
Abstract
Introduction
Healthcare consistently strives to achieve excellence in patient care while being cost-efficient and improving patient satisfaction. To address workflow or process issues, hospitals and health systems have turned to strategies such as Plan Do Study Act and Lean Six Sigma to redesign workflow and evaluate programs.
1
The Joint Commission and hospitals use tracer methodology to evaluate the entire patient experience and patient care (
Technology provides a layer of oversight and support to the bedside staff that enables improved patient care. 2 Remote monitoring provided by a tele-intensive care unit (ICU) program (the Philips eICU® Program) is an example of such supportive technology. The tele-ICU program is typically staffed with an intensivist (8–24 h/day) and an expert critical care nurse or nurses 24 h/day following the traditional medical model of care (Fig. 1). Working together to ensure best practice initiative adherence and collaborating to make the right patient care decisions, the tele-ICU care team facilitates improved outcomes. 3 The remote team monitors and cares for hundreds of patients using software alerts to track patients and intervene before complications occur. Embedded in the eCareManager software from the Philips eICU Program is the Acute Physiology and Chronic Health Evaluation (APACHE®) severity outcome and length of stay (LOS) methodology (Cerner Corporation). Sites that have performed pre- and post-implementation studies have demonstrated impressive reductions in severity-adjusted mortality and LOS. These studies show that this type of collaborative care model can reduce APACHE severity-adjusted ICU mortality by 25% and decrease LOS in the APACHE severity-adjusted low mortality patients, thus reducing overall cost of hospitalization. 4
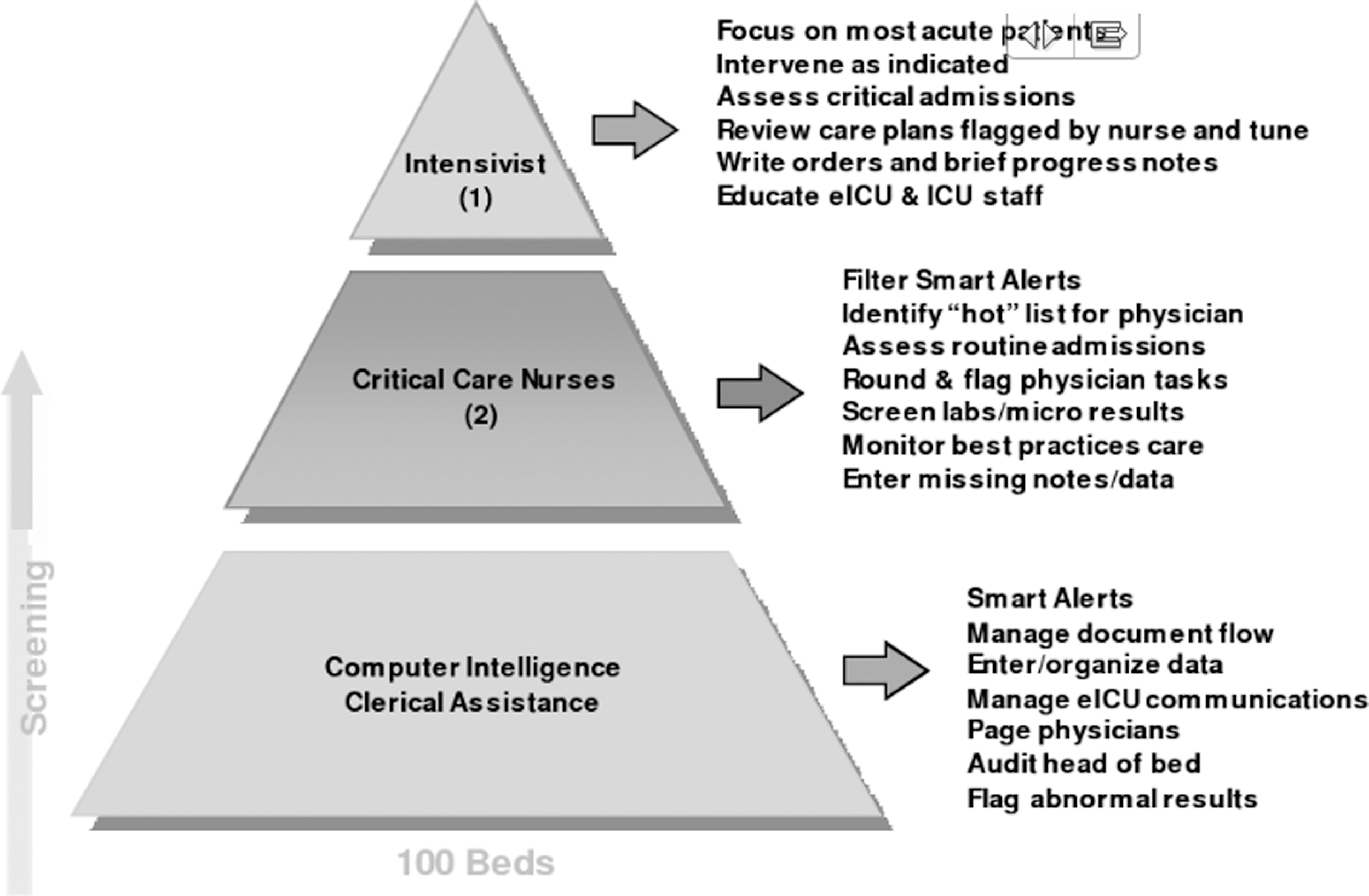
Philips eICU care team workflow. ICU, intensive care unit.
The tele-ICU R.N. can provide mentorship and expert guidance to the novice/advanced-beginner bedside nurse as well as collaborative support to the more expert bedside nurse. The nursing philosophy described by the "Novice to Expert" model of Benner 5 is one of transition from explicit rule-governed behavior (novice) to intuitive contextually based behavior (expert). Benner's philosophy proposes that both experience and mastery are necessary for skill acquisition and progression to a higher level of expertise. Paradigms and intuitions are developed based on previous patient care experiences. 