
Abstract
Introduction
The development and application of information and telecommunication technologies in the health field have as an objective to use the information to improve or increase health service (distant clinics, access to data bases, coordination of medical teams, etc.). The diagnosis and treatment of a high-prevalence disease with significant repercussions on health and effective treatment, such as obstructive sleep apnea syndrome (OSAS), could be provided to wide sectors of the population using telemedicine techniques. 1
The reference diagnostic method in OSAS is polysomnography (PSG), which requires specialist personnel and the patient staying overnight in the special sleep laboratory with a high use of resources. In this sense, the use of respiratory polygraphy with a record of the respiratory variables is currently accepted as a reliable diagnostic method, and there are numerous validation studies that demonstrate this. 2
The treatment of choice of OSAS, with unquestionable scientific evidence, is the use of continuous positive airway pressure (CPAP). 3 The recent introduction of treatment systems with CPAP, known as auto-CPAP, able to respond to changes in pressure according to modifications in flow, allows these systems to be used to optimize CPAP in the patient's home. 4,5
In the context of a highly prevalent process, 6 our group considered the real possibility of a “Virtual Sleep Unit” or “Wide Core Sleep Laboratory.” For this, we examined the technical feasibility of distant performance and transmitting, in real time, respiratory polygraphy telematically (PG-T), along with the sleep sounds and images of the patients, to our Sleep Unit. We also considered teleconsultation with the patients, the application of treatment with CPAP by means of the auto-CPAP pressure adjustment systems with data that could also be transmitted telematically. As secondary outcomes, the level of satisfaction of this method of healthcare was analyzed, and the cost of the procedure was examined.
Subjects and Methods
The central unit was our Sleep Unit of the Hospital Universitario de Burgos, Burgos, Spain. As a distant center, a recovery room was chosen in the District Hospital of Aranda de Duero, a city 80 km (50 miles) from Burgos.
In total, 40 patients from a patient population with clinical suspicion of OSAS were consecutively selected and studied using PG-T. They were attended locally by a nurse, and PG-T was performed and transmitted in real time from Aranda de Duero to the Burgos Sleep Unit (the remote point), where the technicians of this Sleep Unit continually monitored the polygraph recording and the sleep patient images, at the same time and with the same care as the rest of the patients who slept that night in the Sleep Unit. These technicians contacted the nurse at the local point by telephone, at the beginning and the end of the study and also when it was necessary.
