
Abstract
Introduction
Utilizing communication technology, teledermatology is the practice of delivering dermatologic care remotely. 1 –4 The two primary forms of teledermatology are live-interactive and store-and-forward teledermatology (S&F). 1,5,6 Teledermatology has been used to provide increased specialty access for medically underserved populations such as those in rural areas. 1,7
Among those states that reimburse for S&F and LI teledermatology, California possesses the highest volume of teledermatology referrals as well as the most practicing teledermatologists. 8 To assess the effectiveness of teledermatology operations in California, it is important to understand how the needs of the California Medicaid (Medi-Cal) population are served through teledermatology. Specifically, comprehending this issue as well as its associated challenges from the referring providers' perspective is crucial to encouraging further teledermatology consultations.
To explore the perspective of primary care providers (PCPs) on the impact of teledermatology on the Medi-Cal population, we conducted hour-long one-on-one interviews with 10 PCPs who refer patients to teledermatology regularly, with an average aggregate referral base of 2,760 teledermatology cases annually. We examined the PCPs' viewpoints regarding their operational considerations associated with referring to teledermatology services, the value of offering such services, and challenges to ensuring a successful teledermatology operation. Their responses act as a starting point for identifying policy recommendations and practice improvements that would enable wider adoption of teledermatology referrals among PCPs and could improve current referring providers' practices.
Subjects and Methods
Study Setting
This study was approved by the Institutional Review Board at the University of California Davis (Sacramento, CA). The Center for Connected Health Policy provided a list of PCPs who currently refer patients to telemedicine through the Specialty Care Safety Net Initiative. To obtain this list, the Center for Connected Health Policy also utilized the following means: working with California Primary Care Association to obtain information from safety net providers and contacting two professional societies relevant to teledermatology, including the (1) American Telemedicine Association (ATA) Teledermatology Special Interest Group and (2) the Telemedicine Task Force of the American Academy of Dermatology, to identify pertinent PCPs in California. The resulting list of PCPs regularly refer patients to telemedicine in California and serve the Medicaid population. The research team sorted the list based on referral volume of the PCPs and contacted those PCPs who referred the highest volume of patients to teledermatology in the order of referral volume with each PCP referring at least several patients per month. In total, 14 PCPs were contacted; 10 agreed to participate, and four declined participation.
Instrument Development and In-Depth Interviews
Between September 1, 2010 and March 30, 2011, we conducted in-depth hour-long interviews with PCPs in California who regularly refer patients to teledermatologists. The interview questions were developed by the authors in collaboration with the committee members from the ATA Teledermatology Special Interest Group and the Medi-Cal Policy section of the California Department of Health Care Services. The interview questions were revised in four iterations to ensure internal, external, and face validity. These interviews were conducted by two interviewers, and the responses from the PCPs were transcribed. The interview questions that the study team asked the PCPs focused on the following key areas: (A) demographic factors of PCPs and their patients, (B) operational considerations pertinent to the PCP's participation in teledermatology referral, and (C) value and challenges of providing teledermatology services.
Results
Demographic Factors of Referring PCPS and their Patients
We conducted hour-long one-on-one interviews with 10 PCPs who refer patients to teledermatology regularly and who serve an average aggregate referral base of 2,760 teledermatology cases yearly. Eighty percent of surveyed PCPs reported that they practiced in Federally Qualified Health Centers. In regard to their patient demographics, the PCPs reported that their patients are from diverse racial and ethnic backgrounds, are primarily indigent by federal standards, and are uninsured or underinsured. The average insurance distribution of their overall patient population is displayed in Figure 1.
