
Abstract
Introduction
The Joslin Vision Network Diabetes Eye Care Program (JVN) is an American Telemedicine Association category 3 telemedicine program developed at the Joslin Diabetes Center. 1,2 The JVN has been validated to identify clinical Early Treatment Diabetic Retinopathy Study (ETDRS) levels of diabetic retinopathy (DR) and diabetic macular edema (DME) comparable to grading of gold standard 35-mm ETDRS seven-standard field stereo color fundus photographs (ETDRS photographs). 3 The JVN also closely matches clinical examination for determining severity levels of DR and DME 2 and is able to identify non–diabetes-related retinal eye disease within JVN fields comparably to dilated retinal examination by a retinal specialist. 4 The JVN relies on a validated protocol for remote image capture, image transmission to a central reading center for evaluation, DR severity assessment, and a comprehensive diabetes eye care plan based on retinal findings and the patient's medical history. 3 Over the past 10 years, nearly 2 million retinal images have been captured using the JVN protocol.
A barrier to remote nonmydriatic retinal imaging is the high flash exposures needed for adequate retinal image quality using currently available high-resolution digital cameras. The amount of light falling on a given pixel is determined by the illumination flash exposure, the magnification of the retinal image, and the number of pixels in the light-sensitive area. Increased pixel resolution or a greater number of pixels per light-sensitive surface area of the detector, assuming constant flash exposure and magnification, means that less light falls on each available pixel. Thus, in the case of commercially available megapixel cameras, the amount of flash exposure required for an adequate quality retinal image begins to result in a constrictive pupillary response, added discomfort for the patient, and increased time required to acquire the protocol defined retinal fields. The MegaVision E1-i-RIC (retinal image capture) (MegaVision, Santa Barbara, CA) digital camera back is optimized with respect to pixel resolution and low light level capability for nonmydriatic retinal imaging and is designed specifically for the JVN protocol of nonmydriatic retinal imaging with a low-power xenon flash illuminant. The digital camera back is interfaced with the Topcon® NW6S nonmydriatic fundus camera (Topcon Medical Systems, Oakland, NJ), and the system provides 1,000×1,000 pixel resolution at low light level output of 1.7 W-s or 1.3 mW per exposure (approximately five times lower than other currently commercially available systems). The low light exposure improves patient comfort and reduces flash-induced miosis, reducing image acquisition time while maintaining adequate image quality and resolution. MegaVision's calibrated color system enables custom renderings to achieve optimum diagnostic quality.
This study compares the clinical ETDRS level of DR and DME graded from nonmydriatic digital images acquired using the Topcon NW6S camera interfaced with the MegaVision E1-i-RIC camera back (MegaVision images) with both mydriatic ETDRS photographs and mydriatic clinical examination by a retina specialist. Subject comfort and image acquisition time were compared with those of mydriatic ETDRS photography using the Zeiss FF3 fundus camera (Carl Zeiss Meditec, Inc., Dublin, CA).
Subjects and Methods
The Internal Review Board of the Joslin Diabetes Center (Boston, MA) approved the study protocol. Informed consent was obtained from each patient, and the study was conducted in accordance with the Health Insurance Portability and Accountability Act and the tenets of the Declaration of Helsinki. The study was conducted at the Beetham Eye Institute of the Joslin Diabetes Center. Patients over 18 years of age with either type 1 or type 2 diabetes scheduled for eye examination at the Beetham Eye Institute were invited to participate. Record review determined the most recently diagnosed level of DR, and recruitment was stratified by DR severity so that eyes with a wide range of DR severity were included, from no DR (ETDRS level 10) to high-risk proliferative DR (ETDRS level 75). 5 Exclusion criteria included a history of conditions in either eye that may preclude pupil dilation, use of mydriatic or miotic eye drops that would alter pupil size or reactivity, and prior laser treatment or media opacities precluding adequate imaging of the retina.