6 The expert nurse uses quantitative data along with empirical and personal experiences to care for the patient. Clinical judgment requires attendance to a particular patient across time and takes into account changes and what has been learned. 6 Supplementing the expert nurses' intuition and knowledge with the tele-ICU technology brings nursing proficiency to a larger patient population.
The purpose of the study was to examine the impact of a first nurse-implemented tele-ICU staffing model, with the intent that shared nursing vigilance and collaboration can decrease patient complications, which may potentially impact patient outcomes.
Subjects and Methods
The quantitative pre–post study design was approved by the Investigational Review Board at Providence Alaska Medical Center (PAMC) in Anchorage. The study design included education of 90 regular staff nurses in adult critical care and 10 tele-ICU nurses and analyzed aggregated patient data of 1,308 patient participants at PAMC. Nursing and physician leaders set the tone of collaboration and patient outcome/safety benefit. Prior to implementation, bedside nursing staff participated in the planning of the tele-ICU program workflows with a vendor-facilitated clinical process redesign workshop. In the workshop, the bedside staff created workflows such as communication between the bedside and remote team and use of video assessment. Education and marketing tools were tailored to the nurse-only initial implementation with particular focus on the program metrics, communication norms between the tele-ICU and critical care nursing team, and support plans for new graduate bedside nurses. Tele-ICU nurses were hired into shared positions within both the critical care unit and the tele-ICU center. All had more than 5 years of critical care experience, held informal and formal leadership roles in the Adult Critical Care Unit, and were required to attain their C.C.R.N. certification within 1 year of hire into the tele-ICU center.
Population
The aggregated study patient population included those admitted to a PAMC critical care unit between January 1, 2009 and December 31, 2009. The data were further broken out to reflect the nurse-only period of January 1, 2009–September 1, 2009. PAMC, the largest medical center in the state, has a 28-bed open critical care unit with an intensivist physician program.
