
Abstract
Introduction
Telehealthcare is the provision of healthcare service to promote service delivery outside the medical institute and that acts as an extension of outpatient settings. It combines information communication technology and commercialized biometric sensor devices, which address disease management at a distance and facilitate longitudinal health status monitoring. 1 –4 The service has become more and more popular because of several reasons, including using existing healthcare resources more effectively, reducing hospitalization without increasing mortality, and increasing satisfaction compared with daycare centers or nursing homes. 5 –11 The effectiveness of telehealthcare service has been indicated, 12 –16 and there have been many related works in the past decades, such as hypertension, diabetes, heart disease after surgery, or pediatric care. 8,10,12,17 –24 Some of the research has focused on individual diseases, 25 –31 and some has supported generalized chronic disease care. 5,32
Information technology (IT) is increasingly used in healthcare practice, and IT infrastructure appears to be essential while providing telehealthcare service. There are many designs of telehealthcare systems, 5,25 –33 mostly adopting Web-based architecture 5,25 –27,29,30,33 to ensure portability. Some have adopted medical informatics standards 5,27,29 to retain interoperability, and some have exchanged data with existed information systems through an nonstandardized approach. 31,33 Many works have cooperated with off-the-shelf biometric sensors, 5,25,30 –33 with the integration of biometric data being manually inputted, 26,28,30 transmitted through telephone lines, 25,32,33 or transmitted through Bluetooth® (Bluetooth SIG) or a Recommended Standard 232 port to a middleware device, such as a mobile phone or personal computer, 5,27,29 to gain access to the Internet and then uploaded to the server. Some of the studies have investigated the sensors themselves. 27,29
Several insufficiencies have been identified from previous studies, 5,8,33 –38 such as lack of integration with existing systems, the need to accommodate diverse biometric sensors and multiple brands, and inability to access diverse networks because different houses have varied facilities, which presents a challenge to the promotion of telehealthcare. The need for further study on the overall deployment and integration of a telehealthcare system has been pointed out. 12,33,39 To sum up, telehealthcare information systems (THISs) are required to strengthen the delivery of services, and several elements are considered important, including (1) data integration from existing information systems and medical informatics standards adoption, (2) data integration of diverse biometric sensors and multiple brands, and (3) provision of various data transmission networks to support patients' house networks despite differences in the facilities.
This research designs an IT framework for strengthening telehealthcare delivery and will be further evaluated with a pilot study program at the National Taiwan University (NTUH), Taipei, Taiwan, which consists of two telehealthcare programs, with and without the adoption of the framework. The design of the framework and the evaluated case study are described in the Materials and Methods section, and the result from the case study and some of the outcomes of patients are also demonstrated.
Materials and Methods
This study proposes a technology framework to achieve the goal of strengthening telehealthcare delivery. The identified criteria consist of (1) data integration from existing information systems and medical informatics standards adoption, (2) data integration of diverse biometric sensors and multiple brands, and (3) provision of various data transmission networks to support patients' house networks despite differences in the facilities. This research further evaluates the proposed framework with a case study of two telehealthcare programs, for general chronic diseases and heart failure, with and without the adoption of the framework, respectively. The proposed framework consists of two parts, namely, a system architecture design and a network transmission design.
ARCHITECTURE DESIGN
The architecture design consists of the inner structure of the THIS, which adopts the service-oriented architecture, Web-based approach to facilitate scalability and portability. The system is segmented into four layers, including the user interface (UI), data processing, message exchange engine, and data repository, illustrated in Figure 1. Figure 2 demonstrates the system snapshot.