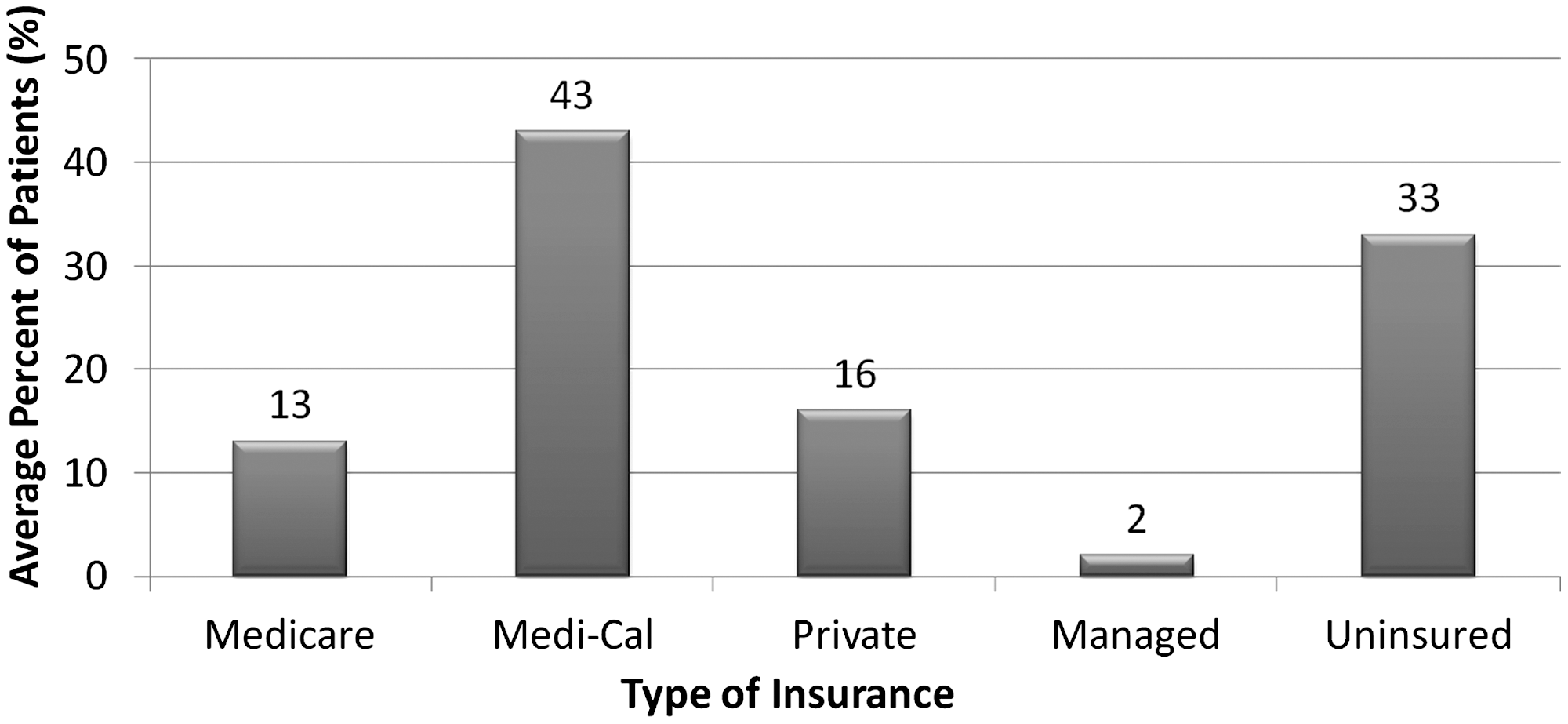
Insurance distribution of patient population served by primary care providers. Medi-Cal, California Medicaid.
When asked how they spent their time professionally, this group of PCPs reported that they spent a mean of 74% of their professional time in general medicine, 4% of their time in teledermatology, and 17% of their time in administration. The PCPs reported that they have been engaged in teledermatology in California for a mean of 4.79 years (standard deviation±5 years). Eighty percent of PCPs reported using S&F teledermatology, and 20% of PCP reported using LI teledermatology. Of the 80% of PCPs who have been involved with S&F teledermatology, 62% have received formal training in telemedicine.
Teledermatology Operational Considerations
When asked, 100% of PCPs responded that increasing access for their patients was the primary reason that they participated in teledermatology.
Factors influencing teledermatology referral
We asked PCPs the proportion of patients with skin diseases that they refer to dermatologists versus managing these skin conditions themselves (Fig. 2). On average, the PCPs reported referring 23 patients to teledermatology in 1 month. The PCPs reported that the top conditions they refer to teledermatology were unknown rashes, skin lesions suspicious for malignancy, and psoriasis.
