
Abstract
Introduction
Chronic obstructive pulmonary disease (COPD) is estimated to affect 210 million people worldwide. 1 As disease severity increases, exacerbations become more frequent, with consequent poorer quality of life, more rapid decline in lung function, and decreased survival. 2 –5 Emergency department visits and hospitalizations, with their attendant costs, are more likely during acute exacerbations. 6 –8 Reported in-hospital mortality ranges from 2.5% to 25%, and, of those who survive, 25–55% will be re-admitted, and 25–50% will die within 12 months. 9 Focusing on both preventing exacerbations and reducing their severity in this at-risk patient group is, consequently, of vital importance.
A Cochrane meta-analysis of a broad range of self-management programs concluded that patients receiving self-management education had fewer hospital admissions than those receiving usual care. 10 Integrated case management, including self-management and accessibility to a specialized nurse case manager through a Web-based call center, has also been shown to improve outcomes in COPD. 11 Such programs generally rely on patients detecting deteriorations through worsening of their symptoms and responding according to a predefined action plan. It follows therefore that even earlier detection and treatment of COPD exacerbations may result in further improvements in health-related quality of life (HRQOL) and reductions in healthcare use and associated costs. Remote telemonitoring may allow patients and healthcare workers to identify such deteriorations earlier by regularly monitoring changes in physiological variables as well as in symptoms.
We designed a pilot randomized controlled trial to determine whether remotely monitoring symptoms, medication usage, and physiological variables daily over a 12-month period was feasible in patients with moderate to severe COPD and whether this intervention could improve quality of life or reduce healthcare use.
Subjects and Methods
Study Participants and Recruitment
Patients were recruited from a metropolitan tertiary-care hospital between June 2006 and April 2008. The Austin Hospital Research Ethics Committee approved the study, and all participants provided informed consent. Inclusion criteria were moderate to severe COPD based on COPDX 12 criteria, at least one hospital presentation in the last 12 months, English fluency, finger dexterity enabling use of keyboard and mouse, willingness to use a computer in health self-management, being ambulant, and living independently. Exclusion criteria were significant co-morbidities including cancer, renal failure, and cognitive impairment.
Subjects were recruited by offering enrollment to suitable new and existing patients of the Austin Hospital Chronic Disease Management Program. This program involves access to outreach nursing for patients with COPD (forced expiratory volume in 1 s [FEV1] <60%) who have had one or more hospital admissions in a 12-month period and are identified as being at risk for recurrent hospital admission. Patients fulfilling the inclusion criteria were contacted by phone and provided with both verbal and written information regarding the trial. The number of patients screened and reason for exclusion were recorded.
Study Design
Patients were randomly allocated to receive either standard best practice care (SBP) or SBP plus remote in-home telemonitoring (RM) for a 12-month period. Randomization was achieved using a set of sequentially numbered, opaque, sealed envelopes containing randomly generated “SBP” or “SBP+RM” designations. SBP included clinical management according to Australian and New Zealand Guidelines 12 with provision of outreach nursing, a written action plan, and availability of pulmonary rehabilitation. RM involved daily monitoring of spirometry, weight, temperature, blood pressure, oxygen saturation by pulse oximetry, electrocardiogram, sputum color and volume, symptoms, and medication usage.
Primary outcomes were hospital admissions, inpatient bed-days, and quality of life. Admission data were obtained by searching the Austin Hospital admissions database. Admissions to other hospitals were documented by SBP+RM patients using an electronic diary, whereas controls used written diaries. Confirmation of all patient-derived data regarding admissions was provided through general practitioner contact and through subsequent respiratory physician follow-up with the relevant hospital health information service. Hospital case-mix data were used to determine reason for admission and length of stay (LOS). Admissions were classified as COPD-related or non–COPD-related. Generic (Short Form 36 [SF-36] 13 ) and disease-specific (Chronic Respiratory Disease Questionnaire 14 [CRDQ]) quality of life questionnaires were completed at baseline and 6 and 12 months.
