
Abstract
Introduction
Men's Health and Help-Seeking
In the Western world men die earlier than women. Life expectancy varies among groups of men in and among countries. 1 –4 Males are vulnerable from birth, and their health is cumulatively disadvantaged over time. 2,5 Men understand health differently from women, 3 are less knowledgeable about personal health, 1,2,4 take more health risks (particularly young men), live a riskier lifestyle, and work in risky environments. 1,6 –8 Men view the most powerful men as those for whom health and safety are “irrelevant”; they are less likely to have a general practitioner (GP), and they have shorter consultation times than women: help-seeking for minor issues “put(s) masculinity up for scrutiny.” 8 Men delay seeking help for health issues so when seen they are more unwell than they need be. 2,3,9 –11
Men use an indirect approach to help-seeking—partners and friends are a primary resource; however, men do respond to innovative ways to provide healthcare or advice. 11 Barriers that inhibit men from seeing a GP include a lack of understanding of the concept of health, lack of knowledge about appointment making, time constraints, negotiating with female receptionists, unsuitable opening hours, and concerns about confidentiality and trust. Furthermore, men may be uncomfortable in a feminized environment and uncertain with the language needed to describe their symptoms. Traditional health settings do not encourage men to seek help. 1,2,4,11,12 Novel approaches to providing health services specifically for men may increase help-seeking: men care about their health and were “willing and able to engage with the right (for them) health services,” and men from “hard to reach” cultural and socioeconomic backgrounds used the services. 12 Specialized health services may be required to encourage men to seek help.
A telephone health service like Healthline might reduce some of the barriers to men's help-seeking and provide an alternative for men seeking health advice. 2
New Zealand Men
New Zealand men die 4.2 years earlier than women. 2 –4 Men from some ethnic groups or from socioeconomically deprived areas and the less educated have poorer health than other men. 3,10,13 Men were less likely than women to have a primary care provider and “significantly less likely to have seen a general practitioner in the previous year.” 10 The most common reasons for the unmet need were not wanting to make a fuss and not having the time. 3,14 The greatest unmet need for GP services for all men is in the 15–24-year age group. 14
Young Men's Health
Younger men have a more fragile “sense of self.” 3 They drink hazardously, are sexually active, engage in risky behavior, and may exhibit violent behavior. 10 Young New Zealand men see sportsmen, particularly rugby players, as ideals of health, resilience, and the ability to withstand pain. 15 Young men appear helpless when left to organize their healthcare: the entire concept of accessing primary healthcare eluded male teenagers. 1 It was something that had previously been done for them by female family members. In New Zealand those in the 15–24-year age group are significantly less likely to have a GP than those 14 years old and under; the greatest number of young men without a GP is in the 25–34-year age group. 14 Thus surgeries, later in life, are alien places. 1 Being unwell and accessing health services may be viewed as feminizing and diminishing their masculinity. 2,15 To young men good health is health that allows physical functioning, so help-seeking may be delayed until functioning is severely compromised; cost of healthcare, lack of confidentiality, anonymity, and trust of the health professional create further barriers to young men accessing healthcare. 15
Older Men's Health
As men age the gender roles and associated stereotypes alter; independence in relation to health and help-seeking is more a “marker” of successful aging than maintaining masculinity—so that being independent may be “health enhancing” but also “health damaging.” Help-seeking may be motivated by quality of life rather than survival. Older men were willing to talk about their health problems in the right environment and over their life may have had illness experiences that encourage help-seeking. 16,17 Older men appreciated good relationships with their GP. 3 New Zealand men 65–74 years old were equally likely and men over 75 years old were more likely than women of the same age to have a GP. 14
Subjects and Methods
Healthline and Telephone Health Advice
Healthline is funded by the New Zealand Ministry of Health, free and available 24 h/day. A registered nurse determines the reason for the call and assesses and advises as required by the caller's needs. Telenurses work at a computer, wearing headphones and using decision-aid software and data collection programs. Healthline has been provided since 2000 by McKesson Asia Pacific, now owned by Medibank Health Solutions, and is a key part of New Zealand's primary health sector. One of Healthline's objectives is to increase timely and appropriate access to health advice and services by groups with poor access to or utilization of primary healthcare. 18
A caller presenting with symptoms is triaged. The triage outcome (disposition) depends on answers given to software-prompted questions with descending levels of acuity and on the clinical judgment of a telenurse.