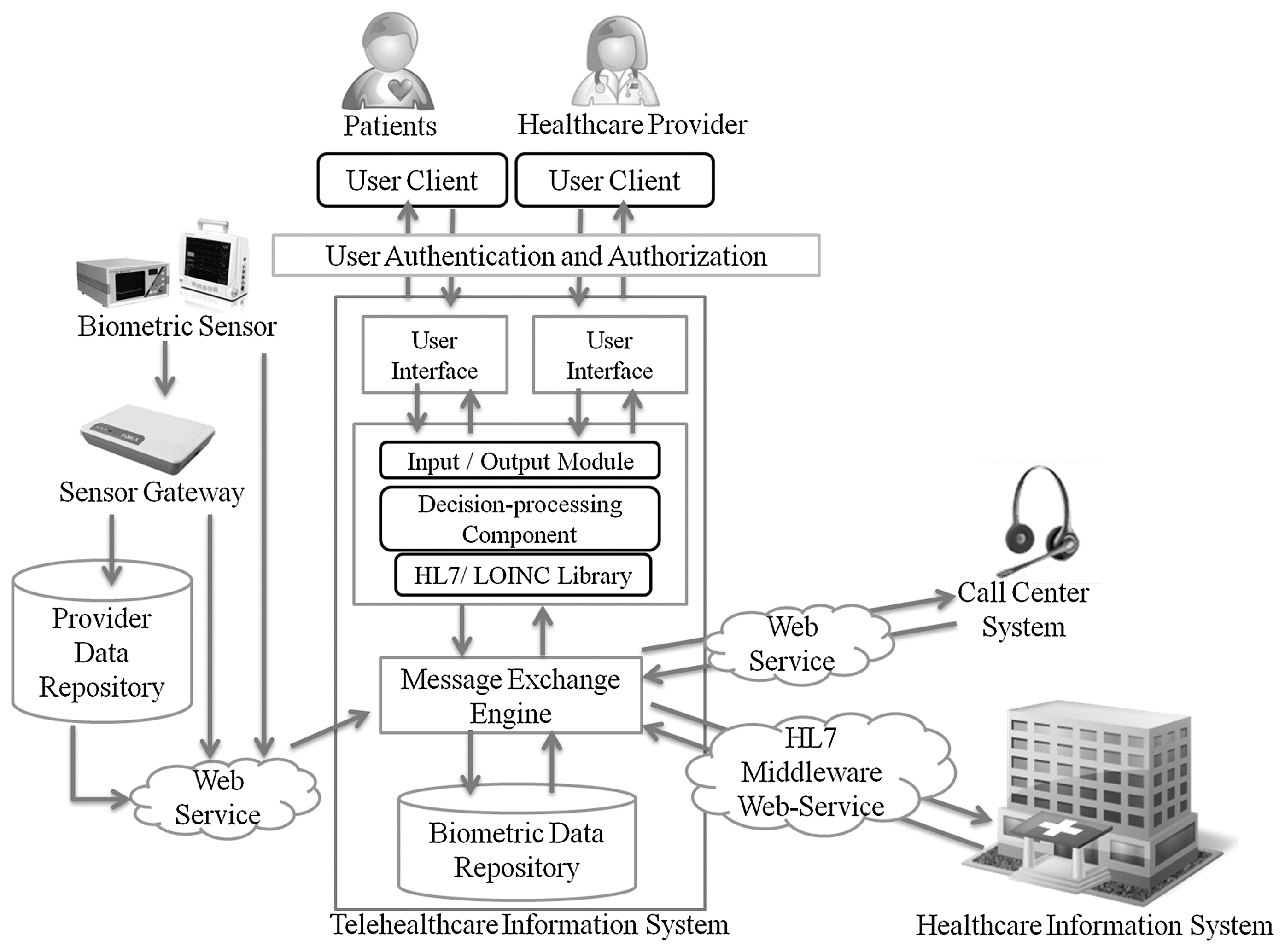
Architecture design of the telehealthcare information system.

Snapshot of the telehealthcare information system.
The UI layer
This layer includes the user-client, user authentication, and authorization. The THIS is only accessible by using a unique account and password. It authenticates the users through accounts and passwords, and the information retrieval of the user-client is based on user identifications. The UI demonstrates the contents and the operation of the system, such as patient information, patient lists, abnormal events, graphic presentation of the vital signs data, reports, messages delivery, evaluation and assessment records, making phone calls, and photo uploads.
The data processing layer
This layer consists of the data input/output component, decision-processing component, and HL7/LOINC library. The input component includes the integrated resources, manual data input, and open access resources. Integrated resources consist of biometric sensor data, medical records, call center system, etc. The manual data input includes the assessment evaluation and interviews of patients. The open access resources include services such as Google Weather API, in order to access everyday climates and remind the patient of avoiding overcontraction of blood vessels and controlling the condition of hypertension. The system illustrates the temperatures of Taipei, Taichung, and Kaohsiung, which represent the locations of northern, central, and southern part of Taiwan, respectively, for serving patients with different locations. The output component includes short message service text messaging and the Skype phone call service to notify of abnormal events through mobile messaging and to facilitate automatic dial-by-click phone calls.
The decision-processing component is a rule-based engine that executes the rules and personalized data thresholds. The rule-based engine supports the condition monitoring and operates routinely as a batch process, such as the personalized abnormal event screening, climate change reminding, medication adherence enhancing, and retention in care plan monitoring. THIS schedules the patients and generates patient lists for the case managers to enhance medication adherence, to monitor retention in the care plan, and to enable efficient patient management. The HL7/LOINC library acts as a reference to ensure the data format being standardized.
