
Abstract
Introduction
Chronic obstructive pulmonary disease (COPD) 1 is widespread, both nationally and internationally. Approximately 210 million people suffer from COPD worldwide, of which about 80 million suffer from moderate to severe COPD. In 2005, more than 3 million people died from COPD, equivalent to approximately 5% of all deaths globally, and the number of COPD deaths is predicted to increase in the coming years. 2 There is a need to manage COPD more effectively so as to reduce healthcare costs and enhance patients' quality of life (QoL).
Telehomecare is understood as care and treatment carried out between the patient's home and healthcare professionals, with the support of communication and information technology. 3 –5 Telehomecare has the potential to prevent or reduce admissions to the hospital or even to extend life. 6,7
Systematic reviews of the cost-effectiveness and impact of telehomecare show that telemonitoring can be both effective and cost-effective. 3,8 However, no definitive conclusions can be drawn from the existing literature, as it consists of small pilot studies of different methods of telehomecare. 3,8 –11
The present study conducted a cost-utility analysis (CUA) of the Danish TELEKAT (Telehomecare, Chronic Patients and the Integrated Healthcare System) project. The TELEKAT project tested and developed a preventive home monitoring concept across sectors for COPD patients. The concept of the TELEKAT project is to reduce admissions by enabling the COPD patients to conduct self-monitoring and maintain rehabilitation activities in their own home. COPD patients with severe and very severe COPD were included in the study. This article is one of several analyses based on the TELEKAT study. 12 –14
Subjects and Methods
Health Economic Evaluation
This economic evaluation followed international guidelines for the conduction of a CUA alongside a clinical randomized controlled trial. 15,16 The analysis was based on a health sector perspective.
All prices and unit costs are from 2010, calculated in Danish kroners and converted into euros using the exchange rate of EUR 100=DKK 750.
The Telekat Project
The TELEKAT project is a randomized controlled trial of 111 COPD patients who were block-randomized into a telerehabilitation group (60 patients) and a control group (51 patients). Randomization was performed by the Aalborg University Hospital (Aalborg, Denmark), general practitioners (GPs), and healthcare centers after written informed consent was obtained from the patients. After eligibility was confirmed and written informed consent was obtained, concealment was performed by a nurse, blinded for healthcare professionals, patients, and researchers. Three COPD patients subsequently dropped out of each group, resulting in a final participation of 57 COPD patients in the telerehabilitation group and 48 COPD patients in the control group. The trial was carried out in Aalborg and followed the guidelines issued by the local Ethics Committee. The study was performed according to the Declaration of Helsinki, and the project was registered with the Danish Data Protection Agency. The COPD patients utilized the telehomecare technology for 4 months with a follow-up period of 6 months, during which prospective data were collected.
Each COPD patient in the telerehabilitation group received a telehealth monitor (model 3370/71; RTX Healthcare) installed in his or her home so that the individual could conduct measurements of lung function, weight, oxygen level, blood pressure, and pulse and thereby monitor the course of the disease. The COPD patients used the telehealth monitor for 4 months, and a doctor prescribed how often the patient had to measure values during a week. During the installation of the telehomecare equipment, the patient was instructed how to take clinical measurements and how to use a step counter and advised in general on how to exercise.
Through wireless technology, the telehealth monitor can collect and transmit data via a secure transmission line. The data are sent to a Web-based portal or to the patient's electronic healthcare record. Healthcare professionals from both primary and secondary sectors, such as GPs, district nurses, hospital nurses, and doctors at the healthcare center or hospital, assessed the patient's data, monitored the patient's disease and training inputs, and offered advice. The patients and relatives could also view their own data on the Web portal. The structure of the telerehabilitation program is illustrated in Figure 1.