A Sibelmed polygraph (Meditel Ingeniería Médica, SIBEL Group, S.A., Barcelona, Spain), with its own software (W-PLUS), was used for this, which recorded oral/nasal flow by means of a thermistor and a pressure cannula, chest and abdomen movements using plethysmography bands, heart rate, body position, snoring, and oxygen saturation (SO2). The patient could also be observed in real time by using a Webcam; thus the study was like an observational study and enabled signals to be recovered if these were degraded or lost, as the center had health staff permanently available who could be contacted (Fig. 1).
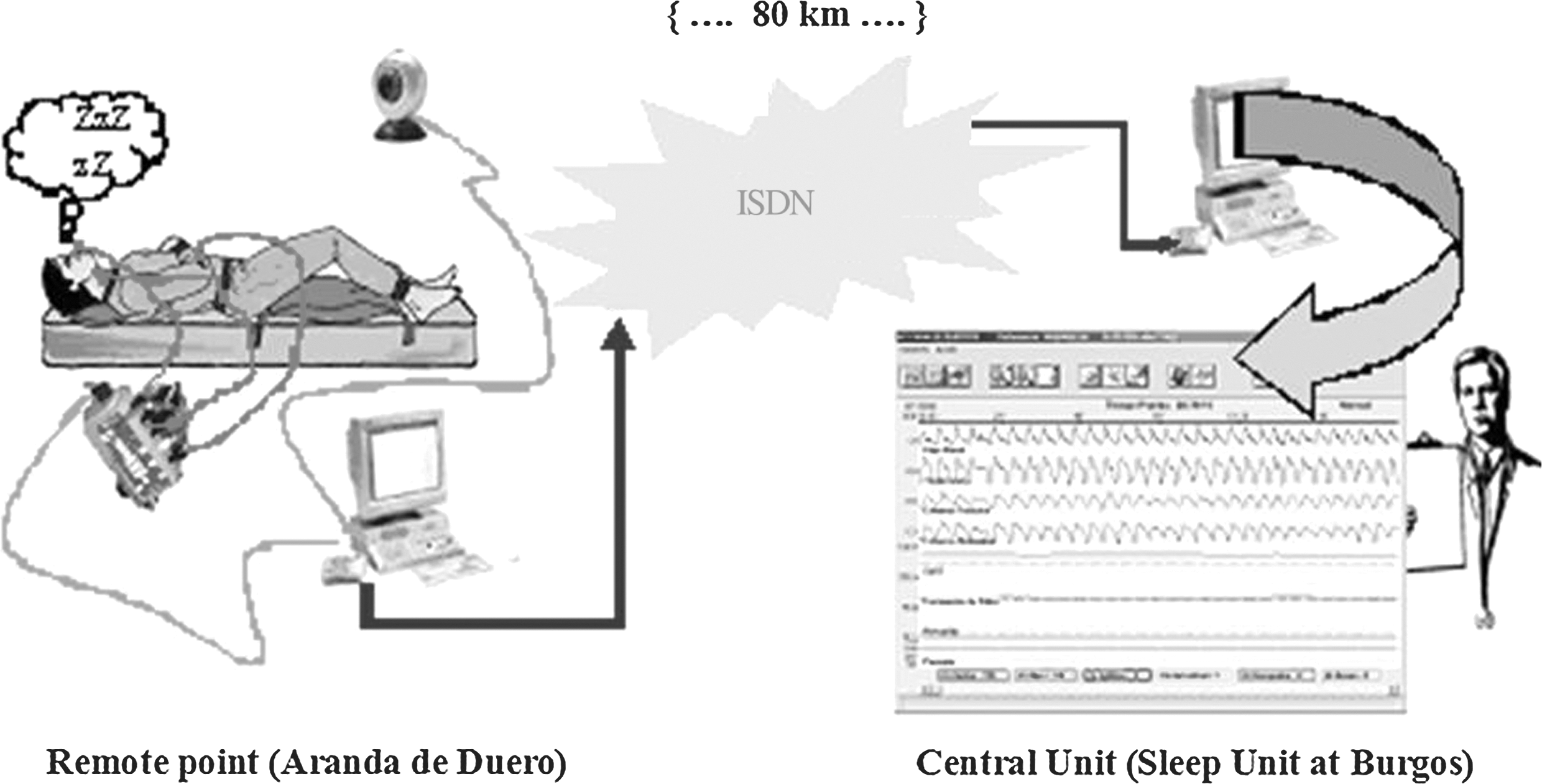
Diagram of the telematic procedure. ISDN, integrated services digital network.
The polygraph is capable of sending records via the Internet using e-mail, but this option was not used. Our original idea was the direct and continuous real-time transmission of the polygraph signals, using other additional software to share ports, in such a way that the recording collected in the local point (Aranda de Duero) was received in the computer of the Burgos Sleep Unit, as if the patient was in another bed of that Sleep Unit.
The polygraph, with its W-PLUS software, carries the CE mark and is considered a Class IIa health product according to Directive 93/42 EEC. The device complies with the International Organization for Standardization ISO 13845 standard quality guidelines and is approved by the European Union.
The polygraph used was not prepared for continuous record transmission. We searched for and found the technical solution to obtaining direct continuous transmission by connecting the polygraph locally to a computer, using commercial software that instructed the polygraph at the series port to dump the data into the central unit computer (80 km away).
The transmission of the polygraph chart data between the local computer (in Aranda de Duero) and the remote one (in Burgos) was done in real time because both computers shared the polygraph access serial port to the local computer. Commercial software (“Network Serial Port Kit,” © FabulaTech LLP, London, United Kingdom) can share physical serial ports with a connected device and then access this device from another computer over a local network or the Internet. Using this software we can share a physical serial port with a connected device (sensors or laboratory or clinical instruments, such as a polygraph, etc.) over the transmission control protocol/Internet protocol (IP) network or Internet. A virtual serial port was created on the remote computer from which to access the local serial device, and it is the exact copy of the physical serial port with the connected device. The polygraph was connected to the computer at the local point and worked with the serial device via the virtual serial port as if it was plugged into this remote computer (in Burgos). Data were forwarded over the network from the physical serial port to the virtual serial port, and vice versa.