Secondary outcomes were 6-min walk distance (6MWD) measured at baseline and 12 months, adherence to daily monitoring, reproducibility of the physiological measurements, and patient acceptance of RM. Patient acceptance was assessed by the administration of a nonvalidated technology survey at the completion of the study that included questions relating to ease of use of the RM system, adequacy of technical support, whether patients felt RM helped them better manage their condition, and overall satisfaction with the RM system.
Procedures
The RM system (TeleMedCare system; Medcare, Sydney, Australia) comprised a laptop computer with digitally integrated blood pressure cuff and stethoscope, pulse oximeter, pneumotachograph for measurement of relaxed and forced spirometry, electrocardiogram touch plate, thermometer, and scales. The software provided a very simple user interface for guiding a patient through the series of measurements and was specifically designed for users with little or no computer experience. The system allowed patients to enter symptoms (visual analog scores measuring changes in overall health, dyspnea, sputum color and volume, symptoms of respiratory tract infection) and changes in medication usage (bronchodilators, inhaled and oral corticosteroids, and antibiotics).
Initial supervised domiciliary training was provided to all patients by a nursing informatics project manager not involved in the patients' clinical care. Ongoing in-home support was available if required. On-screen prompts were also available to help patients complete physiological measurements accurately and to remind them to complete the symptom and medication usage questionnaire. Data were uploaded daily to a central server via an Internet connection through the patient's telephone line.
Patients in the SBP+RM group performed measurements at a convenient set time daily. The quality of spirometry measurements was formally evaluated. This was assessed by determining the intersession reproducibility of the daily spirometric measures during a 4-week exacerbation-free period. Reproducibility was expressed as coefficient of variation.