Patients were enrolled in the study during their regular visit to the Beetham Eye Institute. Each patient underwent nonmydriatic retinal imaging using the Topcon NW6S camera interfaced with the MegaVision digital camera back according to the standard JVN protocol, 6 and images were stored in the JVN database for subsequent review. The JVN imaging protocol has been previously published 3,6 and includes three 45° stereoscopic fields (centered between the optic disc and macula, along the superior temporal vascular arcade, and nasal and slightly inferior to the optic disc), two 30° stereoscopic fields (centered on the optic disc and centered on the macula, corresponding approximately to ETDRS standard fields 1 and 2), and an external image of each eye. After JVN imaging, pupils were dilated with 1% tropicamide and 2.5% phenylephrine hydrochloride. ETDRS seven-standard field stereo 35-mm film photographs according to the ETDRS protocol (ETDRS photographs) 7 were acquired from each eye followed by a dilated retinal examination performed by a retina specialist.
Each eye was assessed according to the ETDRS extension of the Modified Airlie House Classification of DR for the presence and severity of specific lesions of DR and DME. 7,8 Two independent masked readers graded each set of images (ETDRS photographs [P.S.S.] and MegaVision images [J.D.C.]). The retinal findings for both ETDRS photographs and MegaVision images were recorded on the JVN electronic medical record grading templates according to already established and validated JVN grading protocols. 3 The ETDRS clinical level of DR and DME was compared between MegaVision images and ETDRS photographs, and disagreements between the two independent graders were adjudicated by a senior retina specialist (L.M.A.).
Development of JVN Protocol-Specific Automated Image Rendering
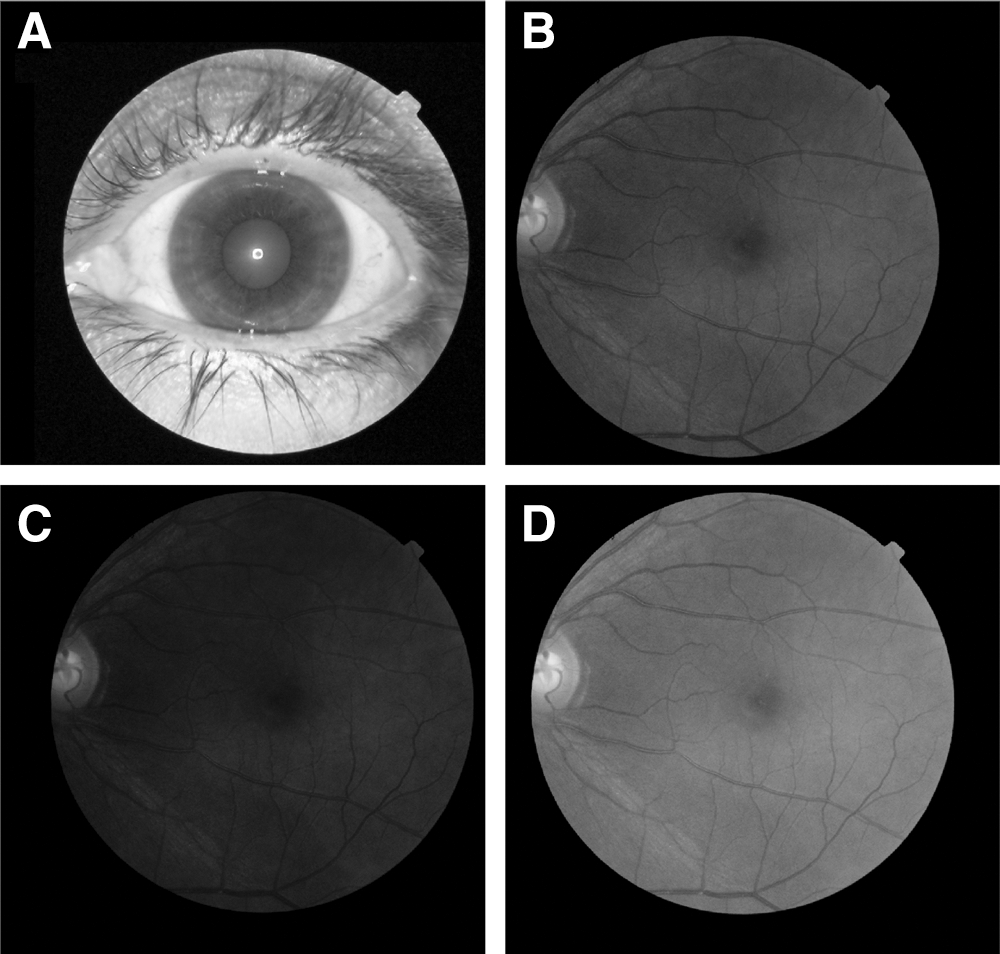
One of the key advantages of the MegaVision camera back is the use of automated image color rendering that allows the use of low levels of flash output while maintaining image quality, thereby avoiding excessive miosis following image capture. Additionally, images for review can be adjusted for optimal tonal balance for predetermined fundus pigmentations that facilitate review of retinal images of diverse populations (Fig. 1).