Data Collection Instruments and Procedures
Aggregated patient data were collected both pre- and post-tele-ICU program implementation. Twelve months of baseline data were collected: APACHE severity-adjusted ICU LOS and ICU mortality, incidence of ventilator-associated pneumonia (VAP), ventilator bundle compliance (stress ulcer and venous thrombosis prophylaxis), and glucose control. APACHE pre-data collection was completed on randomly selected patients (50 consecutive charts/quarter) for the four quarters preceding implementation of the tele-ICU program by trained nursing staff. During the data abstraction process at minimum 10% of charts were reviewed by the trained project lead for adherence to the APACHE methodology. Pre-implementation data, including VAP, stress ulcer and venous thrombus embolism prophylaxis, and glucose control, were manually collected and reported on by the quality improvement department. With implementation of the tele-ICU program, the data for APACHE LOS and mortality, ventilator bundle compliance, and glucose control were electronically captured, collated, and analyzed using the eCareManager Reporting Solution. The incidence of VAP continued to be collected by the health system infectious disease department.
After the tele-ICU program implementation, the critical care nursing leadership team identified a process improvement project involving adherence to physical restraint regulations of the Centers for Medicare and Medicaid Services (CMS). After a workflow and documentation analysis, it was determined that there was an opportunity for the tele-ICU program to assist by performing documentation audits and identifying when restraint order renewals were required. The tele-ICU nursing staff manually collected the restraint compliance data with quality improvement subsequently reporting the monthly data.
Results
Using the APACHE scoring system, a descriptive data analysis with a simple t test was done to compare daily patient ICU LOS, VAP compliance, deep vein thrombosis bundle compliance, and peptic ulcer disease bundle compliance. Additionally, core measurement data were collected for the Surgical Care Improvement Project (SCIP) to report the incidence of hospital-wide surgical complications.
Overall hospital LOS significantly decreased on a per day basis from 4.1 to 3.5 days (p≤0.05). Conversely, however, when compared with the full 2-day hospital LOS measurement, a decrease was demonstrated from 11.25 (per 2 days) to 9.19 (per 2 days) (p=0.064 or p≥0.05), which was insignificant (Table 1). Severity-adjusted mortality produced a decrease in actual to predicted mortality indicating the saving of 22 lives (Table 1).
Data Collection
APACHE, Acute Physiology and Chronic Health Evaluation; ICU, intensive care unit; LOS, length of stay; q, quarter.
Staff compliance measurement of the VAP bundle significantly increased 6%, from 87.2% to 93.3% (p=0.02). The incidence of actual VAP decreased by 13% related to a change in the median VAP from 2.99 in 2008 to 2.6 in 2009.
Compliance with both patient deep vein thrombosis and peptic ulcer disease bundles demonstrated continuous improvement of 1% and 0.5%, respectively. Although these results are statistically insignificant, they represent a consistently strong nurse understanding with the overall bundle in relation to patient outcomes.
Frequency of hypoglycemia, measured by glucose less than 50 mg/dL, decreased from 2.81% to 1.32% based on the number of days in which a patient had at least one reportable glucose value. In addition, the percentage of glucose values less than 50 mg/dL decreased from 0.44% to 0.21%.
Physician monitoring began in September 2009, 9 months after the initial activation of the tele-ICU program. Remote intensivist coverage was available for 10 h/night, 7 days/week, from 9 p.m. until 7 a.m. Ongoing collaboration after the addition of physician monitoring in the tele-ICU continued to focus on collaborative patient care opportunities with the addition of restraint and SCIP monitoring. In 2009, 69% (n=9) missed SCIP opportunities occurred on postoperative Day 2 for cardiac surgery patients, whereas in 2010 with the inclusion of the tele-ICU R.N., 43% (n=7) missed opportunities occurred on postoperative Day 2, resulting in a 26% improvement change.