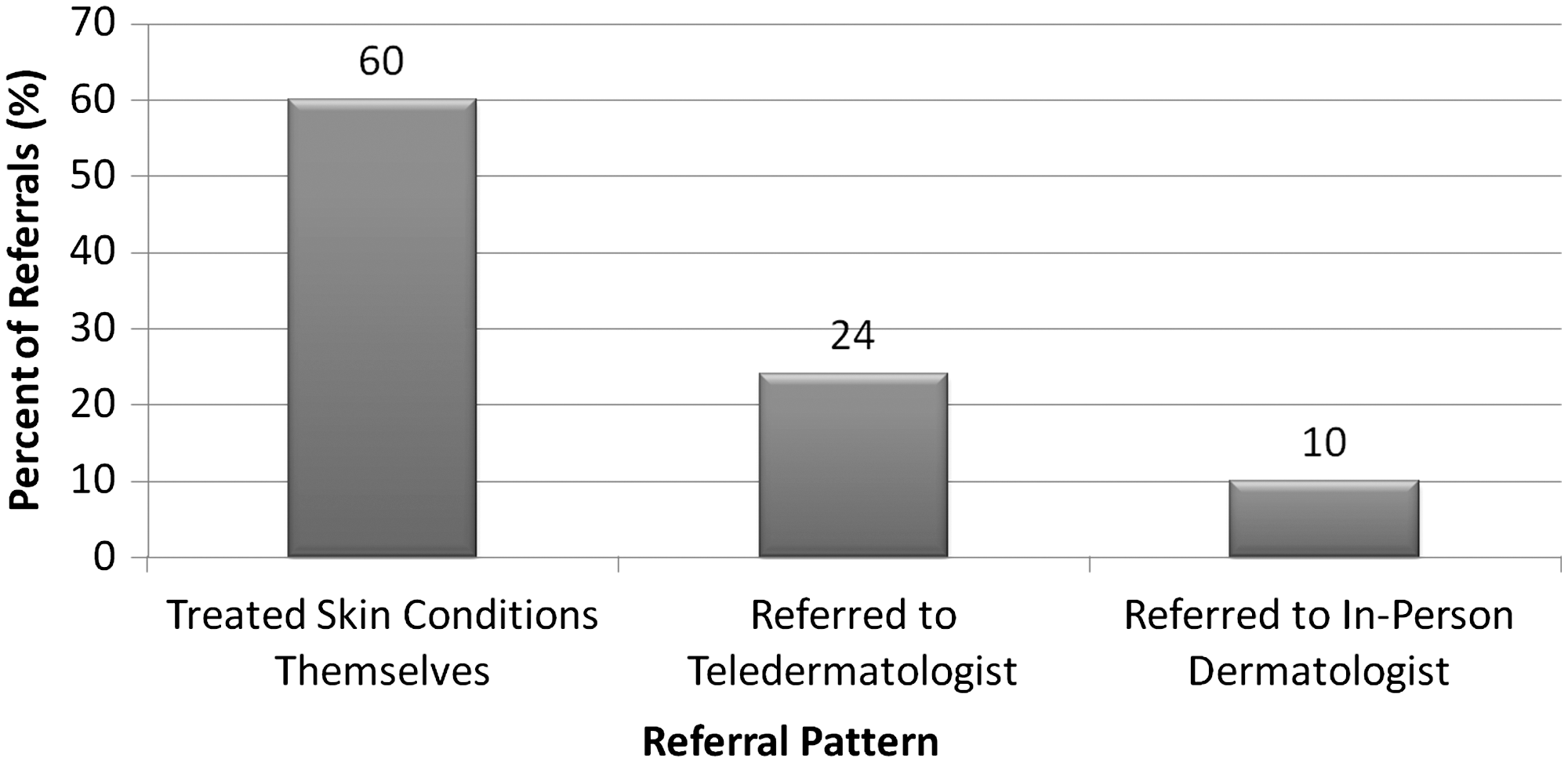
Primary care physician referral pattern for skin diseases.
We also sought to understand factors that influence PCPs to use teledermatology compared with treating the skin diseases themselves (Fig. 3). In general, patients with Medi-Cal or uninsured patients are preferentially referred to teledermatology.