Both the SBP+RM and SBP groups had access to nurse outreach via telephone if they felt unwell. RM data were reviewed 5 days weekly by a study nurse who had access to data trend graphs in order to aid detection of deterioration in any physiological parameter and to determine need for intervention. If there was a significant change in a variable (clinical alert), several management options were available to the study nurse, including contacting the study or local doctor, contacting nurse outreach, or contacting the patient to undertake a phone review and decide on best management (Fig. 1). The study nurse was able to request that the patient perform a repeat set of measurements that was available within 30 min to assist decision-making.
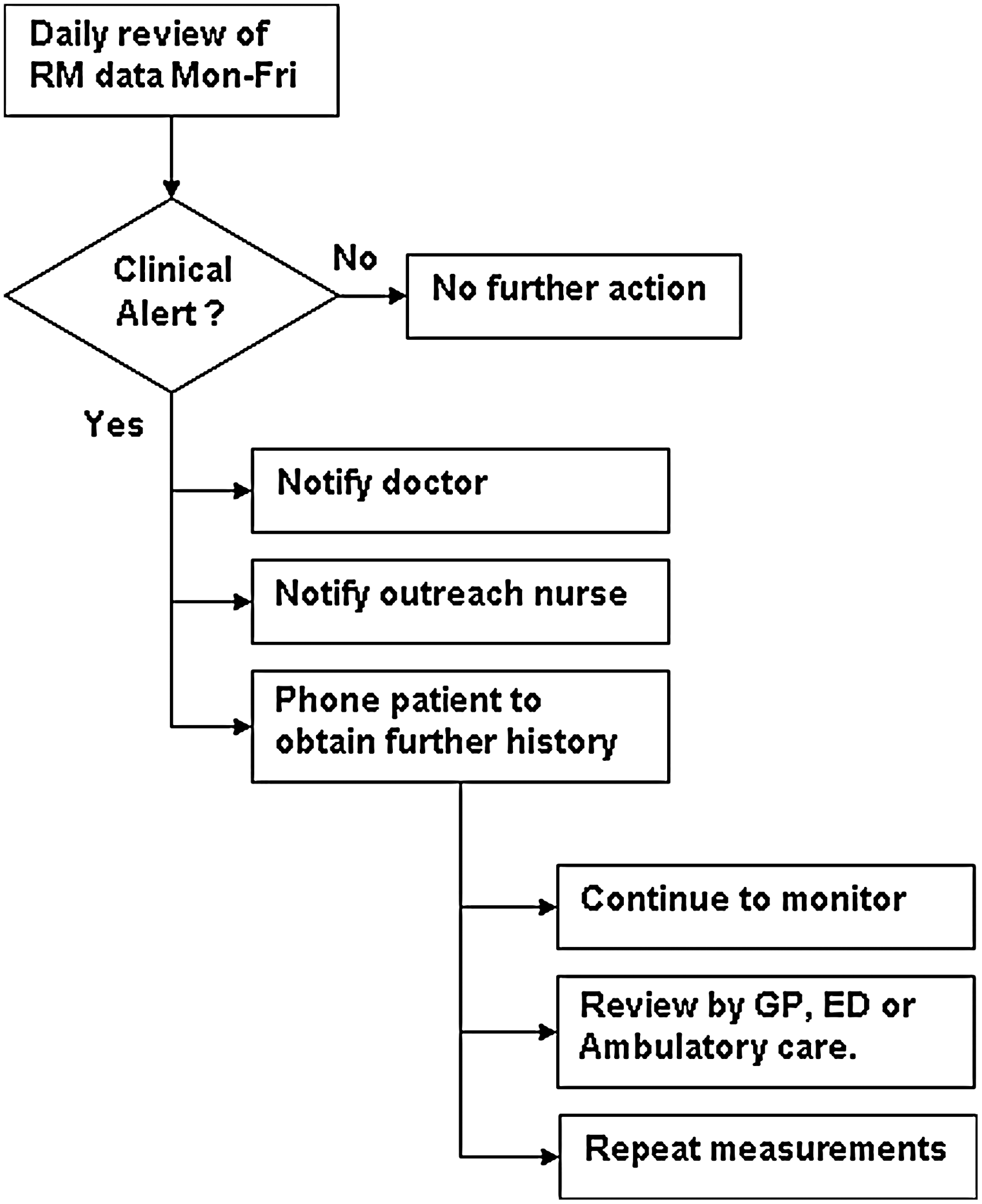
Flow diagram showing possible responses to abnormal trends in the remote in-home monitoring (RM) data. ED, emergency department; GP, general practitioner.
Statistical Analysis
All analyses were performed as intention to treat. Hospital admissions and LOS were analyzed using a Mann–Whitney test. Analysis of variance was used to assess differences in quality of life measures. Wilcoxon tests were used to detect differences in 6MWD between baseline and completion in each group, and Mann–Whitney tests were used to detect differences between the two groups.
Results
Study Subjects
Five hundred patients were screened, with 44 patients randomized: 22 to the SBP+RM group and 22 to the SBP group (Fig. 2). Baseline characteristics were similar between the two groups (Table 1), except for a higher incidence of active smoking and worse severity of airflow obstruction in the SBP group (p<0.05 for both). In each group similar numbers of patients had completed pulmonary rehabilitation prior to commencement of the study (13 in the SBP group and 12 in the SBP+RM group). They had completed pulmonary rehabilitation a mean of 14.3±19.8 months (SBP) and 24±21.5 months (SBP+RM) before commencement in the trial, with 2 subjects in each group undergoing pulmonary rehabilitation during the period of the trial, and 7 subjects in each group never having undergone pulmonary rehabilitation although being offered participation. Four patients withdrew from the SBP+RM group: 1 moved interstate, 1 was placed into residential care, 1 was diagnosed with cancer, and the final patient felt too unwell to continue. Two patients in the SBP+RM group died during the study: 1 with complications from terminal cancer (diagnosed after enrollment in the study) and the other with heart failure. Two patients withdrew from the SBP group: 1 to enter another trial and the other through feeling too unwell to continue. Thirty-six patients (16 SBP+RM and 20 SBP) completed the study. All patients, including those who withdrew, were included in the analysis.

