
Abstract
Introduction
It is estimated that 64 million people suffer from chronic obstructive pulmonary disease (COPD). 1 More than 3 million people died of COPD in 2005, equal to 5% of all deaths globally that year. 1 COPD places a significant burden on healthcare systems worldwide. A major problem associated with COPD is the occurrence of exacerbations, which are acute events characterized by a significant worsening of lung function and symptoms. Seemungal et al. 2 reported the frequency of exacerbations as on average 2.7 per year in a population of 84 English subjects. Exacerbations are the most common cause of hospital admissions worldwide, and 40–50% of the patients discharged from the hospitals are readmitted the following year. 3,4 Furthermore, exacerbations result in increased utilization of healthcare services and decline in health-related quality of life. 5
Exacerbations are particularly managed with oral corticosteroids and antibiotics, 6 but patients seeking treatment for exacerbations often delay consultation for several days after the onset of symptoms, 7 a delay that often results in poor outcomes. 8 Hence, a common goal of COPD treatment is to prevent exacerbations. According to the Global Initiative for Chronic Obstructive Lung Disease, stable COPD is managed using a combination of interventions: smoking cessation, pharmacological therapy, education, pulmonary rehabilitation, nutritional interventions, vaccinations, oxygen therapy, and surgery. 6 One method for fulfilling these goals is to provide care and treatment between the patient's home and healthcare professionals with the support of communication and information technology (i.e., home telehealth). 9 Typically, a communication component is installed in the patient's home so as to facilitate information flow between the patient's home and health professionals. The information allows the health professionals to remotely monitor patient data and quickly respond as required. Another possible benefit is patient empowerment, based on an assumption that optimal outcomes of healthcare interventions are achieved when patients become active participants in the healthcare process. 10,11 Polisena et al. 12 have made a systematic review and meta-analysis of home telehealth by analyzing nine studies encompassing 858 COPD patients; they found that home telehealth reduces rates of hospitalization and emergency department visits. Sorknæs et al. 13 demonstrated that teleconsultations between a nurse and the patient tend to reduce early readmission and number of days in readmission. The clinical impact of home telemonitoring has been investigated in several studies by standardized approaches, such as questionnaires and satisfaction scales. Some of these studies revealed that patient satisfaction is high 14,15 and that patient quality of life increases, 16,17 whereas one study concluded that quality of life did not improve. 18 There are few studies investigating the clinical impact of home telemonitoring by assessing clinical parameters, such as blood pressure, oxygen saturation, lung function, medicine use, etc.
The aim of this study was to explore the clinical impact of home telemonitoring on COPD patients by investigating the development of clinical parameters during home telemonitoring.
Subjects and Methods
The Telekat Project
The data for this study were obtained from the TELEKAT project (Home Telehealth, Chronic Patients and the Integrated Healthcare System). 19 The aim of the TELEKAT project was to develop and test a preventive home telemonitoring program so that COPD patients could avoid readmission to the hospital by performing self-monitoring and maintaining rehabilitation activities in their own homes instead of being treated in a clinic. In this way, home telemonitoring could become a part of the patient's everyday life in the home environment. A telehealth monitor box was installed in the patient's home for 4 months. Based on wireless technology, the telehealth monitor collected and transmitted data about the patient's blood pressure, pulse, weight, oxygen level, and lung function to a Web-based portal or to the patient's electronic healthcare record. Healthcare professionals, such as general practitioners, district nurses, nurses, doctors, and physiotherapists, at the healthcare center or hospital had access to the patient's data. They could therefore monitor the patient's disease and training inputs and provide advice to the patient. Patients and relatives could also view the data on the Web portal and decide with whom they wanted to share these data about their condition.
Participants in this Study
In total, 57 subjects with COPD were recruited from the hospital, healthcare center, or general practitioners in the Danish city of Aalborg in northern Denmark. Inclusion criteria for entry to the study were age ≥18 years, diagnosed COPD 6 in stage III or IV, COPD as primary cause of reduction in function, and ability to understand oral and written instructions. The exclusion criteria for the study were those living outside Aalborg Municipality, heart disease that could limit physical function, mental illness, terminal malignant disease, severe rheumatoid arthriti, and pregnancy. The demographic characteristics of the subjects are shown in Table 1. Each subject was equipped with a digital weight scale (UC-321 pbt; A&D Medical), a blood pressure meter (UA-767 plus BT; A&D Medical), a pulse oximeter (Onyx II; Nonin), and a spirometer (Lung Monitor S; Vitalograph) and was followed up for a 4-month period. A clinician prescribed the measuring frequency for each patient. Hence, readings are not equidistant. One patient died after the inclusion and was therefore excluded because of incomplete data. All participants were informed in detail of the characteristics of the study, and written informed consent was obtained in accordance with the Helsinki Declaration.