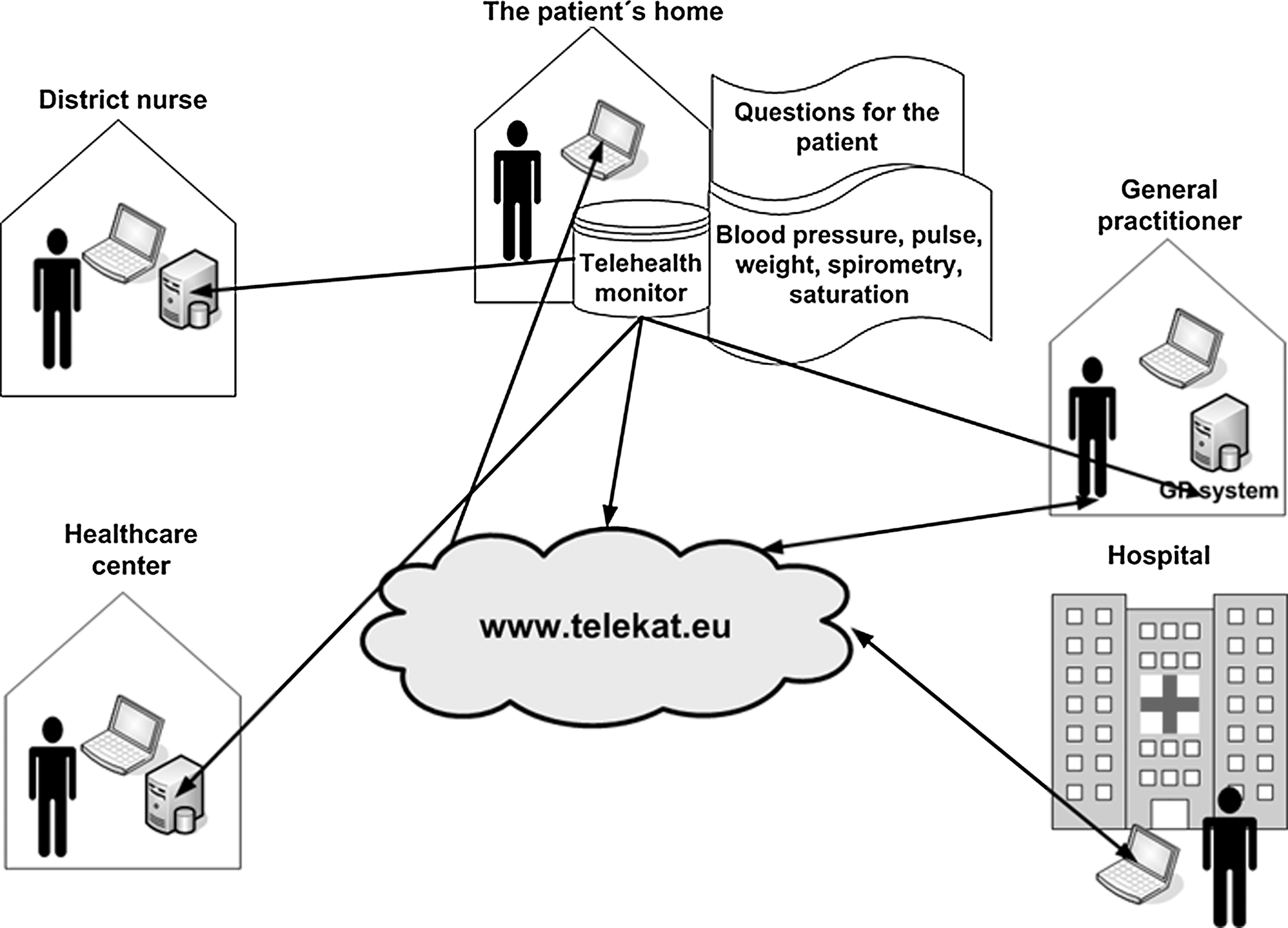
The structure of the telerehabilitation program.
Once a month, a telerehabilitation team consisting of healthcare professionals from primary and secondary sectors would meet online to discuss and coordinate rehabilitation measures for each COPD patient.