The same polygraph signals were stored locally, and the file was physically transferred to the Central Unit to avoid losing it and to be able to compare the data stored in the polygraphs with those that were transmitted, for the purposes of this study.
The personal data of the patient was stored locally and not transmitted. It was not considered necessary to encrypt the signal for the transmission through a wide local area network (WLAN) because the local area networks of the centers were interconnected by integrated services digital network (ISDN) lines of the commercial telephone network. However, if data encryption was necessary, there would be no difficulty in doing this.
The patient's sleep at the local point (Aranda de Duero) was monitored by the Sleep Unit in Burgos, using an IP camera connected to the WLAN. The images were observed via a navigator directed at the IP of the camera.
The OSAS diagnostic criteria were those established by the Spanish Respiratory Diseases and Thoracic Surgery Society consensus. 2
After the polygraph study, the patients were randomized to receive a face-to-face consultation or teleconsultation. The face-to-face consultation was carried out in the usual way, and the teleconsultation was by videoconference, using IP videocameras, with four ISDN ports and a high-resolution monitor. Communication was made through the commercial telephone network, using a broadband of 375 kilobits per second (Kbps) using three ISDN lines. A nurse helped the patients with all the technical aspects of the videoconference; otherwise, the face-to-face consultation and teleconsultation followed the usual procedure for this type of consultation with a similar duration.
Those patients who were diagnosed with OSAS received auto-CPAP titration; in the case of patients who had been seen via videoconference, the data were transmitted telematically (Fig. 1). The patients who had been seen via videoconference confirmed the treatment in another teleconsultation. The validity of the teleconsultation was assessed by the level of compliance to the treatment with CPAP.
The level of satisfaction of the patients according to the diagnostic strategy used was analyzed by means of a visual analog scale from 0 to 10.
All the devices and systems used have received the required mandatory approval. Our innovative contribution was the procedure combining the devices used such as the polygraph with commercial software for networking, teleconsultations, etc., to create the Virtual Sleep Unit.
This research project, with its informed consent form, was submitted to the Burgos-Soria Clinical Research Ethics Committee, which gave its approval before the start of the study. Each patient was informed that the diagnosis would be made using a videoconference system, and all the patients signed the consent.
Statistical Analysis
We analyzed the agreement between the data transmitted telematically in real time and those stored in the polygraph once they were downloaded into the Sleep Unit computer. The analysis was performed blinded and nonconsecutively by the same observer.
The level of compliance to the treatment with CPAP was also analyzed, as well as the level of patient satisfaction with this diagnostic and therapeutic strategy.
An estimation was made of the costs of each one of the procedures, with the real cost of the equipment on the date the study started, which was the years 2004 and 2005. Staff costs have been calculated using figures corresponding to the average of these years, on gross earnings including the employer's Social Security payments.
Student's t test was used for the paired-sample analysis. Agreement was assessed with the Kappa index, and the intraclass correlation coefficient was used to evaluate the quantitative variables. The significance level was p<0.05 with 95% confidence intervals.
Results
In total, 40 patients was studied, of whom 15 were women and 25 were men, with a mean age of 53±10.3 years, a mean body mass index of 31±6.2 kg/m2, and a diurnal somnolence of 12±5.3 measured by the Epworth scale. In total, 35 patients were diagnosed with OSAS, with an Apnea/Hypopnea Index of ≥10, and 16 patients were started on CPAP treatment.
There were problems in data transmission for 1 of the patients studied (2.5%), but the problem was able to be partially resolved during the night, and the study did not have to be repeated. There were also technical problems in the transmission of data in 1 (6.25%) of the 16 auto-CPAP titration studies, and there were also problems in 1 (5%) of the 20 teleconsultations.
In Table 1, excellent agreement can be seen when the data transmitted in real time were analyzed and when the data stored in the polygraph were assessed, as regards Apnea/Hypopnea Index, total apneas and hypopneas, mean SO2, and time with SO2<90%.
Of the patients diagnosed with OSAS, 16 received treatment with CPAP, and for this they were studied with auto-CPAP in a maximum of 2 nights with data transmitted telematically. There was a face-to-face consultation for the commencement of treatment with CPAP in 9 patients and in the other 7 by videoconference.