The message exchange engine
Standardization is an important component to ensure the interoperability of the system. The message exchange engine receives the data through the middleware Web service, refers to the HL7/LOINC library, transforms the data into standardized format, and integrates them into the storage repository.
The biometric data repository
The biometric data repository adopts standardized HL7 format and LOINC terminology, receives standardized messages from the message exchange engine, and stores them in the repository.
Network Transmission Design
The network transmission design mainly deals with the data exchange from outer data resources and the coordination of multiple data transmission networks, illustrated in Figure 3.
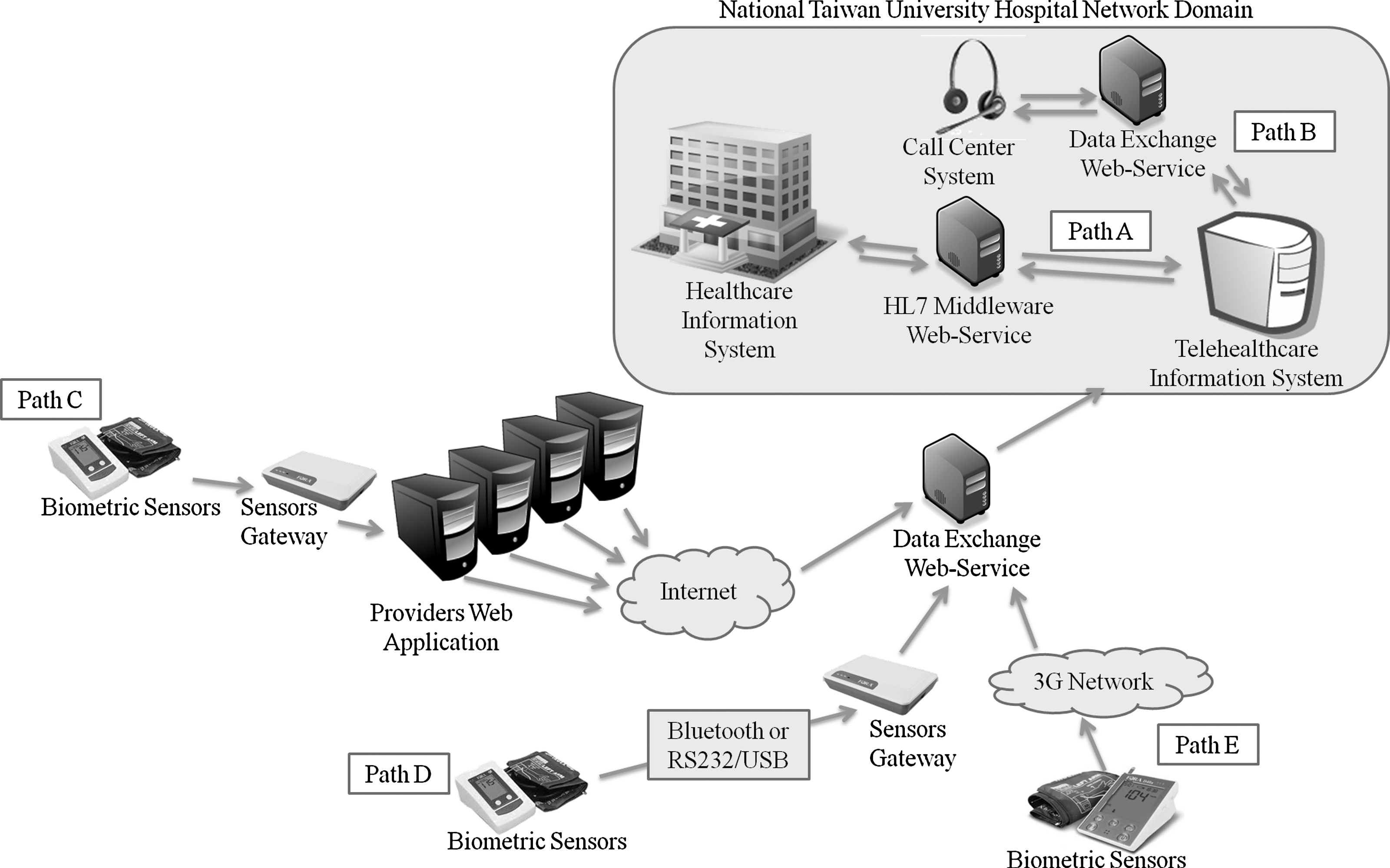
Data transmission network design: Path A, the telehealthcare information system and the healthcare information system exchange data through an HL7 middleware Web service; Path B, the integration of the call center system through a data exchange Web service; Path C, the integration of four Web applications of biometric sensor providers, which gather biometric data through a data exchange Web service; Path D, data retrieval straight from the data transmission gateway to the data exchange Web service, without passing through the providers' Web application; and Path E, the device is inherited with the ability to transmit data through the third-generation mobile telecommunications (3G) network without the gateway.