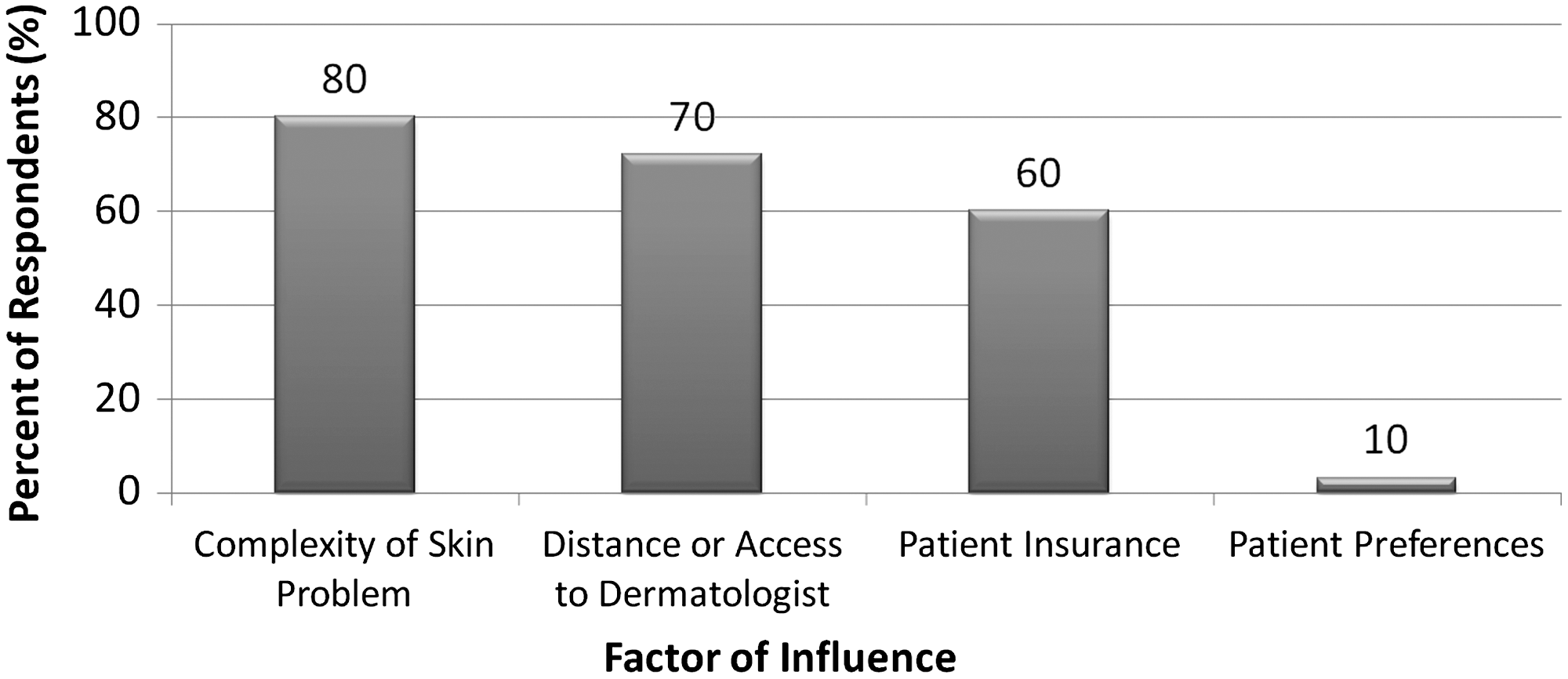
Factors influencing the decision to refer to teledermatology.
Referral site operation
When we asked the primary care physicians their expected staffing requirement for teledermatology, 40% of the PCPs reported that they have no specific staffing requirement. Among the rest of the PCPs who were interviewed, they reported using healthcare professionals of all levels, including physicians, mid-level providers, medical assistants, or nonmedical personnel, to assist with different aspects of the teledermatology operation. Typically there are no dedicated schedules for S&F teledermatology, and patients get their images taken at the time of their primary care visit. When queried about the added responsibility of communicating teledermatologists' recommendations with patients, 90% of PCPs welcomed this added responsibility.
Follow-up of patients needing in-person dermatology visits
When either the PCP or the teledermatologist deemed that an in-person visit with a dermatologist was necessary, 70% of the PCP reported that they referred patients to a local dermatologist, and 30% of the PCP reported that they referred the patients to see the dermatologists who performed the teledermatology encounter.
Education of PCPs
When we asked PCPs whether their understanding of dermatologic problems has improved because of the availability of teledermatology service, 100% of PCPs reported that their understanding has improved and increased. They also reported that the types of skin problems for which they make teledermatology referral have changed over time. Whereas PCPs referred moderately challenging but common skin diseases at the beginning of the referral period, the referral rate for common skin diseases declined over time as they learned how to manage them through teledermatology.
Value and Challenges of Providing Teledermatology to the Medi-Cal Population
When we asked the primary care physicians the value of S&F teledermatology for their Medi-Cal population, 100% reported that it is extremely valuable, and 100% reported that they would like to see more teledermatology service provided to their Medi-Cal patients. Furthermore, if more teledermatologists were available, 90% PCPs reported that they would refer more patients to teledermatologists.
The primary care physicians were asked to identify factors important to the success of a teledermatology operation. The PCPs reported the following two factors as being central to a successful teledermatology operation: timely access to dermatologists (60%) and collegial PCP–dermatologist relationships that allow for dialogue on patient matters (40%).