Correlation Coefficients Obtained with the Data Transmitted in Real Time and the Data Stored in the Polygraph
CI, confidence interval; SO2, oxygen saturation.
The level of compliance with CPAP treatment, defined as a use of more than 4 h/day and more than 5 days/week, when analyzed at 6 months, was maintained by 85% for the patients who received treatment by conventional visit and 75% of those seen in teleconsultations.
The level of satisfaction, measured by a 0–10 visual analog scale, both for the overall evaluation and for the diagnostic strategy, was 9.50±0.72.
Tables 2 and 3 show the breakdown of the estimated costs for implementing a telemedicine strategy compared with the conventional one. Based on our own data, a PSG study has a mean cost of 148.78 € in our Unit, 7 and a telematic study has a mean cost of 227.08 €, for the usual costs of equipment, communications, and staff costs of the years 2004–2005.
Cost of Polysomnography in the Sleep Unit
127.73 € excluding amortization of polysomnographs.
Remote Study Costs
The staff costs are for the year 2010, corresponding to gross pay, including employer's contribution in a public health service center.
222.87 € excluding polygraph amortization.
ADN, Advanced Diploma Nurse; IP, Internet protocol; ISDN, integrated services digital network.
Discussion
The results of this preliminary study show that the use of new information and telematic communications technologies can help to establish diagnostic and therapeutic strategies for sleep apnea syndromes, maintaining an appropriate cost-effectiveness ratio and providing the possibility of avoiding traveling by the patients. 8
This study was designed to analyze the reliability of a new telematic system that combines direct point-to-point data transmission and the use of automatic CPAP systems and teleconsultation by videoconference to establish a therapeutic strategy. Thus, it is not a randomized controlled clinical trial and has methodological limitations, mainly due to the small sample size and a selection bias, because the majority of patients have a high suspicion of sleep apnea, and this ensures a high diagnostic yield and also a possible higher level of compliance.
The gold standard for the diagnosis of disease processes other than sleep apnea, such as restless legs syndrome, narcolepsy, parasomnias, etc., requires the study of neurophysiological variables, obtained using PSG in a sleep laboratory. This study has been performed using a polygraph instead of PSG as the aim was to determine the efficacy of the procedure with a pilot study; it is easy to deduce as obtaining a recording of a polysomnograph and including all the neurophysiological variables in the data transmission is just as feasible. Furthermore, as happens in sleep laboratories, it is possible to detect recording anomalies when they are produced, using data transmission in real time to the Sleep Unit, as well as to intervene locally to obtain the signals, if required, something that is impossible in polygraphic studies in the home.
There is limited previous experience in this field. Thus, Kristo et al. 9,10 evaluated a system based on the transmission of data using an Internet FTP protocol (the conventional system for file transfer) between October 1999 and April 2000 for the diagnosis of OSAS. The polygraphy data were collected in the Walter Reed Army Medical Center in El Paso, TX, and the interpretation was made by the highly trained staff of the Sleep Unit, demonstrating that remote study is technically and clinically feasible, with a good cost-effectiveness ratio and of clinical use to improve patient accessibility to these health resources. Pelletier-Fleury et al. 11,12 comparatively evaluated the cost and effectiveness of PSG telemonitoring and PSG by conventional unsupervised home telemonitoring, demonstrating that remote telemonitoring made the procedure clearly superior from a technical point of view and was preferred by the patients.
One important aspect is the compliance with the treatment, 13,14 which in our study remained at 85% after 6 months of follow-up when the control system was a conventional consultation and 75% in a teleconsultation-based system. Stepnowsky et al., 15 in a pilot study, randomized 45 patients to a teleconsultation and conventional consultation follow-up for 2 months and observed no differences in the levels of compliance with CPAP.
With our data, the estimated cost of a telematic polygraph was around 227 €. In the cost analysis of the series by Pelletier-Fleury et al., 11 they obtained a cost of $244 for PSG telemonitoring, whereas the PSG with conventional unsupervised home telemonitoring was $153, leading to the conclusion that there is a need to evaluate these types of diagnostic systems, particularly for geographical situations that can generate significant transport costs.
The extra cost of remote studies may be gradually reduced as information systems and communications extend and develop. The healthcare infrastructure savings also have to be taken into account. If we add up, for example, the two traveling costs avoided by the patients and the working days that they did not lose, we could estimate that the real cost would be similar or lower than that of conventional PSG and would also have the added value of conceptualizing the Sleep Unit further from the reference site, with diagnostic techniques available in other health centers and hospitals, whether at a different healthcare level or not.
