
Abstract
Introduction
Asthma is one of the most common chronic diseases that affects a large proportion of the population worldwide and can be fatal. 1 The level of asthma control remains inadequate for most patients despite the emergence of new effective controller therapies. 2 Evidence has shown that psychosocial factors play a critical role in the outcomes of patients with asthma. 3 –7 Perceived control of asthma (PCA), 8,9 which is defined as individuals' perceptions of their ability to deal with asthma and its exacerbations, is one of the most important psychosocial factors positively correlated with asthma outcome. PCA is related to the general theories of self-efficacy, locus of control, and learned helplessness. Greater PCA has been shown to be associated with better asthma-related health status and less prospective risk of hospitalization and emergency department (ED) visits. 8 –10 However, the levels of many patients' PCA were lower, 11,12 and preventive care or asthma self-management practices could not completely improve it. 13 Therefore, it is important to find a more effective way to increase patients' PCA.
Guided self-management strategies, including asthma education sessions, self-monitored peak expiratory flow (PEF) monitoring, keeping an asthma diary, and making an action plan, have been proved effective to improve asthma outcomes in previous studies. 13,14 However, significant external barriers such as time and distance barriers exist and directly influence the participation rates and the effect of traditional asthma education. 15 In busy outpatient clinics, doctors usually do not have enough time to teach asthma patients to manage asthma with comprehensive traditional formal asthma self-management programs, which is recommended in the Global Initiative for Asthma (GINA), 16 so it is necessary to simplify asthma education programs.
Previous studies showed that short message service (SMS) was a potentially powerful tool to overcome external barriers and had been delivered to patients with chronic diseases in many different areas. 17 –19 SMS education can increase adherence to asthma treatment, asthma control rate, and quality of life and decrease episodes of exacerbation and unscheduled visits as reported 20,21 ; however, whether SMS education could help to overcome intrinsic barriers and improve patients' PCA remains uncertain.
Subjects and Methods
Patients
Patients meeting the inclusion criteria were recruited as they presented to the Department of Respiratory Medicine of Southern Medical University, Nanfang Hospital (Guangzhou, China), for asthma care. Inclusion criteria were as followed: older than 18 years of age, physician-diagnosed asthma according to GINA at least 3 months before recruitment, bronchodilator reversibility test or bronchodilator provocation test positive in the past year, owning a mobile phone, and ability to read and understand the questionnaires. Exclusion criteria were respiratory infection within the previous 4 weeks, pregnancy, heart disease, stomach surgery, other lung diseases, or current or past smoking history of >10 pack-years.
Study Design
This trial was a prospective, randomized, controlled study. One hundred fifty eligible asthma outpatients from March 2009 to April 2010 were enrolled and randomly assigned to three groups: control, traditional, and SMS groups (Fig. 1). They received different education programs for 12 weeks. Data on PCA, the asthma-specific quality of life, lung function, blood and sputum markers, and follow-up adherence rate, medicine compliance rate, and ED visits were collected at the initial visit and the end of the study. Oral informed consent was obtained from all participants, and the protocol was approved by the institutional review board of Southern Medical University. During our research, personal health information was strictly confidential, and the doctor was always available for consultation to safeguard patients' security.

Trial profile.
The control group
Participants of the control group received verbal asthma education information from their outpatient clinic physicians at the initial visit, including standardized components regarding asthma facts and verbal and graphic interpretation of lung function results, medication actions, and inhaler technique.
The traditional group
In addition to receiving control education, patients in the traditional group received a free PEF meter and were trained on its proper use. Patients were told what to do if their reading fell in the yellow or red zone and encouraged to write asthma diaries about asthma symptoms, PEF data, and medication usage. They were taught how to adjust an action plan based on their diary entries.
The SMS group
In addition to receiving control education, patients in the SMS group received short text messages reminder about how to manage asthma at 10:00 a.m. and 8:00 p.m. every day from clinic investigators. The content of the short text messages included introduction to asthma, classes of asthma medications, proper device use, common types of triggers, strategies for avoiding triggers, how to make an action plan, and how to handle asthma acute attacks. If they had any questions about asthma, patients could send short text messages by their mobile phone to clinic investigators and receive answers.
Outcomes
PCA was measured through the six-item PCA Questionnaire (PCAQ-6), 11 which has been previously validated. It contains six items, and scores range from 1 to 5; sum scores range from 5 to 30, with higher scores reflecting greater perceived control of asthma.
The asthma-specific quality of life was assessed by using the Standard Asthma-Specific Quality of Life Questionnaire [AQLQ(S)], 22 a 32-item questionnaire that measures the symptoms, physical, emotional, and social impact of asthma. Sum scores range from 32 to 224, with higher scores representing greater asthma-specific quality of life.