Baseline Characteristics of the Subjects
Data are mean values.
BMI, body mass index; FEV1, forced expiratory volume in 1 s; MRC, Medical Research Council.
Ethical approval was obtained from the local Ethics Committees (August 27, 2008; protocol number N-20080049). The project was reported to the Danish Data Protection Agency (granted on August 7, 2008).
Assessment of Clinical Impact
To assess the clinical impact of home telemonitoring, the following eight clinical parameters were extracted: (1) prescription of corticosteroid (prednisolone) and antibiotics, (2) clinical consultations (general practitioner and emergency physician), (3) oxygen saturation, (4) forced expiratory volume in 1 s (FEV1), (5) forced vital capacity (FVC), (6) pulse, (7) diastolic blood pressure, and (8) systolic blood pressure. The first two parameters were extracted from the electronic health record. The difference between the mean of the first and the last month of the parameter readings was calculated (oxygen saturation is shown as an example in Fig. 1). The difference between the standard deviation (SD) of the first and last month of the parameter readings was also calculated for saturation, pulse, and blood pressure. This calculation is based on the assumption that a beneficial treatment may result in a stabilization of unstable short-term physiological parameters. 20 Because the use of the different measuring devices varied among individuals according to prescriptions, there is for some patients a complete lack of data for the first and/or the last month. Therefore, patients with no data for a given parameter in one of the periods were excluded for that particular calculation. From the baseline characteristics of the subjects in Table 1, pulse and blood pressure are too high, whereas oxygen saturation and lung function (FEV1) are too low. 20 The clinical impact of home telemonitoring is assessed as being beneficial if pulse is lowered, blood pressure is lowered, oxygen saturation is raised, or lung function is improved (raised FEV1 or FVC) during the 4-month study. Furthermore, the clinical impact may be assessed as beneficial if there is a reduction in medicine use or in the number of clinical consultations.
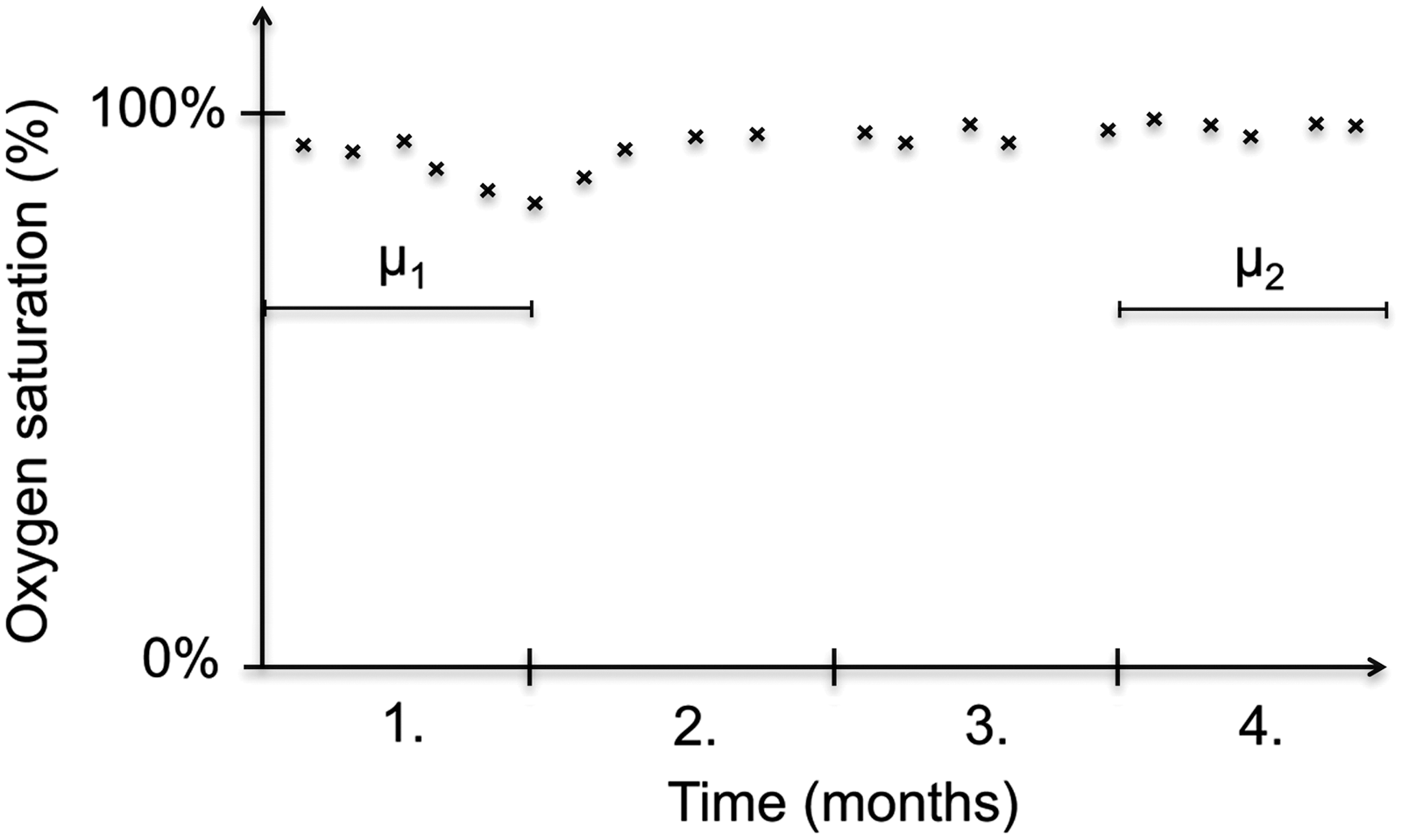
Clinical parameters were assessed during the home telemonitoring period by calculating the difference between the mean of all the readings during the first month and the mean of all the readings during the last month. This graph is a fictitious example where a patient has measured oxygen saturation in 4 months. The mean of the oxygen saturation readings for the last month (μ 2) is subtracted from the mean of the readings the first month (μ 1) to obtain the difference (D=μ 1 – μ 2).