The control group received instructions on performing home exercise, and these patients were then made responsible for performing the activities by themselves. Participants from both the telerehabilitation and the control groups might have participated in other rehabilitation activities, such as networking groups, during their participation in the 4-month trial period of the TELEKAT project. The control group did not have as close contact with the healthcare professional as did the telerehabilitation group. Both groups were informed that if urgent treatment was needed, they should contact either their GP or an emergency doctor. Aalborg University was responsible for the logistics of the TELEKAT project (hotline for those with technical problems and delivery, installation, and removal of the equipment).
After the COPD patients were enrolled in the study, a doctor entered baseline information on clinical data, as shown in Table 1.
Characteristics and Interquartile Range Baseline Variables for the Telerehabilitation Group and the Control Group
MRC, Medical Research Council.
Outcome Measurement
The Short Form-36 (SF-36) 17 was used at baseline and at 10 months. Brazier's algorithm 18 was used to convert SF-36 scores into SF-6D scores. The difference between the SF-6D QoL scores at baseline and 10 months was used to estimate the quality-adjusted life years (QALY) gain in each group over a period of 10 months.
Cost Measurement
Data for resource usage and unit costs were collected prospectively during the randomized controlled trial. According to international guidelines for health economic evaluation, only marginal costs have been collected (i.e., the costs that differ between the two groups).
16,19
Marginal costs include: • Costs related to telehomecare equipment: training of healthcare professionals, logistics, and the time used by healthcare professionals • Costs related to hospital admissions, ambulatory contacts, GP contacts, emergency physician contacts, other primary services, and medicine consumption
The costs related to training of healthcare professionals include time spent on training and the healthcare professionals' various hourly salary rates. The training of the healthcare professionals consisted of instruction in their use of the equipment so that they can assist the COPD patients.
It is assumed that the training of the various healthcare professionals is useful for 5 years, meaning that it is estimated that no further training of healthcare professionals is needed within this 5-year period. To estimate annual costs of training and per-patient cost, the annuitization method is applied using a discount rate of 3%.
The costs of the telehomecare equipment are based on current prices of the equipment at the time when the TELEKAT project began (2008) excluding VAT. At the completion of the study, the equipment was discarded with no scrap value.
The logistical costs cover time spent on installing and calibrating the equipment in the patient's home; these costs also include costs of salary for the technical personnel and gasoline.
The opportunity costs of the healthcare professionals are estimated according to the effective time they have spent working on the TELEKAT project multiplied by their individual hourly salaries.
The primary sector includes contacts with the GP, emergency physician, dentist, physiotherapist, ophthalmologist, and other medical specialists. Other primary services cover all contacts to the primary sector, excluding contacts with the GP and emergency physician. In the Danish Civil Registration System, all Danish citizens and residents are assigned a unique civil registration number that is used in all health databases. This allows for unambiguous record linkage between databases. 20
The costs related to the presented outcomes (e.g., hospital admissions, ambulatory visits, GP visits, etc.) are drawn from the National Patient Register that records every visit made by a citizen in the Danish healthcare system. Each healthcare service is ascribed a certain standardized rate in Denmark, such that costs related to the presented outcomes are based on the number of visits recorded in the Danish National Patient Register multiplied by the ascribed standardized rate.
Incremental Cost-Effectiveness Ratio
The incremental cost-effectiveness ratio (ICER) is the result of a CUA. The mean ICER is calculated according to the formula:
The incremental QALY of the ICER is calculated according to the formula:
Analysis
The data analysis is based on the principle of intention to treat. A complete case analysis was performed with a telerehabilitation group (35 patients) and a control group (34 patients). The results are presented as mean cost and QALYs gained from telerehabilitation and control, with±95% confidence intervals (CI), and ICER at 10 months post-randomization. The cost-effectiveness acceptability curve shows the probability that the telerehabilitation program is cost-effective given varying threshold values of willingness to pay for a QALY.