The triage dispositions may be any of the following: 1. 111 call for the appropriate service 2. See GP or go to emergency department immediately 3. See GP within 24 h 4. Seek medical advice within 72 h 5. Self-care advice for home care
Callers to Healthline
Calls are received throughout the day with peaks at 8 a.m. and 7 p.m. In the October–December 2010 quarter, 77.9% were from callers with symptoms that required assessment; of these, 2.9% required an ambulance, 17.6% required urgent care, 34.5% needed to see a GP within 24 h, 18.6% needed to contact a provider within 72 h, and 26.5% of callers were advised they could manage their symptoms at home. Of all callers, 63.4% were European, 18% were Māori, and 5.4% were Pacific people. 19
Callers heard about Healthline from a variety of sources: 70.5% of callers were repeat callers, with word of mouth accounting for a further 8%. Repeat callers and their word of mouth endorsement are clearly important marketing factors for Healthline.
An independent survey found that men were less likely than women to know the service was free and that it was registered nurse based. More men than women identified a lack of trust in the service. On the other hand, men who did call were more likely than women to have found the service “very helpful.” 20
Procedures
Data were obtained from information collected routinely through automated documentation systems. A caller was defined as someone calling for him- or herself about his or her own health.
A random week in October 2010 was chosen. The total number of calls for the week was 3,278. Removing asymptomatic callers, those under 18 years of age, those whose age or gender was not recorded, anonymous callers, and calls where no disposition was recorded left 487 men and 2,120 women. A control group of 487 women was randomly selected by computer.