The two main data exchange resources are the data in the hospital and the biometric data from the commercialized devices. To integrate data from the hospital, THIS is located inside the NTUH network domain. Data exchange between THIS and the healthcare information system (HIS) is through a HL7 middleware Web service, and the documentation is in XML form (Path A). Data exchange requires an authentication in advance. THIS asks for data of a specific patient, and HIS retrieves them. HIS requests notification of whether the patient is referred to the program and for detailed information if necessary. Essential information for disease management is collected from HIS, such as the past clinic visit records, diagnosis, allergy histories, and medication lists. The system also integrates information from the call center system (Path B) through a data exchange Web service.
This study coordinates three data transmission networks from four biometric sensor providers. Many biometric sensors have inherited data transmission networks, such as public switched telephone networks, Internet, and third-generation mobile telecommunications (3G). Table 1 summarizes the product characters from the four biometric sensor providers in Taiwan. It could be observed that most of the providers offer Web applications, to collect the data from their own products and to view the data. Patients measure biometric data at home, which are transmitted through a data transmission gateway to the Web application of the providers. The Web application then transmits the data through the data exchange Web service and integrates the data into the THIS data repository (Path C).
Product Characters of the Four Biometric Sensor Providers
3G, third-generation mobile telecommunications; DTMF, dual-tone multifrequency signaling; PSTN, public switched telephone network.
With concerns of data scattered in diverse repositories causing the violation of patient privacy, this study favors integration of the data without going through the application of the providers. Data retrieval is further addressed from the data transmission gateway (Path D) or from the sensor itself (Path E). Data are transmitted through the Internet or 3G networks. The transmission network can be chosen based on the patient's needs. Not all the applications are able to modify or to open the data transmission port as required. The adopted solution is based on the character of the product.