Data were analyzed with Stata version 9.1 software. The cost-effectiveness acceptability curve and CI around differences in outcomes and cost are generated using nonparametric bootstrapping.
Results
The baseline average QoL scores at the start of the study were estimated to be 0.589 for the telerehabilitation group and 0.59 for the control group. Hence, there was no need for statistical adjustment for differences in baseline QoL scores. After a 10-month period, the incremental QALY was calculated (Table 2).
Mean Costs and Incremental Quality-Adjusted Life Years in the Telerehabilitation Group and the Control Group
All costs are given in euros.
GP, general practitioner; QALY, quality-adjusted life years.
Cost-Utility
The mean ICER, located in the southeast quadrant, shows that telerehabilitation is less costly and more effective than the rehabilitation given to the control group.
Figure 2 shows the probability that the telerehabilitation program is more cost-effective than the conventional rehabilitation program.

The cost-effectiveness acceptability curve (CEAC) for telerehabilitation compared with conventional rehabilitation.
Discussion
The aim of the present study was to conduct a CUA of the Danish TELEKAT project. The results of the CUA indicate that the telerehabilitation program is more cost-effective than the conventional rehabilitation program. The telerehabilitation program produces more value for money and generates savings on healthcare budgets.
There remain limitations to our study. The baseline clinical characteristics of the groups, as shown in Table 1, indicate that the telerehabilitation and control groups are comparable on the key variables. However, we did not control for differences in socioeconomic characteristics. This variable may be of major importance, as the clinical effects from telehomecare depend largely on the participants' attitudes and capacities to change behavior or alter their lifestyle. 14
The results of our study may be difficult to reproduce in an actual implementing situation or a large-scale test of the telerehabiliation program. The TELEKAT project is a small-sized research-and-innovation project, conducted by highly motivated researchers, healthcare professionals, and patients encouraged to participate in patient-driven innovation.
The prices for the equipment used in the TELEKAT project are higher than today's purchase prices, and, in addition, there may be large discounts on equipment when used in a large-scale implementation.
Furthermore, the CUA conducted in this study does not include costs outside the health sector, such as homecare and indirect costs. The CUA carried out here shows that telerehabilitation is cost-effective at the health sector level. However, further research is needed because some costs are not accounted for in this economic evaluation; for example, cost-shifting might be present. As mentioned earlier in this article, participants from both the telerehabilitation and the control groups might have participated in other rehabilitation activities, such as networking groups, during their participation in the 4-month trial period of the TELEKAT project; this might be a potential confounder in that these additional rehabilitation activities were not accounted for when the patients were selected for the two groups. Additional rehabilitation activities may influence the results of the TELEKAT project, as previous studies have shown rehabilitation to have a positive effect on QoL. 21 The COPD patients included in the TELEKAT project have the disease at an advanced stage, a factor associated with a relatively high level of medicine consumption. Therefore, medicine consumption was not expected to decrease, as advanced-stage COPD requires a high level of medication.
It has not been possible to identify any other studies of telehomecare that have been carried out within a similar interdisciplinary setting, including representatives from the healthcare center, GP, hospital, and district nurses and where the healthcare professionals have been able to share data and meet virtually. Furthermore, the enhanced QoL in the telerehabilitation group may stem from improved patient monitoring and coordination between healthcare professionals and/or the efforts to improve rehabilitation and patient education that were also part of the intervention. Hence, the lack of comparable telehomecare projects, small sample sizes, and different methodologies make it difficult to compare this study with other telehomecare studies. Further research is needed in order to fully establish the cost-effective potential of telerehabilitation.
Conclusions
The telerehabilitation program appears to be more cost-effective than the conventional rehabilitation program for COPD patients. Further studies of cost-effectiveness with a focus on large-scale studies are needed.
Footnotes
Acknowledgments
We wish to thank the COPD patients and their relatives for participating in the project, as well as clinical and industrial partners (for details, see
Disclosure Statement
No competing financial interests exist.