MegaVision automated color rendering:
The JVN protocol requires that multiple nonmydriatic images be captured in a session. This requirement, in turn, requires that the light be limited to a very low level (1.7 W-s on the Topcon NW6S camera). Image quality degrades rapidly with less light, and acquiring color images at this low light level requires optimization of the camera sensor and optics. The main cause of image degradation is not a reduction in the overall light falling on the sensor but rather the ratio of the amount of light to the number of pixels. As the number of pixels decreases, the light to pixel ratio increases for a fixed amount of light, increasing signal/noise and leading to an improvement in tonal resolution. However, as the number of pixels decreases beyond an optimal point, the reduction in spatial resolution will degrade the image. Based on the light levels required by multiple image acquisition of the JVN protocol, the optimal amount of spatial resolution and tonal resolution was determined to be in the 1 megapixel range.
Calibration of the image acquisition system and viewing systems was done in accordance with International Color Consortium protocols and standards to ensure accurate and uniform response to signal inputs. Optimum image rendering was adjusted to accommodate for a range of different fundus pigmentations. The different degrees of fundus pigmentations were grouped based on the amount of light that differently pigmented retinas reflected. The lightest pigmented fundi can reflect up to three stops more light than the darkest pigmented fundi. To improve imaging, this range was taken into account by having the imager identify a patient's eye color prior to image capture and then using that information to optimize the image capture.
Statistical Analysis
The adjudicated grades derived from the ETDRS images were considered the reference standards. The clinical ETDRS level of DR severity and the presence/absence of DR lesions were compared. Agreement between clinical ETDRS level of DR severity between MegaVision images and ETDRS photographs was cross-tabulated, and both unweighted (κ) and weighted (using a linear scheme) (κw) κ values were calculated. Images classified as ungradable were excluded from the analysis. Guidelines for interpretation of κ statistics were based on the recommendations of Landis and Koch 9 as used in ETDRS Report Number 10 (0.0–0.2=slight agreement, 0.21–0.40=fair agreement, 0.41–0.60=moderate agreement, 0.61–0.80=substantial agreement, and 0.81–1.00=almost perfect agreement). 7 All statistical analyses were performed using SAS (version 9.2) software (SAS, Inc., Cary, NC).
Results
In total, 126 eyes from 67 diabetic subjects were included in the study. Four subjects (8 eyes) did not complete the study and were excluded from the analysis. There was no indication that these subjects differed from the remaining subjects evaluated in this study. The mean age of the subjects participating in the study was 49 years (range, 24–83 years), and 79.1% (53) reported white ethnicity. The demographic data of the study population are summarized in Table 1.
Demographic Data of the Study Population
Four patients did not complete the study and were excluded, leaving 67 patients for analysis. The excluded patients did not differ significantly for the cohort evaluated.
DM, diabetes mellitus; SD, standard deviation.