Evaluation: A Case Study Of The Ntuh
This research evaluates the proposed IT framework by a case study of two telehealthcare programs, for general chronic diseases and heart failure, with and without the adoption of the framework, respectively. The program initially started in September 2009. Patients from outpatient settings or community care were considered. The service flow is demonstrated in Figure 4.
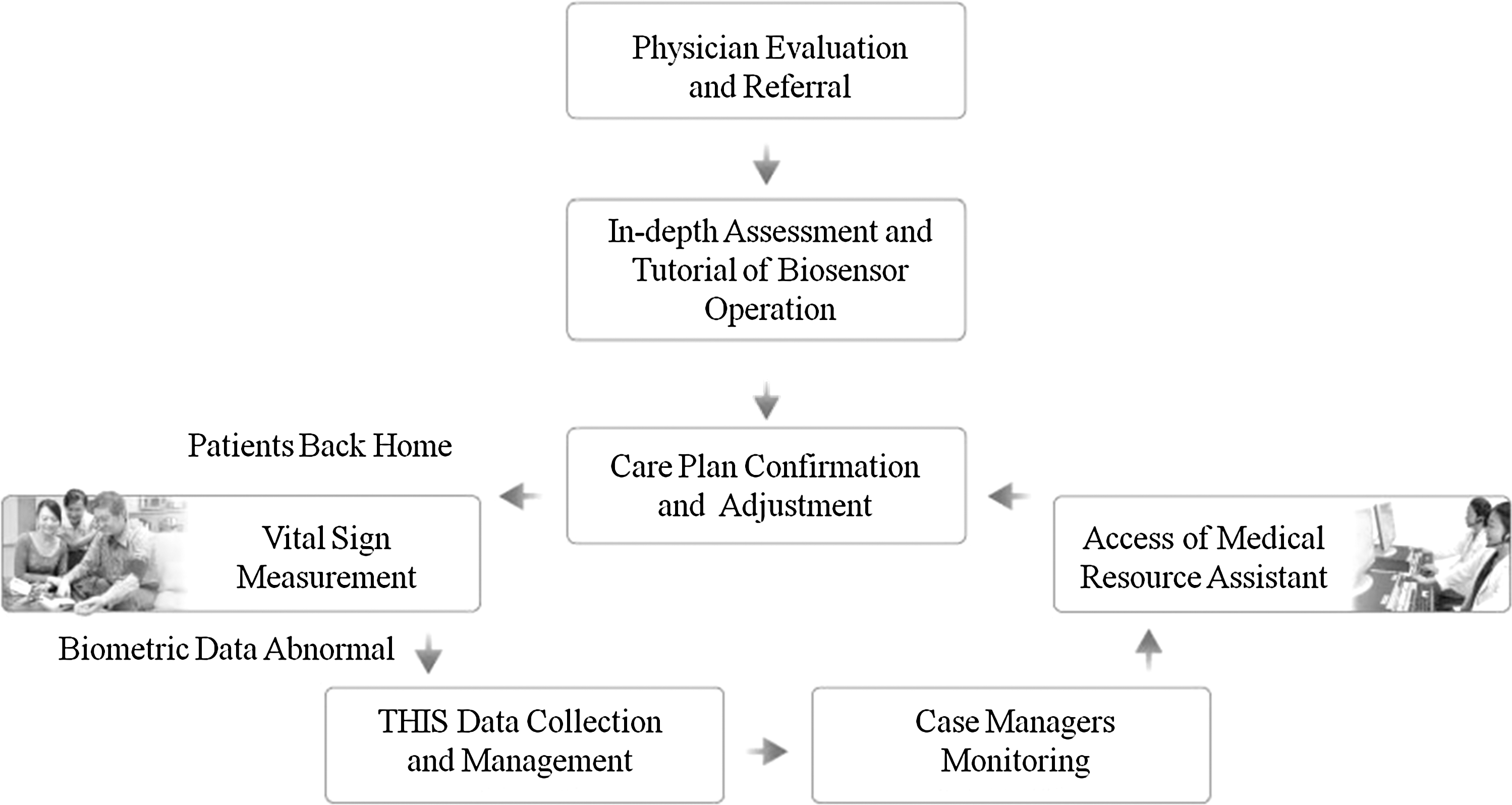
Telehealthcare service flow. THIS, telehealthcare information system.
During the clinical visit, the patients were evaluated by the physicians as to whether they would join the program or whether coming back for another routine appointment was sufficient. After patients were referred to the telehealthcare program, case managers would assist the patient in going through an in-depth assessment evaluation, provide introductions of the telehealthcare program, and tutor on the operation of the biosensor. The equipped sensors were determined based on the patient's condition. According to the in-depth assessment, the care plan of the individual was discussed and confirmed with the patient.
Sensors allow individuals to collect vital signs at home and to upload the data automatically while the Internet connection is available. As THIS collected the data, case managers were able to monitor patient status and provided further assistance or informed other staff if necessary.
As a pilot study, the program initially enrolled patients with heart failure. It started without a properly designed IT framework so that case managers had to access four types of data resources in order to gather the patient information needed, shown in Figure 5. The resources included the Web application of the provider, the HIS, an isolated client/server-based disease management information system, and other assessment documentations. The Web application was to access the biometric data the patients had uploaded. HIS was to retrieve information such as history, treatment, and medication because it was designed for general use in clinic practice, allowing the retrieval of data for a single patient at a time. Case managers had to query each patient individually. The disease management information system was provided by another IT provider by a prior project to record patient care information, but the data required manual inputting. Other assessment documentation includes the hand script not yet included in the systems, such as interviews and assessment hand script forms.