We also asked PCPs to identify the most challenging aspects of participating in teledermatology. The PCPs identified the following challenges: implementing dermatologists' recommendations (40%), disruptions in their work flow as a result of incorporating teledermatology (40%), and difficulties in photographing skin lesions (20%). Finally, the PCPs were asked which aspect(s) of teledermatology operation needed improvement. The PCPs reported improvement in workflow (30%), decrease in consultation cost (30%), faster turnaround time for consultations (20%), improvement in communication with the dermatologist (20%), and technological improvements (10%).
Discussion
Value, Operational Considerations, and Challenges of Referring to Teledermatology Services
The results of our survey demonstrate that 100% of surveyed PCPs find teledermatology extremely valuable. Our survey elucidated that the primary reason that PCPs participate in teledermatology referral is to open the doors of access to dermatology services for their patients. In addition to increasing access to specialty care, participating in teledermatology provides an educational opportunity for primary care physicians. Over time, as their depth of knowledge has increased, these PCPs who regularly participate in the teledermatology referral process have learned to manage common skin conditions themselves and have required fewer dermatological referrals. While improving healthcare access and providing educational opportunities for referring physicians, teledermatology may also help to reduce the healthcare cost to society as PCPs learn to manage challenging cases of common skin diseases and as persons who formerly could not have obtained dermatology care receive treatment during the earlier, more treatable stages of their skin diseases.
Although our survey demonstrates that the primary care physician considers teledermatology extremely valuable, he or she must also consider the practicalities of time management, staffing requirements, and office workflow that may be affected if teledermatology is incorporated into the physician's practice. In regard to time considerations, the surveyed physicians, all of whom regularly refer their patients for teledermatology services, spend only 4% of their time participating in teledermatology. Furthermore, 90% of those surveyed would refer additional patients to teledermatology if more teledermatologists were available, and 100% would like to see more teledermatology services available for their Medi-Cal population. Of the PCPs surveyed, 90% do not mind the additional time required to communicate the teledermatologist's recommendations to their patients.
In addition to time requirements, the PCPs must consider which healthcare staff members are necessary to successfully participate in teledermatology communications. According to our survey results, the type of healthcare professional needed to assist PCPs in teledermatology operations varied for 60% of the physicians surveyed. Alternatively, 40% of those PCPs surveyed reported that they have no specific staffing requirement. This diversity in human resource requirements suggests that teledermatology may be adapted and implemented in a variety of PCP office settings.
In addition to considering human resources, PCPs who desire to participate in teledermatology operations should contemplate how their practice workflow may be adjusted to smoothly incorporate the teledermatology referral process. First assessing the effectiveness of a variety of healthcare employees in assisting with teledermatology practice operations may enable the PCP to select the most effective staff member for the task and devise an efficient workflow.
In addition to their practice considerations, we asked the referring physicians to identify those (1) challenges, (2) factors critical to success, and (3) areas needing improvement associated with participating in teledermatology operations. From their responses, several themes emerged, including the need for improved workflow, communication, and timely access to dermatologist. Regarding their own practice, PCPs identified disruptions in workflow and implementation of the teledermatologist's recommendations as challenges associated with teledermatology. Additionally, open, collegial communication with teledermatologists and timely access to a dermatologist were two factors identified as crucial to a successful teledermatology operation.
The findings of this study need to be interpreted within the context of the study design. Selection bias could be present in this study by focusing on referring providers who regularly refer patients to teledermatology. However, because one aim of this study was to elucidate challenges during the work process, providers who frequently participate in teledermatology referrals were most likely to identify long-term barriers. Future studies can focus on surveying a greater number of referring providers with diverse teledermatology experience to identify different challenges associated with program initiation and sustainability.
Suggestions for Addressing Challenges of Referring to Teledermatology Services
Because PCPs who regularly refer to teledermatologists identified enhanced workflow, communication, and timely access to dermatologists as necessary improvements to teledermatology operations, we recommend adoption of the following policy or practice recommendations (Table 1).
Summary of Policy Recommendations and Practice Suggestions
Policy and practice recommendations to enhance communication and improve workflow
Although telehealth training is available through different mechanisms, many practitioners of telehealth, including both dermatologists and referring providers, do not receive standardized training and tend to take the approach of “learning on the job.” Haphazard training can create nonstandardized and nonstreamlined work processes and suboptimal teledermatology data quality. Therefore, encouraging newcomers to obtain structured telehealth training from the existing educational mechanisms will help ensure a high standard of telehealth care.