Deprivation scores of 1–10 are applied to meshblocks and derived from variables from the 2006 New Zealand Census that reflect deprivation. After data were rendered unidentifiable, meshblock IDs were attached to each record and matched with meshblocks in the NZDep 2006 Index of Deprivation; 86% of the sample was able to be geocoded. For this study deciles were converted to quintiles. The least deprived areas have a score of 1, and the most deprived have a score of 5.
Results
In all age groups there were more women than men callers (χ2 [5 df]=31.1, p<0.001) (Fig. 1). The difference was most marked in the 18–29-year age group (only 7% of all calls were from young men in this age group, compared with 30% of all calls from 18–29-year-old women) and became progressively less marked with age.
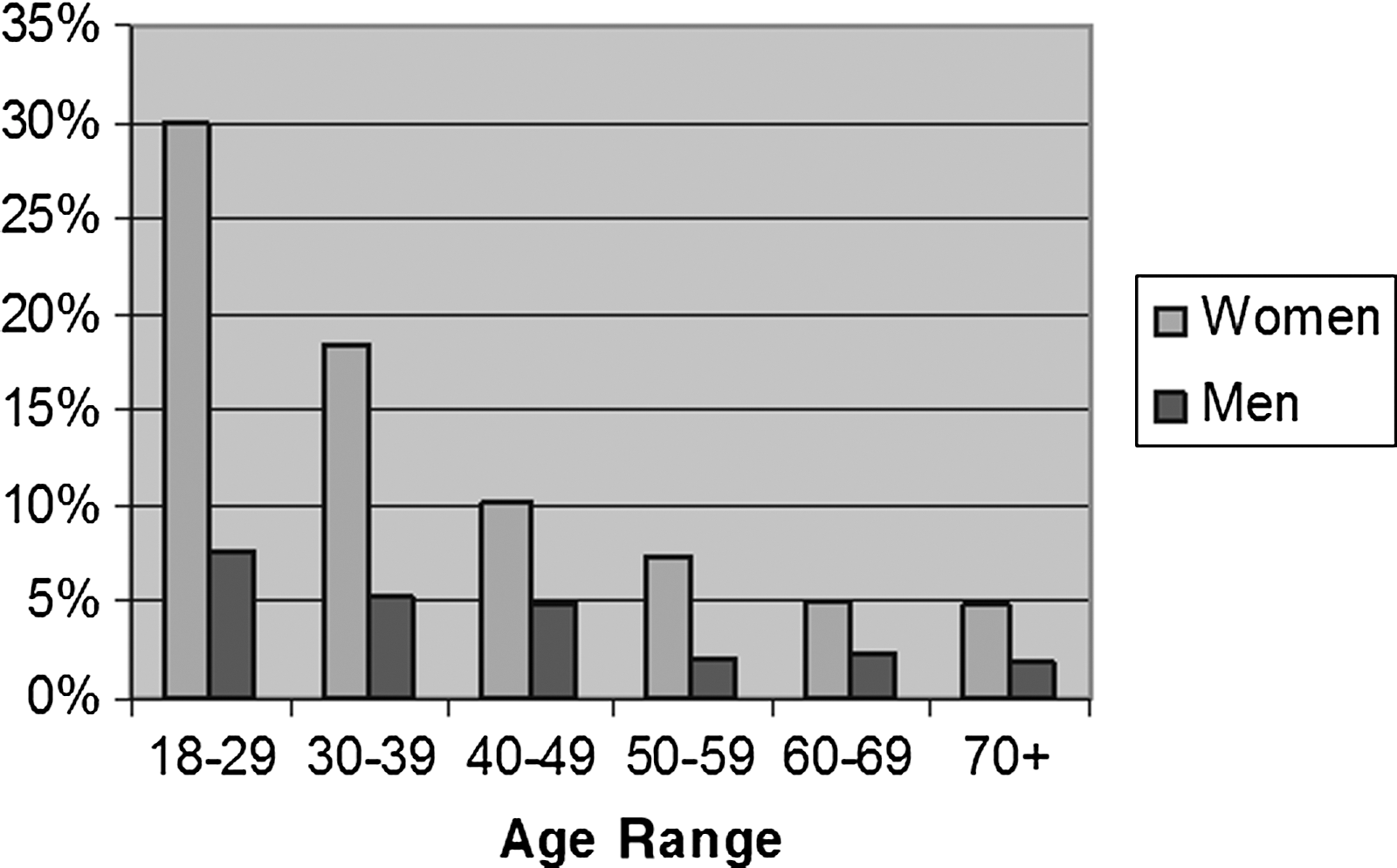
Percentage of all calls during the study week by age group and gender (2,120 women, 673 men).
Mean call durations were a little longer for callers under 40 years of age and shorter for callers older than 40 (F 5,962=4.15, p=0.001), but not significantly different between male and female callers (F 1,962=0.18, p=0.672) (Figs. 2 and 3).

Call duration by gender for 487 men and 487 women.

Mean call duration by age and gender for 487 men and 487 women.
There was no significant difference over the 24-h period in the calling pattern by gender (χ2 [5 df]=8.737, p=0.12) (Figs. 4 and 5) or by age.
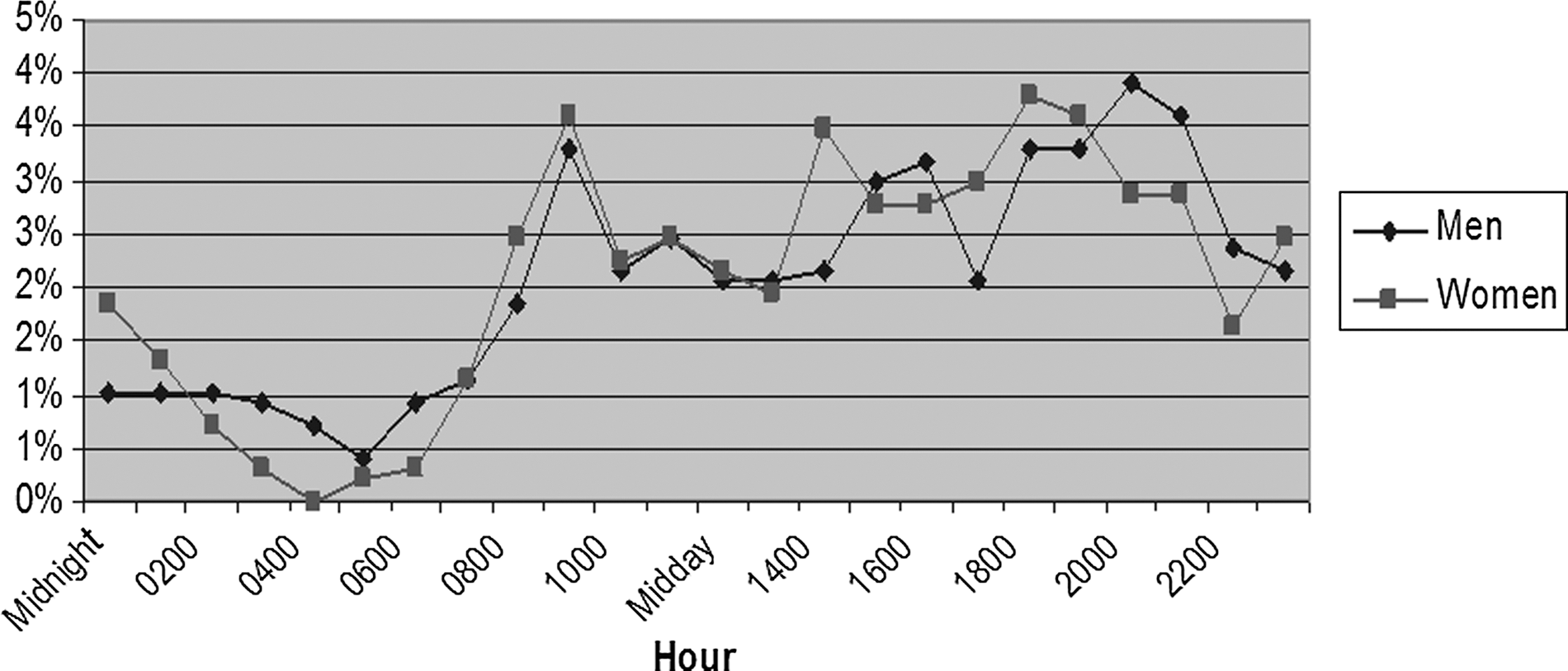
Percentage of all calls by hour of day for 487 men and 487 women.