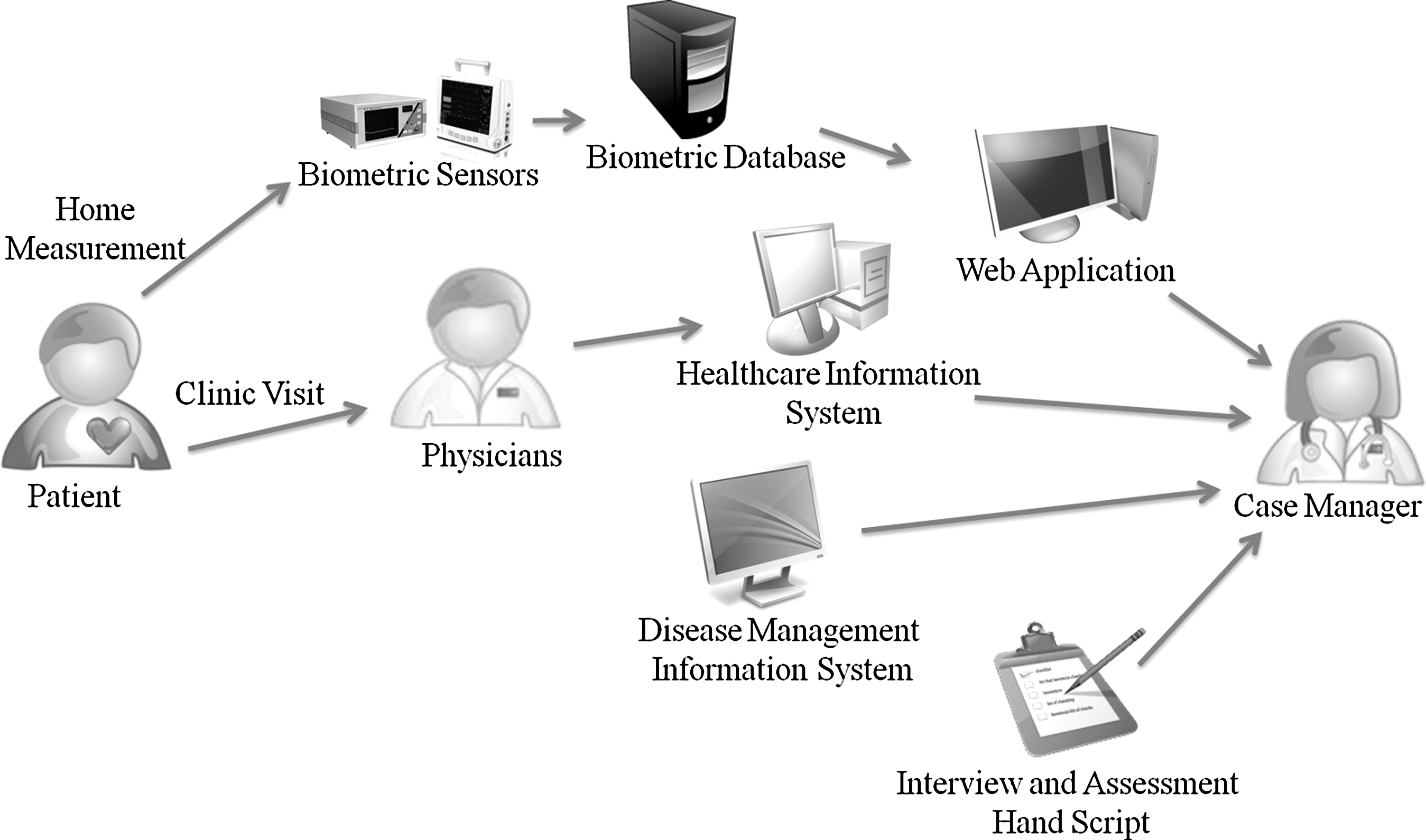
Four data resources to operate the telehealthcare service.
In order to take care of the patients, case managers had to access four different information resources, which consisted of ID/password login for three information systems, individual patient queries in each of the three systems, and manually collecting the information and integrating it into an Excel (Microsoft)-based patient data list in a desirable form.
The required patient information was scattered and required extra work to reach. Case managers were overwhelmed with data management as the number of the patients grew. This became a limitation toward the promotion of the service.
The NTUH telehealthcare program extended the service to hypertension and chronic diseases that, meanwhile, adopted the technology framework proposed. The extended service began from October 2010 for patients diagnosed with diabetes or hypertension or those who were willing to participate in health improvement voluntarily, who were referred to the program.
Results
The framework not only strengthens the delivery of care, but also facilitates further evaluation of the service performed. Table 2 compares the enrollment of the two programs, in which the number of heart failure patients is unstable and hard to trace, whereas the number of chronic disease patient enrollments steadily increases, and further insight of the program is more accessible.
Patient Enrollments of the Two Programs
For the chronic disease program, the average data upload frequency per patient per month went from 0.8 to 13.7 times during the period (Table 3). Status for 52% of the patients became stable, and the status of 44% of the patients approached the preset goals after entering the program. For example, the blood pressure of Patient A (Fig. 6) became more stable compared with the previous month. For Patient B (Fig. 7), the variance of the blood pressure decreased, became stable, and gently dropped into the preferable range of the preset goals within 1 month.