Asthma severity was measured by the forced expiratory volume in 1 s (FEV1%). Asthma control level was divided into mild (FEV1% ≥80%), moderate (60% ≤FEV1% <80%), and severe (FEV1% <60%). Pulmonary function was assessed before sputum induction using the Jaeger (Wuerzburg, Germany) Masterscope® spirometry system according to American Thoracic Society guidelines. 23
Blood and induced sputum samples were collected at the initial visit and the end of the study to assess the degree of airway inflammation. For sputum induction and processing, we used the guidelines suggested by the Task Force on Induced Sputum of the European Respiratory Society. 24
Follow-up adherence rate, medicine compliance rate, and ED visits data were collected at the end of the study.
Statistical Analysis
The results were analyzed by SPSS version 13.0 (SPSS, Inc., Chicago, IL). The analyses were conducted on only those subjects who completed the follow-up visit (n=71). The results were expressed as mean±SD values for continuous variables and median (interquartile range) for variables of skewed distributions. For categorical variables, the number of observations and percentages were given in each category. Paired-samples t tests were used to assess differences within each group for all outcomes comparing baseline with 12 weeks, while one-way analysis of variance and least significant difference methods were used to compare changes among groups after education. Skewed distribution data were analyzed by the nonparametric test. Categorical data were analyzed by chi-squared tests. Pearson's correlation test was used to examine the association between changes of PCA and asthma-specific quality of life. A value of p<0.05 was considered statistically significant. The covariates that influenced the dependent variable were controlled.
Results
One hundred fifty patients met the inclusion criteria. Ages ranged from 18 to 65 years in all groups. There were 14 patients who came back for the follow-up visit in the control group, while 27 patients in the traditional group and 30 patients in the SMS group returned (Fig. 1). The characteristics of all patients who finished the study are shown in Table 1, and there was no significant difference in gender, age, body mass index, educational level, health insurance, FEV1% predicted, asthma severity, and other factors among the groups except percentage of sputum neutrophils as shown in Table 1. We adjusted the analysis of sputum neutrophils percentage variable, and there was no differences between the adjusted and unadjusted analyses.
Demographics and Baseline Characteristics of Patients Who Finished the Study
Data are mean±SD values, median (interquartile) values, or number (percentage) as indicated.
AQLQ(S), Standard Asthma-Specific Quality of Life; BMI, body mass index; FEV1, forced expiratory volume in 1 s; PCAQ-6, six-item Perceived Control of Asthma Questionnaire.