Statistical Analysis
Each parameter was tested for normality by observing the histogram and QQ-plot of the parameter readings. The statistical analysis was performed using parametric or nonparametric methods, where appropriate. For parametric analysis, two-tailed paired t tests were used between the two periods. For nonparametric statistics,Wilcoxon matched-pairs signed-rank tests were used. The null hypothesis was rejected if p≤0.05. Data are presented as mean±SD values. Significant differences between the first and last months were further analyzed by correlating the mean of the parameter readings for the first month with the difference between the first and last months. The correlation was analyzed using linear regression. Goodness of fit was assessed using the coefficient of determination R 2.
The statistical analysis was performed in MATLAB® (release 2011b; The MathWorks) with the built-in Statistics Toolbox™. MATLAB is a software environment for algorithm development, data visualization, data analysis, and numerical computation.
Results
Table 2 shows the results of the home telemonitoring from the first to the last month. As observed in Table 2, the use of prescribed antibiotics and corticosteroids declined significantly (p=0.03) by more than 50% in the period. The contact with general practitioners also declined (p=0.05) from an average of four times during the first month to an average of three times for the final month. Systolic blood pressure declined (p<0.001) by 5.3 mm Hg, and diastolic blood pressure declined as well (p=0.02) by 2.2 mm Hg. Finally, the SD of systolic blood pressure declined (p=0.03). Saturation mean, saturation SD, FEV1 mean, FVC mean, pulse mean, pulse SD, and diastolic SD did not decline significantly.
Test Statistics: Results of the Two-Tailed Paired t Test
μ 1 is the mean of the parameter readings in the first month for the n patients, whereas μ 2 is the mean of the parameter readings for the n patients in the last month. The value of n varies because data are not available the first and/or the last month for some patients. D is the mean difference between first and last month (±standard deviation [SD]).
Wilcoxon matched-pairs signed-rank test.
bpm, beats per minute; CI, confidence interval; FEV1, forced expiratory volume in 1 s; FVC, forced vital capacity.