Frequency of Biometric Sensor Uploads of the Chronic Disease Program
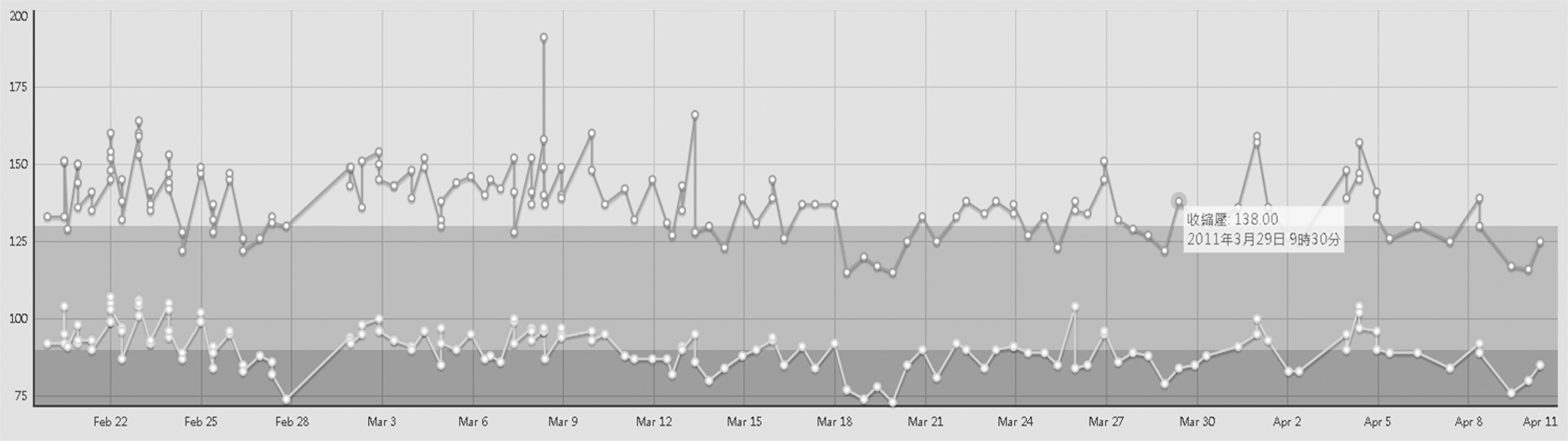
Daily blood pressure trend of Patient
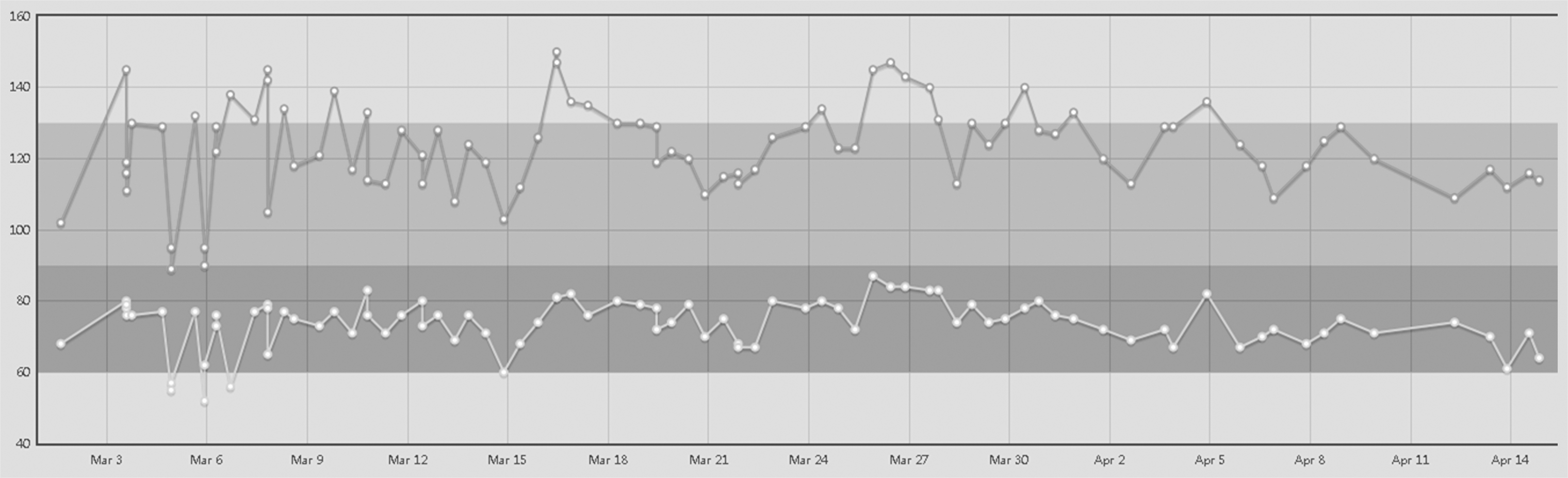
Daily blood pressure trend of Patient
In Figures 6 and 7, the upper line represents the systolic blood pressure, the lower line represents the diastolic blood pressure, and the background color illustrates the preset goals indicated when the patient was referred to the program. The upper background field defines the setting range for systolic blood pressure, and the lower background field defines the setting range for diastolic blood pressure. Once the arrow moves to the line, the THIS shows the detailed information of the data, such as the actual value, data capture date, and time.
As the telehealthcare program was underway, there were comments and feedback from the patients. The main influences of the service on patient self-awareness could be generally summarized as below. Patients expressed positive encouragement, which enhanced better self-management even after they left the program.