The aim of our study was to demonstrate the reliability of telemedicine in the diagnosis and treatment of sleep apnea syndrome. At the time the study was performed the option of an interconnection using an asymmetric digital subscriber line was not available in time and at a reasonable cost. We avoided using the Internet, as well as access to networks using Wi-Fi technology, for confidentiality reasons, among others.
To have a suitable and constant broadband available to transmit high-quality images in real time throughout the study, three ISDN lines (each 128 Kbps) were rented from the commercial telephone network because during the study period the local area network of the centers themselves lacked this capacity. Although one ISDN line was sufficient to transmit the sleep recording and the study surveillance Webcam signal, the teleconsultations used three ISDN lines.
Currently, this cost would be very different because these centers connect their respective local area network to an intranet-type network using commercial products, such as high-performance asymmetric digital subscriber line-Wi-Fi, with greatly reduced costs.
Our work shows the real costs that were incurred in the project. The costs of transmission have been separated in order to adequately explain the origin of each cost. If we compare the costs of Table 2 with those of Table 3, we see that the cost difference between the studies is 30.96 €, excluding the depreciation costs of the polygraph/polysomnograph.
The data are for guidance because a rigorous study should also take into account the cost of the bed/night in one or the other center, the travel savings, etc., as well as a proportion of the costs due to failed studies. The aim of these cost tables is only to show that it is not a particularly costly procedure. On the contrary, it could be more economical, as it extends the area of the central Sleep Unit and uses its resources to attend to a much greater population, thus increasing the efficiency of the Unit.
The main contribution of the study is that we have shown that it is possible to diagnose sleep apnea syndrome in patients located in health centers of a lower care level, by transmitting, in real time, images, sound, and polygraph recordings of a sleeping patient to a Sleep Unit. We have also managed to establish treatment with CPAP, after the appropriate pressure adjustment titration and instructing the patient by means of videoconference consultation. We have shown that this form of telemedicine maintains long-term compliance, avoids patient travel, and keeps them satisfied. We may consider that this group of distant points connected by information and communication systems with a central Sleep Unit is a true Virtual Sleep Unit, where the central Sleep Unit becomes a real control center for the diagnostic, therapeutic, and patient follow-up processes (process management).
The cost in communications reported in our work has a very relative importance because of the gradual extension of the networks and the variation in the associated cost differs considerably over time and between regions and countries.
We used IP videocameras that provide a high-quality videoconference for the teleconsultations. This system is expensive and was possible as we had the equipment available before the study. However, this kind of application could be implemented with new technological devices. The development of a camera and imaging transmission system in real time is advancing rapidly. Teleconsultation experiments via the iPhone® (Apple, Cupertino, CA) have already been published, as well as other diagnostic and therapeutic applications using mobile phone technology with considerably lower costs. 16 –18 That is the reason for not including the cost of the videocameras used in the teleconsultations. As Liu and Liu 19 wrote, with the help of electrical and mechanical technologies, it is expected that a full combination between the biomedical sensors and mobile phones will bring a bright future for the coming pervasive medical care.
The strong point of our work is the optimization of the human and technological resources of the Sleep Unit because it becomes more efficient with a “virtual” increase in beds that are lower in cost. The District Hospital resources also increase as it makes possible the diagnosis and treatment of sleep apnea patients in its catchment area, at a minimal cost and without traveling costs, which is more comfortable for the patient.
This Virtual Sleep Unit extends the possibilities and advantages of a Sleep Unit, well provided with staff and resources, to health centers of a lower care level, thus providing specialized healthcare to a geographically distant population and a saving of patient travel time and expense. Furthermore, it improves the efficiency of the central Sleep Unit as it provides comprehensive care to more patients with sleep apnea with a lower proportion of specialized staff, as well as optimizing its resources and using lower cost hospital beds.
More studies need to be performed in order to analyze the diagnostic yield and its behavior in terms of cost and treatment compliance when applied to a nonselective population.
Footnotes
Acknowledgments
We would like to thank the Regional Government of Castilla y León, which provided funding support for this project (grant GRS 27-04).
Disclosure Statement
No competing financial interests exist.