased the opinions of the parents is unclear. Efforts to enroll as broad a population as possible required a brief survey, with the consequence of an incomplete picture of parental and healthcare provider opinions.
The parental and healthcare provider surveys both demonstrated broad approval for the use of SMS in pediatric healthcare. Approval varies on a number of factors but opens the possibility of broad clinical and research use in pediatrics. Clearly issues remain to be addressed, such as how to integrate such technology into a practice, address security and privacy concerns, and decide what messaging is appropriate for which patients. Duplicating some of the research into what content is ideal while including parents may help create communications with broad approval for parents and an acceptable tone for the patients. Exploration into the technologies to enable those with limitations to utilize such messaging systems, such as electromyography, would expand the broad utilization and bring those otherwise potentially isolated patients further into the mainstream of healthcare.
Footnotes
Disclosure Statement
No competing financial interests exist.