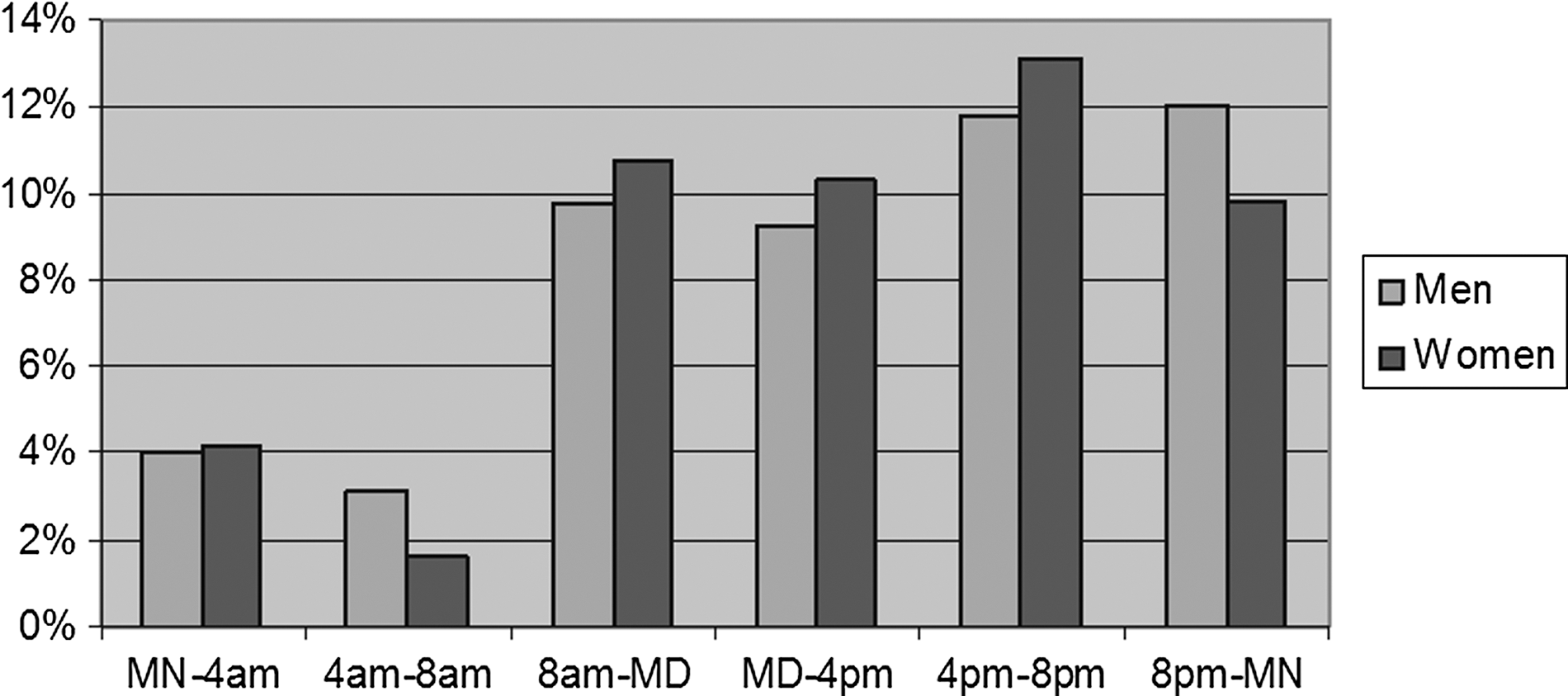
Calls over a 24-h period by 4-h time block and gender. MD, midday; MN, midnight,
European, Māori, Pacific Island, Chinese, and Indian ethnicities were identified for the audit. Compared with their representation in the population, European men and Māori women were overrepresented, and other ethnic groups were underrepresented (Fig. 6).