A single independent masked reader (P.S.S.) evaluated the ETDRS photographs for the presence and severity of DR and DME. DR was identified in 113 eyes (89.7%), no DR was identified in 13 eyes (10.3%), and no images were ungradable based on ETDRS photographs. A separate independent senior masked reader experienced in grading nonmydriatic 45° retinal images (J.D.C.) evaluated the MegaVision images for the presence and severity of DR and DME. Agreement between the two readers with regard to grading retinopathy level has previously been demonstrated to have substantial to almost perfect agreement (internal reading center quality control, κ=0.80±0.13, κw=0.95±0.04). DR was detected in 116 eyes (92.1%), no DR was identified in 10 eyes (7.9%), and images from 3 eyes (2.4%) could not be graded. Comparing DR severity levels identified between the MegaVision images and ETDRS photographs, respectively, 27 eyes (21.4%) versus 24 eyes (19.1%) were identified with mild nonproliferative DR (NPDR), 35 eyes (27.8%) versus 36 eyes (28.6%) had moderate NPDR, 20 eyes (15.9%) versus 18 eyes (14.3%) had severe NPDR, 1 eye (0.8%) in each group had very severe NPDR, 12 eyes (9.5%) versus 16 eyes (12.7%) had proliferative DR (PDR) less than high-risk criteria, 3 eyes (2.4%) in each group had PDR greater than high-risk criteria, and 15 eyes (11.9%) in each group had quiescent PDR. MegaVision images were ungradable in 3 eyes (2.4%), and all ETDRS photographs were gradable. After the 3 eyes with ungradable MegaVision images were excluded, exact agreement for level of DR between MegaVision images and ETDRS photographs was observed in 82% of eyes (95% confidence interval [CI]=0.75–0.98) and agreement was within 1 step of DR severity in 92% of eyes (95% CI=0.86–0.96). The distribution of DR severity using the MegaVision images and ETDRS photographs is summarized in Table 2. The sensitivity, specificity, positive predictive values, and negative predictive values to DR and DME thresholds are summarized in Table 3.
Cross-Tabulation of Level of Diabetic Retinopathy in MegaVision Images and 35-mm Early Treatment Diabetic Retinopathy Study Photographs
These measures did not include eyes that could not be graded by MegaVision and 35-mm Early Treatment Diabetic Retinopathy Study (ETDRS) photographs, so that only 123 eyes were included.
Entries in bold indicate perfect agreement: 82% (95% confidence interval 75–98%). Entries in italics indicate within one-step agreement: 92% (95% confidence interval 86–96%). The simple κ statistic was 0.81 (95% confidence interval 0.73–0.89); the weighted κ statistic (linear scale) was 0.89 (95% confidence interval 0.83–0.95).
DR, diabetic retinopathy; NPDR, nonproliferative diabetic retinopathy; PDR, proliferative diabetic retinopathy.
Comparison by Different Diabetic Retinopathy and Diabetic Macular Edema Thresholds: 35-mm Early Treatment Diabetic Retinopathy Study Photographs Compared with MegaVision Images, with Ungradable Eyes Excluded
CI, confidence interval; CSME, clinically significant macular edema; DME, diabetic macular edema; DR, diabetic retinopathy; NPDR, nonproliferative diabetic retinopathy; SE, standard error.
There was substantial agreement between the level of DR identified in MegaVision images and ETDRS photographs with a κ of 0.81 (95% CI=0.73–0.89) and κw=0.89 (95% CI=0.83–0.95). MegaVision images had a positive predictive value of 0.92 for determining presence of DR and a positive predictive value of 0.92 for determining the presence of sight-threatening DR (severe NPDR or worse). There was a trend for MegaVision images to overdiagnose severe NPDR (15.9% versus 14.3%) and underdiagnose early PDR (9.5% versus 12.7%) due to the differences in the retinal fields covered by the two imaging systems (Table 2). The MegaVision “overdiagnosis” of severe NPDR was due to the presence of more severe nonproliferative retinal changes in the fields not covered by the ETDRS photographs. This difference in fields is even more striking in patients “underdiagnosed” with PDR by MegaVision because in 60% of these patients the diagnosis of PDR was missed owing to the presence of neovascular lesions in the inferotemporal quadrant, which is not covered by the JVN fields. Subgroup analysis of eyes with PDR and new vessels elsewhere located within the JVN fields demonstrated an exact match between MegaVision and ETDRS photographs in all cases. The negative predictive value was 1.00 for the presence of any level of DR and 0.94 for the presence of sight-threatening DR.