Both the teledermatologists and PCPs have emphasized the importance of technological improvement to achieve greater efficiency in clinical care. Most practitioners hope to see the creation of less cumbersome and efficient systems that are easy to learn and navigate. Additionally, these systems must be affordable to allow more practitioners to engage in telehealth. Efficient technological applications will improve practice workflow, open the lines of communication between PCPs and specialists, and reduce provider time requirements as improved applications allow practitioners to focus on caring for the patient rather than troubleshooting the application.
In addition to improved telehealth technologies, taking steps to ensure that workflow is streamlined to easily integrate telehealth is crucial to an optimal practice structure. Because many referral sites do not have dedicated teledermatology clinic or staff, when a patient presents with a skin condition that would benefit from use of telehealth, a PCP or another medical staff member stops his or her usual work process to locate teledermatology equipment, image the patient, and refer the patient to teledermatology. Sometimes, this is perceived as a “disruption” to the usual work process, and practitioners and their staff are reluctant to deviate from their usual workflow. Therefore, developing novel methods of integrating teledermatology seamlessly into the existing workflow is critical.
Policy and practice recommendations to improve timely access to dermatologists
The Medi-Cal requirement to document barriers to an in-person visit for coverage of telehealth services presents significant challenges and disincentives to providing telehealth services. The administrative burden associated with documentation of barrier to telehealth services sometimes exceeds efforts involved with actual care of the patient. The referring providers need to be able to select the most appropriate healthcare delivery for their patients, and the teledermatologists need an efficient system for providing that service and obtaining reimbursement. The administrative burden involved with teledermatology referral must be no greater than that involved with in-person dermatologist referrals. Therefore, we should eliminate the requirement to document barriers to an in-person visit for coverage of teledermatology services.
Another important incentive for PCPs to refer patients to teledermatology is the timely receipt of the detailed and specific dermatologist's recommendations. When the teledermatologist cannot produce timely responses, the PCPs are less incentivized to refer the patient to teledermatology and are more likely to either care for the skin disease themselves or refer the patient for an in-person evaluation. Furthermore, PCPs reported that general recommendations are usually not helpful; instead, they prefer to receive specific recommendations with detailed discussions of alternative treatments that are customized to their patients. Thus, we encourage teledermatologists to make timely and specific recommendations to referring providers.
Conclusions
Literature that describes the referring provider's perspective on teledermatology services for medically underserved patients is scarce. Without first understanding the PCP's viewpoint, attempting to improve current specialty telehealth operations may not prove efficacious. Furthermore, evaluating and addressing the referring provider's perspective are crucial in encouraging additional teledermatology participation and improving access for medically underserved patients. With strong reimbursement policies in place, evaluating the use of telehealth services in the Medi-Cal population is a worthy investigative starting point. One hundred percent of surveyed PCPs reported that their primary reason for participating in teledermatology operations is to increase access for their patients, and 90% reported that they would refer more patients to teledermatologists if more teledermatologists were available. Meanwhile, 100% of those surveyed reported that their understanding of dermatologic problems has improved because of the current availability of teledermatology service, and 100% rated the overall value of teledermatology as extremely valuable.
To enable future patients and PCPs to benefit from teledermatology operations, we sought to understand the current challenges of participating in teledermatology referrals from the PCP perspective. To address the areas concerning to referring PCPs, which include improved workflow, communication, and timely access to dermatologists, we recommend adoption of the aforementioned policy and practice recommendations. The incorporation of these recommendations into primary care and teledermatology operations will enhance the effectiveness of current teledermatology programs, will encourage additional PCPs to participate in the teledermatology referral process, and will ultimately improve healthcare access for the medically underserved.
Footnotes
Acknowledgments
We would like to acknowledge Dr. Jeffrey Benabio, Dr. Melvin Chiu, Dr. William J Coffey, Dr. Kelly Cordoro, Dr. Noah Craft, Dr. Eileen Crowley, Dr. Haines Ely, Dr. Ilona Frieden, Dr. Eric Fromer, Dr. Marc Goldyne, Dr. Michael Kolodney, Dr. Ivy Lee, Dr. Toby Maurer, Dr. Dennis Oh, Dr. Abel Torres, and Dr. David Wong for their participation in this project. We thank Dr. Marc Goldyne for his valuable insights and guidance regarding the design of this project. We thank Amber Harrison for her administrative support of this project.
Disclosure Statement
No competing financial interests exist.