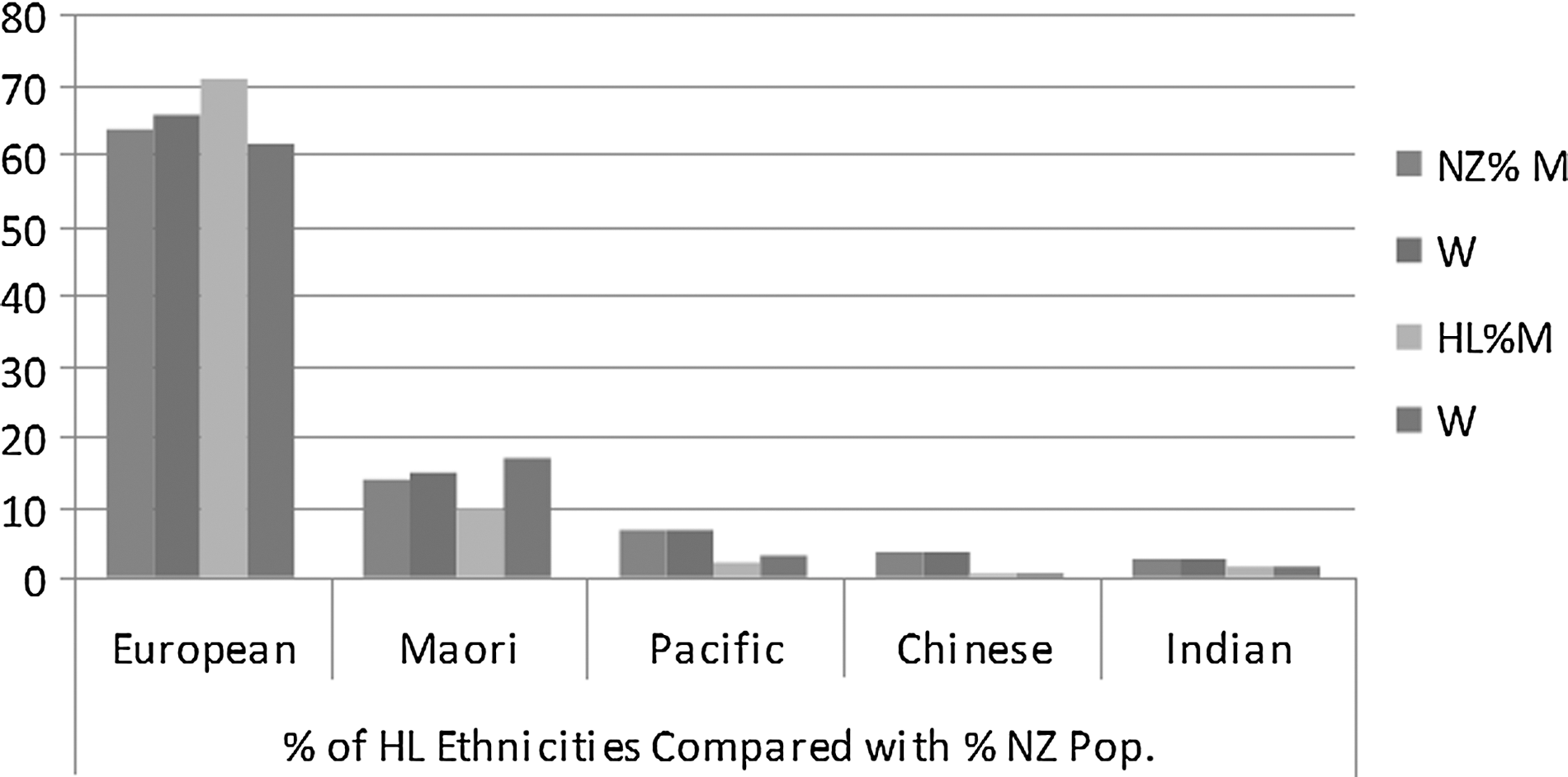
Percentage of Healthline (HL) callers by gender and ethnicity of sample compared with total New Zealand (NZ) population. M, men; W, women.