Fundus examination by a retina specialist identified DR in 114 patients (90.5%) and absence of DR in 12 patients (9.5%). An exact match with MegaVision images was seen in 76% eyes (95% CI=68–84) and within 1 step in 91% eyes (95% CI=85–95). Substantial agreement between the MegaVision images and clinical examination was observed (κ=0.71 [95% CI=0.62–0.80] and κw=0.81 [95% CI=0.73–0.89]). As it was for ETDRS photographs, a trend for “overdiagnosis” of severe NPDR with MegaVision images compared with clinical examination was similarly observed. The distribution of DR severity evaluated using the MegaVision images and clinical examination is summarized in Table 4.
Cross-Tabulation of Level of Diabetic Retinopathy in MegaVision Images and Dilated Retinal Examination
These measures did not include eyes that could not be graded by MegaVision and 35-mm Early Treatment Diabetic Retinopathy Study (ETDRS) photographs, so that only 123 eyes were included.
Entries in bold indicate perfect agreement: 76% (95% confidence interval 68–84%). Entries in italics indicate within one-step agreement: 91% (95% confidence interval 85–95%). The simple κ statistic was 0.71 (95% confidence interval 0.62–0.80). The weighted κ statistic (linear scale) was 0.81 (95% confidence interval 0.73–0.89).
DR, diabetic retinopathy; NPDR, nonproliferative diabetic retinopathy; PDR, proliferative diabetic retinopathy.
Comparing MegaVision images with ETDRS photographs (Table 5) for the presence and severity of DME, respectively, 55 (43.7%) versus 61 (48.4%) eyes had no DME, 1 (0.8%) had questionable DME in each group, 37 (29.4%) versus 41 (32.5%) eyes had DME less than clinically significant macular edema (CSME), and 19 (15.1%) versus 22 (17.5%) eyes had CSME. Comparing MegaVision to clinical examination for the presence and severity of DME (Table 6), respectively, 55 (43.7%) versus 76 (60.3%) eyes had no DME, 1 (0.8%) versus none had questionable DME, 37 (29.4%) versus 31 (24.6%) had DME less than CSME, and 19 (15.1%) eyes had CSME in each group. Substantial agreement was observed for DME grading with ETDRS photographs (κ=0.92 [95% CI=0.87–0.98], κw=0.95 [95% CI=0.90–1.00]) and moderate agreement with clinical examination (κ=0.58 [95% CI=0.46–0.71], κw=0.66 [95% CI=0.55–0.78]). Using MegaVision imaging, the positive predictive value for accurately determining DME was 1.00 and 0.89 for CSME. The negative predictive value for DME was 0.98 and 0.97 for CSME (Table 3).
Cross-Tabulation of Level of Diabetic Macular Edema in MegaVision Images and 35-mm Early Treatment Diabetic Retinopathy Study Photographs
These measures did not include eyes that could not be graded by MegaVision and 35-mm Early Treatment Diabetic Retinopathy Study (ETDRS) photographs, so that only 112 eyes were included.
Entries in bold indicate perfect agreement: 96% (95% confidence interval 90–98%). Entries in italics indicate within one-step agreement: 99% (95% confidence interval 95–100%). The simple κ statistic was 0.92 (95% confidence interval 0.87–0.98); weighted κ statistic (linear scale) was 0.95 (95% confidence interval 0.90–1.00).
CSME, clinically significant macular edema; DME, diabetic macular edema.
Cross-Tabulation of Level of Diabetic Macular Edema in MegaVision Images and Dilated Retinal Examination
These measures did not include eyes that could not be graded by MegaVision and 35-mm Early Treatment Diabetic Retinopathy Study (ETDRS) photographs, so that only 112 eyes were included.