Figure 2 shows the relation between the parameters for the first month and the difference between the first and last months. It should be noted that for prescriptions and consultations, there are several patients with the same values. These manifest themselves in multiple points in the same spots in the graphs, marked with more intense circles. Those patients enrolled with high blood pressure improved most during the telemonitoring period. Especially for systolic SD, there is a close correlation between the level in the first month and the magnitude of the decline. The number of prescriptions and clinical consultations for the first month also shows a close correlation with the magnitude of the decline.
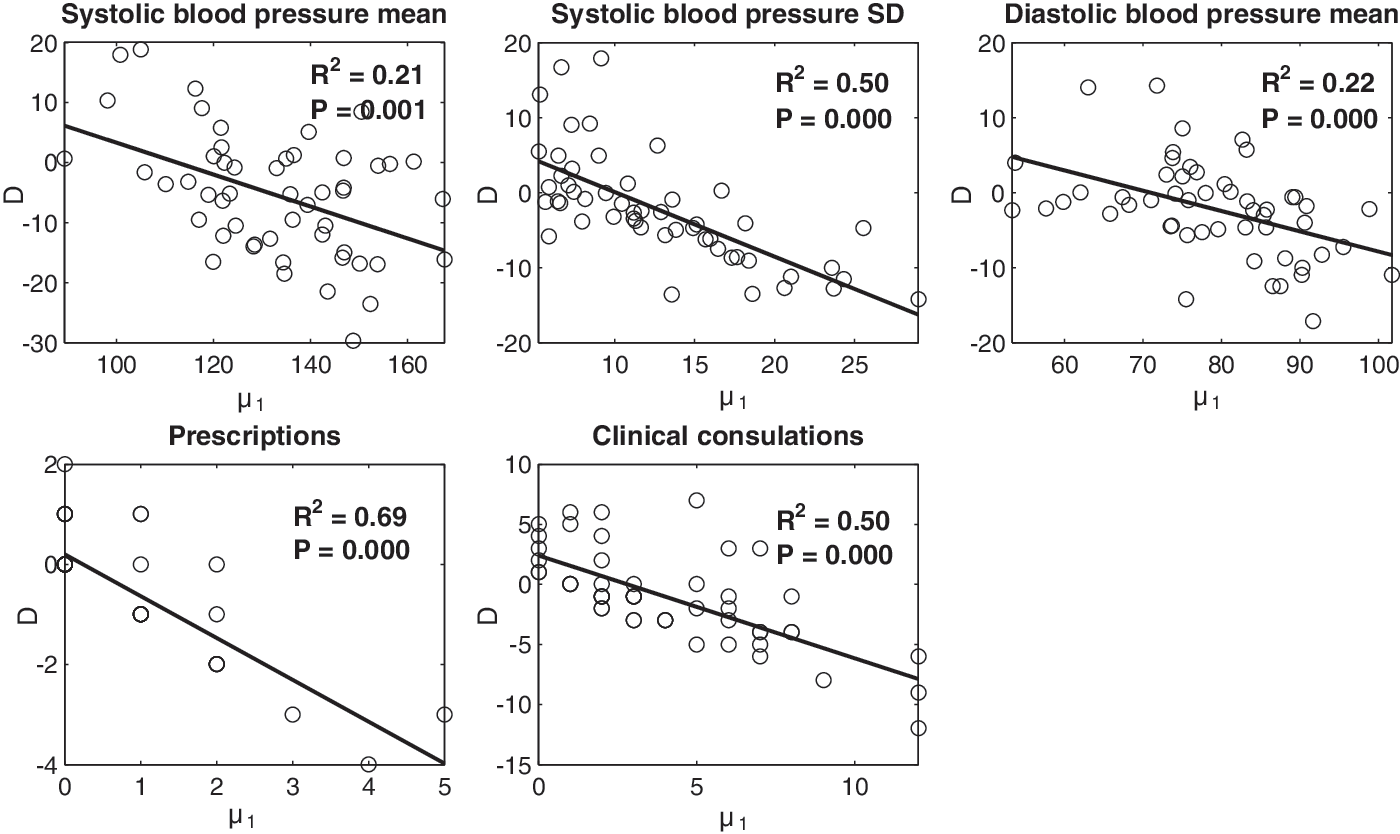
Correlation between the mean of the parameter readings in the first month (μ 1) and the difference between the means of the first and last months (D=μ 1 – μ 2): systolic blood pressure, systolic blood pressure standard deviation (SD), diastolic blood pressure mean, number of prescriptions, and number of clinical consultations.