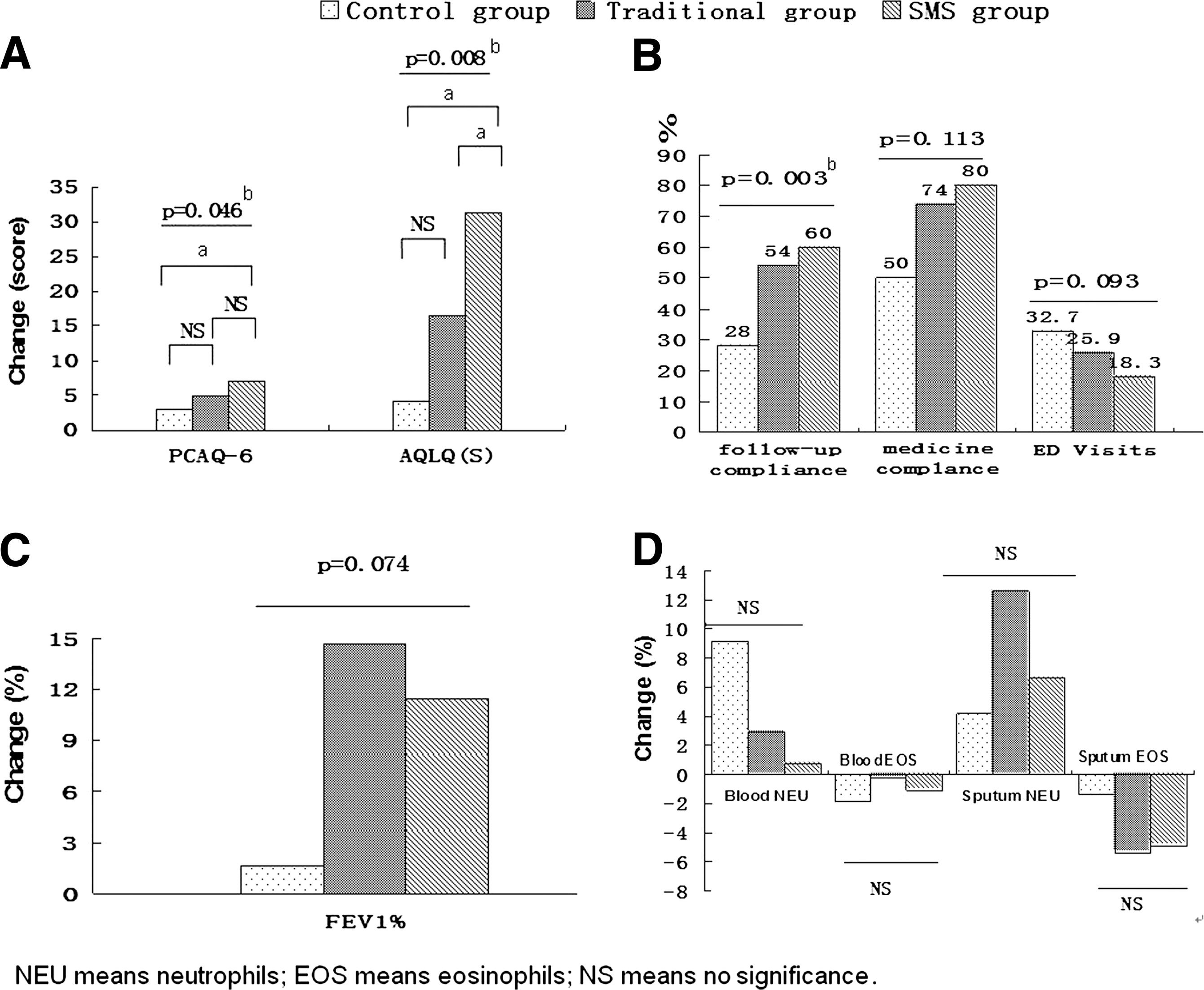
PCAQ-6 scores ranged from 10 to 26 (18.75±3.42) for all patients, and it was significantly lower than that in the study of Chang et al. 11 Patients' PCAQ-6 scores improved significantly in the traditional group and the SMS group (p<0.001), whereas the control group showed no improvement (p=0.054) at the end of the study (Fig. 2A). The mean change in PCAQ-6 score did differ significantly among groups (p=0.046) (Table 2). The mean change of patients' PCAQ-6 score in the SMS group was significantly higher than in the control group (p=0.018, least significant difference), although there was no significant difference between the SMS group and the traditional group (p=0.299).

Scores on the six-item Perceived Control of Asthma Questionnaire (PCAQ-6) in
Mean Changes in Outcomes from the Baseline to the End of the Study
Data are mean±SD values.
V1, visit 1 (baseline); V2, visit 2 (end of study).
Patients' AQLQ(S) scores improved significantly in the traditional group and SMS group after education compared with no change in the control group. The changes in AQLQ(S) score differed significantly in the three groups (p=0.008) (Table 2 and Fig. 3A), and the change in AQLQ(S) score of patients in the SMS group was highest. The change in PCAQ-6 score was related to the change in AQLQ(S) score (r=0.442, p<0.001) (Table 2).
Changes in the control, traditional, and SMS groups in
The follow-up adherence rates of 28%, 54%, and 60%, respectively, were significantly different in the three groups (p=0.003). More asthma patients who received the mobile SMS intervention came back for the follow-up visit than those receiving traditional education intervention (Fig. 3B). Table 3 shows the reasons for patients' withdrawal in the three groups. As shown in Supplementary Tables S1–S3 (Supplementary Material is available online at
The Reasons for Patients' Withdrawal from the Study
PEF, peak expiratory flow.
Medication compliance rates for the patients who completed the follow-up visits did not differ significantly among the three groups (p=0.113), but the rate was higher in the SMS group (80.0%) and the traditional group (74.1%) than in the control group (50.0%) (Fig. 3B).
The incidence of ED visits did not differ significantly in the three groups (p=0.093), and the patients in the SMS group had the lowest rate of unscheduled visits (Fig. 3B).
FEV1% predicted improved in all groups compared with the initial visit data, but no significant differences were observed in the change rates among the three groups (Table 2 and Fig. 3C).
Blood and sputum eosinophil counts (as a percentage) significantly decreased in the SMS group but not in the other two groups. Blood and sputum neutrophil counts were not changed significantly in the three groups. There were no significant differences among the three groups in the changes of eosinophil counts and neutrophil counts in blood and sputum (Fig. 3D).