Entries in bold indicate perfect agreement: 75% (95% confidence interval 66–83%). Entries in italics indicate within one-step agreement: 87% (95% confidence interval 79–92%). The simple κ statistic was 0.58 (95% confidence interval 0.46–0.71); the weighted κ statistic (linear scale) was 0.66 (95% confidence interval 0.55–0.78).
CSME, clinically significant macular edema; DME, diabetic macular edema.
The time for image acquisition was calculated from the initial nonmydriatic image to the final nonmydriatic image using the Topcon NW6S camera interfaced with the low-light-adapted MegaVision digital camera back compared with the image acquisition time of standard mydriatic seven-standard ETDRS stereoscopic images using the Zeiss FF3 camera. The mean time taken to acquire 22 MegaVision images from both eyes was 9:52 min (data available for 61 patients). For ETDRS photographs, images were obtained after pharmacological mydriasis. A previous study has shown that the time for pupillary dilatation for 95% patients with 1 drop each of 1% tropicamide and 10% phenylephrine hydrochloride is 20 min. 8 Adding this to the image acquisition time for ETDRS photographs, the total time for ETDRS photographs was 27 min, not including image sorting and slide processing.
To ascertain the subjective comfort with low flash output from MegaVision imaging, a subset of 10 patients was imaged with the Topcon NW6S camera interfaced with the low-light MegaVision digital camera back using two flash settings (1.7 or 3.3 W-s) that were presented in random order to the subjects. Six subjects (60%) found the lower flash setting of 1.7 W-s more comfortable, 3 (30%) found no difference in the comfort level between the two flash outputs, and only 1 (10%) subject preferred the higher flash output.
An important step in the JVN-MegaVision image analysis process was the integration of automated image rendering into the retinal image evaluation protocol. This automated process involved adjusting the gamma curve of the retinal images according to predetermined steps based on retinal pigmentation (Fig. 1). This process was in addition to the standard image manipulation capabilities available in the JVN image evaluation software (JVN reader version 4.0, Joslin Diabetes Center), which included manual dynamic rendering, digital magnification, red-free images, and side-by-side image comparisons. To determine the effect of automated rendering on the quality and ungradable rate of nonmydriatic images, a retrospective review of all JVN–Joslin Diabetes Center images taken with the MegaVision camera was performed. Images taken from January 1, 2008 to December 31, 2008 (n=8170 eyes) that did not undergo automated image rendering were compared with images taken from January 1, 2010 to December 31, 2010 (n=6962 eyes), where automated image rendering had been integrated into the protocol. In the JVN–Joslin Diabetes Center teleophthalmology program retinal images were taken from diabetes patients, including those with cataracts and small pupils. The ungradable rate for images that did not undergo the automated rendering process was 14.2% (n=1164) for DR and 15.6% (n=1272) for DME compared with 11.2% (n=783) for DR and 11.8% for DME (n=824) for images that were rendered based on retinal pigmentation, representing a 21.1% (p<0.0001) and 24.5% (p<0.0001) improvement rate, respectively.
Discussion
The prevalence of DR and vision-threatening DR among adults with diabetes in the United States is estimated at 28.5% and 4.4%, respectively. 10 It has been shown that careful and appropriately spaced regular retinal evaluations for DR can be cost-effective in terms of number of sight-years saved and federal budget savings. 11 –15 A previous study has demonstrated that the JVN telemedicine program accurately determines the level of retinopathy equivalent to ETDRS photographs or a clinical examination and can potentially be more effective than clinical examination for detecting PDR and averting cases of severe vision loss and may do so at lower cost. 16 Implementing this retinal imaging technology in a primary care setting has been shown to result in a significant increase in the rate of DR surveillance along with an increase in the rate of laser treatment for DR for a large patient population. 17
The MegaVision digital camera back was developed for JVN, specifically for nonmydriatic capture of multiple retinal fields using a minimal amount of flash. Interfaced with the Topcon NW6S camera, the digital camera back has been optimized for low light exposure while maintaining adequate image resolution for detecting the small retinal lesions such as hemorrhages and microaneurysm. The low flash output limits miosis, allowing the rapid capture of successive retinal images without degrading the quality of images that might obscure subtle pathology or cause undue difficulty to the retinal imager and prolong the imaging session. The image resolution has been maintained by high sensitivity, low noise, electronic shuttering, and optical filtration. The quality of the nonmydriatic digital retinal images is further enhanced by the use of automated image rendering based on retinal pigmentation in addition to standard digital image manipulation, which is not possible with nondigital formats. This feature resulted in more than a 20% reduction in ungradable images.