Discussion
In COPD, exacerbations cause hospitalizations and reduced health-related quality of life. Several studies 12,13,21 have shown that utilization of home telehealth for COPD patients reduces rates of hospitalization and helps prevent early readmission. However, there is no consensus about whether home telehealth improves quality of life. 16 –18
In the present study, significant differences were observed in several clinical parameters. A significant decline was seen in the number of clinical consultations. This may be connected to an empowerment of the patients by telemonitoring: the patients are educated about their disease, feel more comfortable dealing with it, and therefore feel less need to seek assistance from healthcare professionals. This finding supports the findings by Polisena et al. 12 In their meta-analysis, the number of emergency department visits in general decreased, but only one randomized controlled trial reported a lower number of primary care visits. It should be noted that their meta-analysis dealt with both home telemonitoring and teleconsultation. On the other hand, a study by Lewis et al. 22 showed that home telemonitoring reduces primary care visits, whereas the number of emergency department visits remained unchanged.
The number of prescriptions declined by more than 50%, which contrasts with a study of telemonitoring by Trappenburg et al., 18 where no difference in the number of oral corticosteroids and antibiotics was observed. Antibiotics and corticosteroids are more frequently used in rehabilitation plans; the medication is prescribed in several treatments, enabling self-administration for the COPD patient. If, for example, the self-administration plan had commenced at the beginning of the telemonitoring period, with prescriptions for the total period, this could explain the reduction in prescriptions between the first and last month. On the other hand, clinical testing in the TELEKAT study was conducted in 2008–2010, and during this period, rehabilitation plans were not common; hence, this issue is not assessed as significant.
The significant decline in blood pressure may indicate that telemonitoring improves the short-term condition of the patient. The drop in blood pressure may be due to an increased awareness by the patient resulting from continuous self-monitoring using the blood pressure device. Moreover, the increased attention to blood pressure may encourage clinical health personnel to initiate hypertension treatment. Variation in systolic blood pressure decreases more from the first to the last month if the variation in the first month is higher. These observations accord with the hypothesis that telemonitoring increases patient empowerment and with the qualitative investigations of home telehealth in TELEKAT. 10 This is because patients with very unstable blood pressure may tend to care more about controlling their blood pressure once they have become aware of their condition. The change in blood pressure could be explained as a result of regression toward the mean. However, each patient was measured several times during the first and last month, such that regression toward the mean becomes implausible. COPD is an irreversible condition, where deterioration of lung function is a typical long-term outcome. Nonsignificant changes in the clinical outcomes of FEV1 and FVC suggest that home telemonitoring does not cause injurious long-term effects.
In conclusion, we evaluated the clinical impact of home telemonitoring in patients with severe to very severe levels of COPD. This study represents the results of a randomized noncontrolled 4-month trial. During the telemonitoring period, a significant decline was observed in blood pressure, clinical consultations, and antibiotics and steroids prescriptions. These results indicate that telemonitoring has had a positive clinical impact on patients with severe and very severe COPD.
Limitations
In a systematic review by Bartoli et al., 23 6 of 13 telemonitoring studies do not use a control group. This is also the case for this study, where only the intervention group was investigated. Given this limitation, the observed differences might be due to the patients becoming more focused on their disease after enrolling in the study. However, it was not possible to include a control group (who did not have telemonitoring) because the aim was to investigate developments in physiological parameters during telemonitoring. Another potential limitation of the study is the 4-month duration. However, the literature within home telehealth provides no documentation for the most effective duration of home monitoring. The choice of 4 months is therefore based on a trade-off between available resources (time, staff, and funds) and the need to have a sufficiently long enough period for the patients to become familiar with their own disease and to deal with their symptoms in the telemonitoring context. Further studies are needed to determine the most effective duration of home telemonitoring, but this is beyond the scope of the present study.
Footnotes
Acknowledgments
We wish to thank the COPD patients and relatives participating in the TELEKAT project as well as our clinical and industrial partners (for details, see
Disclosure Statement
No competing financial interests exist.