Discussion
We first studied the use of mobile health technologies to improve asthmatics' PCA and compared the SMS program with the traditional educational program (traditional group) and the outpatient ordinary service (control group) in improving patient-centered outcomes, using a prospective observation design. The major findings of this study were as follows: (1) PCA can be enhanced by SMS and traditional asthma education, and the improvement of PCA correlated to the improvement of asthma-specific quality of life; and (2) SMS had more advantages in improving patients' follow-up attendance rates and asthma-specific quality of life than traditional education programs.
In this study, we showed that PCA values were lower in all groups compared with the report by Chang et al. 11 This finding proved again that it is necessary to pay more attention to PCA and find a way to improve its level. Also, our study demonstrated that both SMS and traditional education programs can improve PCA. The change in PCAQ-6 scores was higher in the SMS group compared with the control group, whereas there was no difference between the traditional group and the control group, indicating the advantage of SMS. Consistent with our study, there was also a report 9 that PCA could be improved with traditional education programs. By contrast, Calfee et al. 10 found that the asthma preventive care (including asthma PEF monitoring, asthma education, and self-management, which were similar to traditional education programs in our study) could not improve PCA. In their study, the subjects studied had much more serious asthma (intensive care unit admission rate of 22%). This is a likely reason for the difference in findings, as we have shown the recruitment samples in our study were outpatients with mild or moderate asthma. SMS was proved to be useful to increase adherence to asthma treatment and improved asthma control as reported previously, 20 and our study further supported its important role in asthma management such as improving PCA of asthmatics.
We also found changes in AQLQ(S) correlated significantly with PCAQ-6. This has been supported by many other studies 8 –10 in which patients' PCA was related to asthma-related health status; these studies showed that if PCA could be modified, better outcomes (particularly better psychological outcomes) might be achieved for individuals with asthma. This study also indicated that PCA, as a psychosocial factor, plays an important role in asthma outcomes.
In this study, we also found the patients in the SMS group had a better follow-up rate (about 60%) compared with the other groups (54% in the control group and 28% in the traditional group). The follow-up compliance and medication compliance rate were lower in all groups in our 12-week study, as described by Lemaigre et al. 25 Janson et al. 26 reported that adherence to self-management decreased over time for a 24-week intervention. In our study, external barriers such as time and distance were the leading causes of failure to follow-up.
Our results showed that the patients in the traditional group who completed the study had more serious asthma than those who withdrew by comparing baseline characteristics of patients. However, there was no significant difference in the other two groups. We speculated that the milder asthma patients in the traditional group may think their asthma conditions were under control and they did not need a doctor's help, 15 so they chose to withdraw. Also, it may indicate that the traditional education program is not attractive enough for milder asthama patients. Therefore, our study indicated that the SMS program is more useful and attractive to patients with asthma of any level of severity.
In this study, we also found both SMS and traditional programs can improve patients' FEV1%, and we did not find any advantage of SMS compared with the other groups. In this study, the low medication adherence should be taken into account. Evidence 27,28 had shown that adherence to medicine is very important to asthma control. Long-term use of action plans or SMS for self-management can reduce asthma exacerbations. 13,20 However, the incidence of ED visits did not differ significantly among the three groups in our study. So these still need more strict and long-term study to clarify.
In this study, we also found that blood and sputum eosinophil counts (as a percentage) significantly decreased in the SMS group but not in the other two groups, and we found the medication compliance rate was higher in the SMS group (80.0%). Previous studies showed that blood and sputum eosinophil count may reflect asthma activity 29 and can be used to assess the compliance with corticosteroid therapy in asthma. 30 So we speculated the decrease of eosinophil counts in the SMS group may be related to the high adherence to inhaled corticosteroid treatment.
This study has several limitations. First, although patients agreed to participate in our study, nearly half of the patients did not finish the study in the end. Second, we did not ask patients of the SMS group to reply to the daily SMS, except when they came across problems in the course of treatment of asthma.
In conclusion, our study showed an SMS education program can overcome the internal barrier and improve the level of PCA and had advantages in improving patients' follow-up rate and asthma-specific quality of life compared with a traditional education program.
Footnotes
Acknowledgments
This work was also supported in part by the pulmonary function technicians who work in the Lung Function Department, Nanfang Hospital, Southern Medical University, Guangzhou, China.
Disclosure Statement
No competing financial interests exist. Y.L., H.Z., Z.L., H.D., D.Z. and S.C. made substantial contributions to the conception and design, acquisition of data, or analysis and interpretation of data. All authors drafted the submitted article or revised it critically for important intellectual content and provided final approval of the version to be published.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.