Flow diagram showing the number of subjects screened, enrolled, and who completed the study. CDMP, Chronic Disease Management Program; RM+SBP, remote in-home monitoring + standard best practices care; SPB, standard best practices care.
Baseline Demographics and Clinical Characteristics
Data are mean (standard deviation) values for all variables other than admissions and length of stay (LOS), which are median (interquartile range). Admissions and LOS are for the 12-month period prior to recruitment.
6MWD, 6-min walk distance; COPD, chronic obstructive pulmonary disease; CRDQ, Chronic Respiratory Disease Questionnaire; FER, forced expiratory ratio; FEV1, forced expiratory volume in 1 s; FVC, forced vital capacity; NS, not significant; RM, remote in-home telemonitoring; SBP, standard best practice care; SF-36, Short Form 36 questionnaire.
Patient Measurements and Recordings
Although there were initial difficulties with the user interface for some SBP+RM subjects (for example, difficulties with telecommunications service providers, difficulties with data readability in tremulous older patients), most patients adapted well to the technology and to the need for performing daily measurements. The project manager visited the patient at home to resolve such difficulties.
SBP+RM patients were instructed to collect their data 7 days per week. These data were reviewed by the nurse monitor Monday–Friday over the course of the study, and reminders were sent as required. Overall compliance with the telemonitoring throughout the study was excellent, with median compliance for all daily measurements of around 80% (Table 2). Results for the evaluation of the quality of the patient-performed, home-based spirometry measurements are shown in Table 3, with a coefficient of variation for FEV1 of 7% in the convenience sample of the first 14 subjects recruited.
Adherence by Patients in the Remote In-Home Monitoring Group with Daily Measurements and Questionnaires over a 12-Month Period
Data are mean (interquartile range) values.
SpO2, pulse oximeter oxygen saturation.
Between-Session Coefficient of Variation for Spirometric Parameters Measured Daily over a 4-Week Exacerbation-Free Period in the First 14 Subjects Recruited
FEV1 and FEV6, forced expiratory volume in 1 and 6 s, respectively; FVC, forced vital capacity; IC, inspiratory capacity; PEF, peak expiratory flow; RR, respiratory rate; SD, standard deviation.
Hospital Presentations and LOS
There were no statistically significant differences in the number of COPD-related admissions/year, in COPD-related LOS days/year, total admissions/year, or total LOS days/year between the two groups over the 12-month period (Table 4).
Hospital Presentations and Length of Stay
Data are mean (standard deviation) values.
COPD, chronic obstructive pulmonary disease; LOS, length of stay; RM, remote in-home monitoring; SBP, standard best practice care.
Patients who received telemonitoring had a trend toward a decreased COPD-related admission rate (median [interquartile range] during the study period of 1 [0–2] admission/year) compared with the preceding 12-month period (2 [1–4] admissions/year) (p=0.052). This trend was not present in the SBP group (p=0.52).
HRQOL
There was no significant change in SF-36 or CRDQ (total) between baseline and measurements at 6 and 12 months within each group or between groups (Table 5). There were no significant differences between the groups for the dyspnea, emotion, fatigue, or mastery subscales of the CRDQ.
Health-Related Quality of Life
Data are mean (standard deviation) values. For the Chronic Respiratory Disease Questionnaire (CRDQ) and the Short Form 36 questionnaire (SF-36) a lower value represents better function.
NS, not significant; RM, remote in-home monitoring; SBP, standard best practices care.
Other Outcomes
There were no significant changes in the 6MWD in the SBP or SBP+RM groups over the 12-month period (Table 6), although there was a trend toward decline in the SBP+RM group between baseline and 12 months (mean [95% confidence interval] −28 [−65, 9] min). Ninety-four percent of patients found the home monitoring system easy to use, 82% felt the system helped them manage their COPD better, and the overall satisfaction rate was 88%. All patients felt the technical support they received was good. Adherence to measurements was excellent at a median of 80% overall. The between-session coefficient of variation for patient-performed spirometry was 7%.