The major source of discrepancy between the MegaVision images and ETDRS photographs was attributable to differences in field size (45° compared with 30° fields) and definition (two compared with four peripheral fields) between the two modalities. Previous studies have shown that the sensitivity of DR detection depends on the area of the retina imaged 18 ; however, there is no consensus on the number of fields and the area of retina that should be imaged in order to find all DR lesions and/or to accurately determine the actual level of DR most efficiently. Various studies have confirmed that the use of three 45° fields is more sensitive for detection of DR compared with a single 45° field image. 18 –20 Other authors argue that two 45° fields each centered on disc and macula are most effective for population-based DR evaluation and that addition of further fields may result in diminished utility and cost-effectiveness of the approach. 21,22 In this current study, about 60% of proliferative lesions located inferotemporally that were identified in Field 5 of the ETDRS photographs were not imaged by MegaVision, and the DR severity level for these eyes was not accurately determined. In contrast, compared with the 30° field of ETDRS photographs, the wider 45° field of the MegaVision images identified more extensive nonproliferative changes in the periphery of about 27%, contributing to a diagnosis of a more severe level of retinopathy. These findings stress the importance of a wider imaging field and the importance of including peripheral retinal areas to detect otherwise overlooked DR lesions.
The results of this validation study suggest that MegaVision retinal images when evaluated with a rigorous reading protocol using automated image rendering and manual dynamic image rendering compare favorably with ETDRS photographs and clinical examination by a retina specialist for grading of DR and DME. When evaluated in this fashion, these images show substantial agreement with ETDRS photographs in determine clinical DR severity. Furthermore, they detect more retinal disease than dilated retinal expert clinical examination alone. These findings provide further support that the inclusion of more peripheral fields and the use of image rendering increase the detection of DR lesions and suggest that the use of nonmydriatic digital wide-field retinal imaging may lead to more accurate overall DR assessment.
Conclusions
The role of telemedicine initiatives in the delivery of diabetes eye care has been increasing over the past 10 years. With substantial developments in information technology infrastructure, image acquisition systems, and automated algorithms, it has the potential to expand access to and the delivery of care, disseminate validated clinical care standards, and allow patients to participate more fully in their healthcare. 23 DR progresses through defined severity levels, making it ideal for telemedicine approaches that can accurately assess the level of retinopathy severity. Telemedicine retinal evaluation also improves patient compliance with subsequent follow-up examinations for DR. 24,25
The Topcon NW6S camera interfaced with the low-light-optimized MegaVision E1-RIC digital camera back used for JVN telemedicine program allows multiple retinal fields to be acquired through nonmydriatic pupils while accurately assessing the level of DR and DME equivalent to ETDRS photographs or a retinal examination by a retinal specialist. In addition, these images cover more retinal area and are acquired at low flash outputs, at faster speed, and with improved patient comfort. These data support several potential benefits of using low-light-optimized digital camera backs with standard nonmydriatic retinal cameras to accurately assess severity of DR and DME in patients with diabetes.
Footnotes
Acknowledgments
This work was funded in part by Department of the Army by means of Cooperative Agreement DAMD 17-03-2-0062 and the Massachusetts Lions Eye Research Fund for the Joslin Vision Network.
Disclosure Statement
No competing financial interests exist. The authors have no financial relationship with MegaVision.