1. Consistent monitoring enables early findings: During the participation in the program, the consistent monitoring of blood pressure revealed patient lifestyle. Through daily monitoring, it became easier to find potential risk factors and the misinterpreted concepts in everyday life. Consistent monitoring enabled early findings, which facilitated preventive care and early intervention if necessary.
2. Better understanding of self-condition: Through longitudinal monitoring, daily blood pressure trends are illustrated. It became easier to trace a condition, which resulted in better self-understanding and self-awareness and enhanced self-management, education, and lifestyle adjustment.
3. Enhancing trust and confidence in self-improvement: With the encouragement from the case managers, patients gained more confidence in self-improvement and were willing to engage more in lifestyle changing.
Discussion
While the world is trying to provide telehealthcare service and correct maldistributed healthcare resources, the key to establish an infrastructure is to facilitate the service across regions and without boundaries. 11 The IT infrastructure is an essential part of telehealthcare delivery. A properly designed framework is able to enhance the delivery of the service. This study proposes an IT framework to strengthen the delivery of the services, and several elements have been considered important, such as the data integration and medical informatics standards adoption, the integration of diverse biometric sensors and multiple brands, and the provision of various data transmission networks.
INTEROPERABILITY AND DATA INTEGRATION
An isolated system might result in poor data integration, duplication of development resources, and lack of expansion for future evolvement. The service of telehealthcare could not be isolated from the existing healthcare delivery systems. Integrating with existing information systems and adopting medical informatics standards are the ways to connect the service to the current healthcare delivery system. In this study, the proposed framework segments THIS into four layers. The data are integrated through Web services. The message exchange engine receives the data and refers them to the HL7/LOINC library, then transforms the data into standardized format, and stores them into the repository. The design enables the data integration between standardized and nonstandardized information systems and considers the interoperability between systems. Based on the proposed system, case managers are able to manage patient status based on a single interface, the enrollment of patients steadily increases, and further insight of the program is more accessible.
Integration Of Diverse Biometric Sensors And Multiple Brands
The integration of the device-supported approach is a crucial step to make the service more accessible and more effective for telehealthcare. A wide range of commercialized biometric sensors and detectors are available nowadays. As the telehealthcare services are heading toward serving diverse illnesses, multiple indicating devices are essential. High acceptance will be achieved if the technologies are able to integrate the device the patient already knows. THISs are required to accommodate diverse biometric sensors and multiple brands in order to facilitate and promote the service. 36 With the multiple layer design, the framework is able to integrate the data of various biometric device providers, in a standardized or nonstandardized approach. The design enhances patient participation and gains acceptance as it integrates the device with which they are familiar. The outcomes of patients indicate positive improvements, and the self-awareness influences of patients show positive attitudes toward the service.
Provision Of Various Data Transmission Networks
Another way of enhancing participation of patients is to enhance the availability of the service. As the network infrastructure is not essential to every apartment, houses without network infrastructure may become a barrier toward the engagement of the program. The technology is required to provide availability according to different facilities. The proposed system adopted service-oriented architecture and Web-based architecture to ensure the portability and eliminate the limitation to specific operation platforms or devices. It is designed to integrate diverse data transmission networks to fulfill different considerations, such as the apartment differentiation, the preference of the patient, and the diversity of the product. The steady increases of data upload frequency of patients indicate the accumulation of patient acceptance and participation, as they become more familiar with the service and realize the benefit it could bring. Patients are willing to engage in it more and to become more active.
Conclusions
The findings of this study add up to the construction of a sophisticated information system to support telehealthcare. Implementing the proposed framework further assists the functionality of the service and enhances the availability of the service and patient acceptances. The framework of this study has been transferred to Pingtung Christian Hospital, showing that it is not limited to specific institutions, and the subsequent effect requires further observation. Further efforts are still required to realize telehealthcare in daily practice, but the benefits it can bring are promising, and it potentially leads to the reform of current healthcare systems.
Footnotes
Acknowledgments
The initial concept of this article has been accepted and published as “An Infrastructure to Enabling Integration of Personal Telehealthcare into Taiwan National Health Insurance” in the First AMA-IEEE Medical Technology Conference on Individualized Healthcare, 2010. 40 The project has undergone review by the Institutional Review Board (protocol number 201010055R). The authors would like to thank the National Science Council of Taiwan for funding the program (grant NSC 99-2219-E-002-023). We express our gratitude for the cooperation of the Department of Family Medicine, Information Systems Office, and the Department of Nursing of NTUH and the participation of the case managers.
Disclosure Statement
No competing financial interests exist.