Results for the 6-Min Walk Distance
Method for imputation: all missing values replaced with the group average value at that time point.
Statistically significant at the p<0.05 level.
ANOVA, analysis of variance; CI, confidence interval; RN, remote in-home monitoring; SBP, standard best practices care; SD, standard deviation.
Discussion
This pilot randomized clinical trial was designed to assess the feasibility of remotely monitoring several symptom-based and physiological variables in patients with moderate to severe COPD and to determine whether this would improve quality of life or reduce healthcare utilization. Patients' symptoms, medication usage, and several physiological variables, including daily spirometry, were monitored in an attempt to detect and treat exacerbations early.
The study revealed that use of telemonitoring to measure several variables on a daily basis over a 12-month period was feasible in this elderly group of patients with COPD, at least half of whom had no previous computer exposure. We demonstrated that patients are comfortable using home monitoring in their care, with 94% of patients describing the telemonitoring system as easy to use, 82% feeling the system helped them manage their COPD better, and an overall satisfaction rate of 88%. Adherence with measurements was excellent at a median of 80% overall. The between-session coefficient of variation we observed for patient-performed spirometry of 7% for FEV1 compares favorably with published data for in-laboratory spirometry in COPD performed with instruction by a laboratory scientist 15,16 and suggests that it is indeed possible for even severely impaired COPD patients to perform technically acceptable measurements of spirometry themselves in the home.
Although the trend of our results favors SBP+RM, we did not find statistically significant differences in admission rate, hospital presentation rate, or HRQOL between SBP+RM and SBP alone. The magnitude of the differences observed by the addition of RM to SBP was very small and of questionable clinical significance. This finding suggests that RM, when added to SBP, may not result in significantly improved outcomes in COPD patients.
An alternative explanation for our failure to observe a significant effect of RM could be related to the high quality of usual care provided to all patients involved in our study. In addition to adhering to established guidelines for management of COPD, admitted patients with COPD are referred to our Chronic Disease Management Program. This involves assessment by trained respiratory nursing staff, COPD-specific education, extensive social work, occupational therapy review, and close follow-up on discharge with access to outreach nursing. They are also assisted in developing a self-management plan. As such, results of this trial in a center where such multidisciplinary, coordinated chronic disease management is not the standard of care may have been different.
It is to be noted that in the current study the number of admissions fell substantially from the year before the study to the year of the study in the SBP+RM group but not in the SBP-only group. Closer matching of control and intervention groups in terms of numbers of prior hospital admissions/year may have yielded differing results.
Only 9% of patients screened were suitable for entry to our trial, with 37% of screened patients having significant non-COPD co-morbidities such as renal failure, cancer, dementia, or other cognitive impairment as their reason for noneligibility. Of the 456 patients excluded from entry to the trial, 15% were excluded because of language difficulties. Only 14% of patients refused, indicating a high level of willingness to consider using the technology. During 12 months of observation we did not find any change in HRQOL as measured by both generic and disease-specific assessment tools. Although patients in the SBP+RM group appeared to feel positively disposed to the RM system overall, as determined through our questionnaire, this did not translate into an improvement in their HRQOL. Conversely, there was no deterioration in HRQOL in either group, suggesting that the imposition of the RM equipment and its daily use did not impact adversely in these patients.