Nurse documentation of patient restraint compliance moved in a continuously improved trend from 74% compliance pre-R.N. model to a consistent 100% compliance post-R.N. model in just 3 months after collaboration and inclusion of the tele-ICU R.N. in 2009.
Conclusions
Through nursing collaboration and assurance of best practice adherence the team produced the decreased ICU LOS. The cost savings for the ICU stay conservatively is $399,312 at an estimated ICU cost of $1,800/day. Decrease in the actual to predicted ICU mortality ratio is reflective of the collaboration between the bedside and remote caregivers. In addition, the use of the eCareManager software technology facilitated adherence to evidence-based protocols and early identification of potential adverse patient clinical status trends (Table 2).
Results of Nursing Collaboration and Assurance of Best Practice Adherence
Assumes average intensive care unit (ICU) cost/day of $1,800.
Assumes average hospital cost/day of $750.
Q, quarter.
Two aspects of the tele-ICU program implementation supported the nurse-only program success. First was leadership support and championing of the program. Executive leadership, consisting of the Chief Medical Officer, Assistant Chief Nursing Executive, and Chief Executive Officer, championed the program. Through discussion and education regarding the tele-ICU program mission and need, the critical care services leadership and frontline staff gained an understanding of the importance of the program and the need for collaboration. Nursing staff took ownership of the tele-ICU program on both sides of the camera. First, the bedside nursing staff changed their admission workflow to include notification of the tele-ICU staff of patient admissions. Second, the tele-ICU staff acquired the skill set of using the eCareManager technology and higher-level surveillance in contrast to the detail/task-laden workflow of the bedside nurse.
The tele-ICU nursing staff use of the daily management report facilitated adherence or identification of missing stress ulcer and venous thrombus embolism prophylaxis. This coupled with discussions during daily interdisciplinary rounds led to improved best practice adherence and the decrease in VAP rate. Collaboration beween bedside and remote caregivers, health system support for the quality improvement initiatives, and technology all contributed to the improvement as seen in the workflow.
As collaboration and adherence to best practice protocols improved, the team was more open to leveraging the technology and workflows in other areas of patient care. Restraint documentation and adherence to policy in accordance with The Joint Commission and CMS standards are anecdotally often cited by managers as a key concern across the country and at PAMC. The staff and leadership struggled to meet their compliance goals with restraint documentation. Until the tele-ICU nursing staff assumed the quality auditing role for restraint compliance, compliance was typically 70%. As the tele-ICU nursing staff monitored each shift for patients with restraints, they communicated missing documentation to the ICU staff. Compliance rose within 3 months of collaboration with the tele-ICU staff. The true quality improvement did not come from the audit but from the communication between the bedside and remote nurses.
Based on the restraint compliance success, a collaborative effort was made by the critical care team to more aggressively manage blood glucose levels in post-open heart surgery patients (SCIP), including improved use of insulin drips and starting long-acting insulin on postoperative day. The tele-ICU R.N.s were tasked with monitoring the blood glucose trends and actively following up with the bedside nurse and tele-ICU physician to create an individualized glycemic management plan for each patient.
The PAMC experience with restraint documentation and SCIP compliance exemplifies the American Association of Critical-Care Nurses' Healthy Work Environment Standard of True Collaboration: “True collaboration is a process, not an event. It must be ongoing and build over time, eventually resulting in a work culture where joint communication and decision making between nurses and other disciplines and among nurses themselves becomes the norm.” 7
In conclusion, the PAMC nurse-only tele-ICU program demonstrates that the use of technology, clinical decision support tools, collaboration, and communication all work in concert to improve patient care and outcomes.
Footnotes
Acknowledgments
The authors thank the bedside nursing staff and Adult Critical Care Unit nursing leadership for their willingness and support of the tele-ICU implementation and ongoing collaboration.
Disclosure Statement
C.R., J.M., J.F., and M.S. declare no competing financial interests exist. M.H., M.J., and E.C. are all employees of Philips Healthcare; participation in the project is or was part of their normal work duties.