Although there has been increasing interest in telemedicine from healthcare organizations and clinicians alike, few robust data assessing clinically meaningful outcomes in patients with COPD exist. A recent systematic review and meta-analysis looking at telehealth (telephone support and telemonitoring) in COPD identified only nine studies for inclusion, and only four of these involved telemonitoring. 17 Clinical heterogeneity did not allow pooling of outcomes such as number of hospitalizations or hospital bed-days. Furthermore, the telemonitoring systems used varied among studies. Although three of the four included individual telemonitoring studies demonstrated reductions in hospitalizations and associated healthcare costs, 18 –20 these studies were not randomized clinical trials; hence their utility arguably remains unproven. Two more recent randomized controlled studies of telemedicine in COPD have been reported. Koff et al., 21 in a study over two jurisdictions in Leuven, Belgium, and Barcelona, Spain, showed a significant improvement in HRQOL with a trend toward decreased healthcare costs. However, in that study, remote home monitoring of symptoms and physiological variables was only one of four components of a “proactive integrated care program,” which also included disease-specific education, self-management education, and enhanced communication with study coordinators. Our results are similar to those reported in a Welsh study where, in a group of 40 subjects who had completed pulmonary rehabilitation and were already attended by a chronic disease management team, no significant differences were found in hospital admissions or in use of hospital or specialist community team resources in 20 patients receiving standard care plus telemonitoring for 6 months, followed by standard care for a further 6 months, compared with a control group. 22 In that study, as in ours, patients had access to specialist respiratory outreach services. In the study by Lewis et al., 22 there were fewer primary care contacts for chest problems in the telemonitoring group. We did not collect data on primary care attendances in the current study. The results of the current study, despite its limitations, are of significant importance given that, as in the study by Lewis et al., 22 they pertain specifically to remote telemonitoring added to best practice care, without other associated interventions.
Limitations of the Study
Use of the remote monitoring technology was demonstrated to be feasible in this elderly group of patients with COPD. However, it is noted that 37% of subjects screened were excluded because of significant cognitive impairment or other significant co-morbidities, so this feasibility may not pertain to the wider group of patients with COPD. The two groups in our study were well matched at baseline except in terms of severity of airflow obstruction and current smoking status. The SBP group had worse airflow obstruction and more current smokers. This may have been expected to increase the frequency and severity of exacerbations and consequent hospitalizations in this group, given that exacerbations increase in frequency and severity with severity of COPD 23 and also that smoking cessation reduces exacerbation risk. 24 The a priori sample size determined to be required to detect a difference of one admission per year between the two groups was 128 subjects (0.8 power, p=0.05, two sided). It is not surprising that our observed effect size of 0.2 admissions/year was not statistically significant, because of both its small magnitude and the relatively low numbers of subjects ultimately entered in this study.
A further limitation is that telemonitoring was compared in this study with SBP, which, in this tertiary-care referral institution, includes many features not necessarily available in other centers, including respiratory outreach nursing, post-acute care physiotherapy and nursing review, and inpatient and outpatient pulmonary rehabilitation. Comparison of the intervention with standard care in another jurisdiction may have yielded differing results. A cost analysis of the intervention was beyond the scope of the study. Although there was no significant difference in admissions or LOS, patients who were remotely monitored incurred the added costs of the telemonitoring unit and of the clinical team reviewing and analyzing their data. We did not collect data relating to other healthcare costs such as outpatient and general practitioner visits as well as nurse outreach time. It could be argued that daily monitoring of symptoms and physiological data might result in a greater number of healthcare interventions.
Conclusions
We demonstrated, as have others, that patients are comfortable using home monitoring in their care. Despite more than 50% of patients not having previously used a computer or having a computer at home, the majority of our study patients found the system easy to use, and the adherence to monitoring over 12 months was excellent, with 80% adherence to physiological monitoring and 73% adherence to symptom monitoring. Previous studies have similarly demonstrated patient acceptance of such technology but, in the absence of rigorous design, have suggested benefits that were not demonstrated in this small randomized controlled trial. We were also able to show that, after initial instruction, patients are able to perform a battery of unsupervised physiological measures with good reliability, further supporting the feasibility of this technology. The absence of significant reductions in admission rate, LOS, and quality of life we observed between SBP and SBP+RM suggests that it is likely that RM, at least in the implementation model we studied, may not improve on standard care. It remains to be seen whether other approaches using RM in models of COPD care prove to be beneficial in disease management.
Footnotes
Acknowledgments
This work was supported by the Department of Human Services, Victoria, Australia.
Disclosure Statement
No competing financial interests exist.