Men were less likely than women to be calling from an area of high deprivation (Fig. 7).
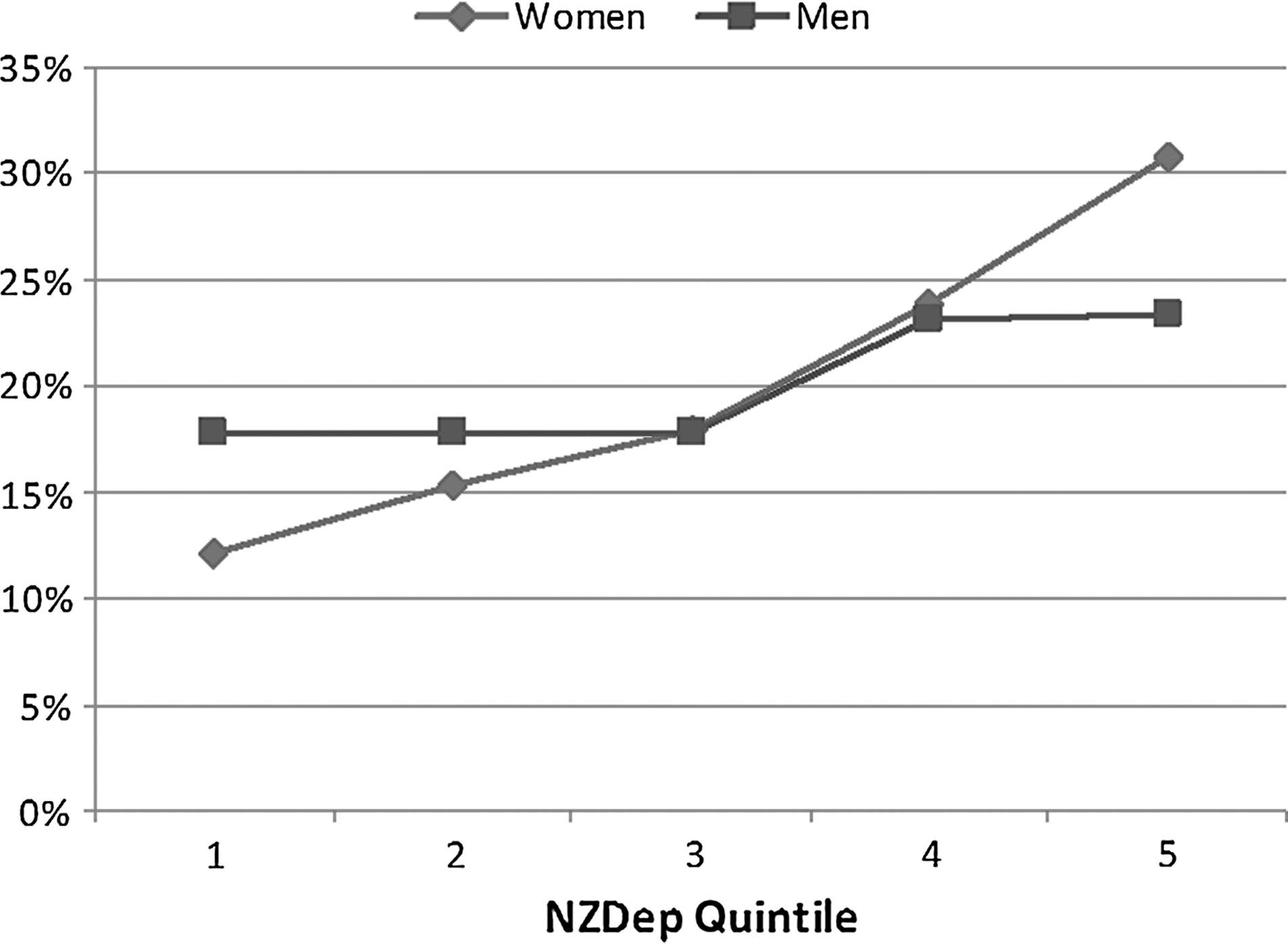
New Zealand deprivation (NZDep) quintile (from 1=least deprived to 5=most deprived) by gender.
There were no significant trends in acuity across quintiles of deprivation (Fig. 8).
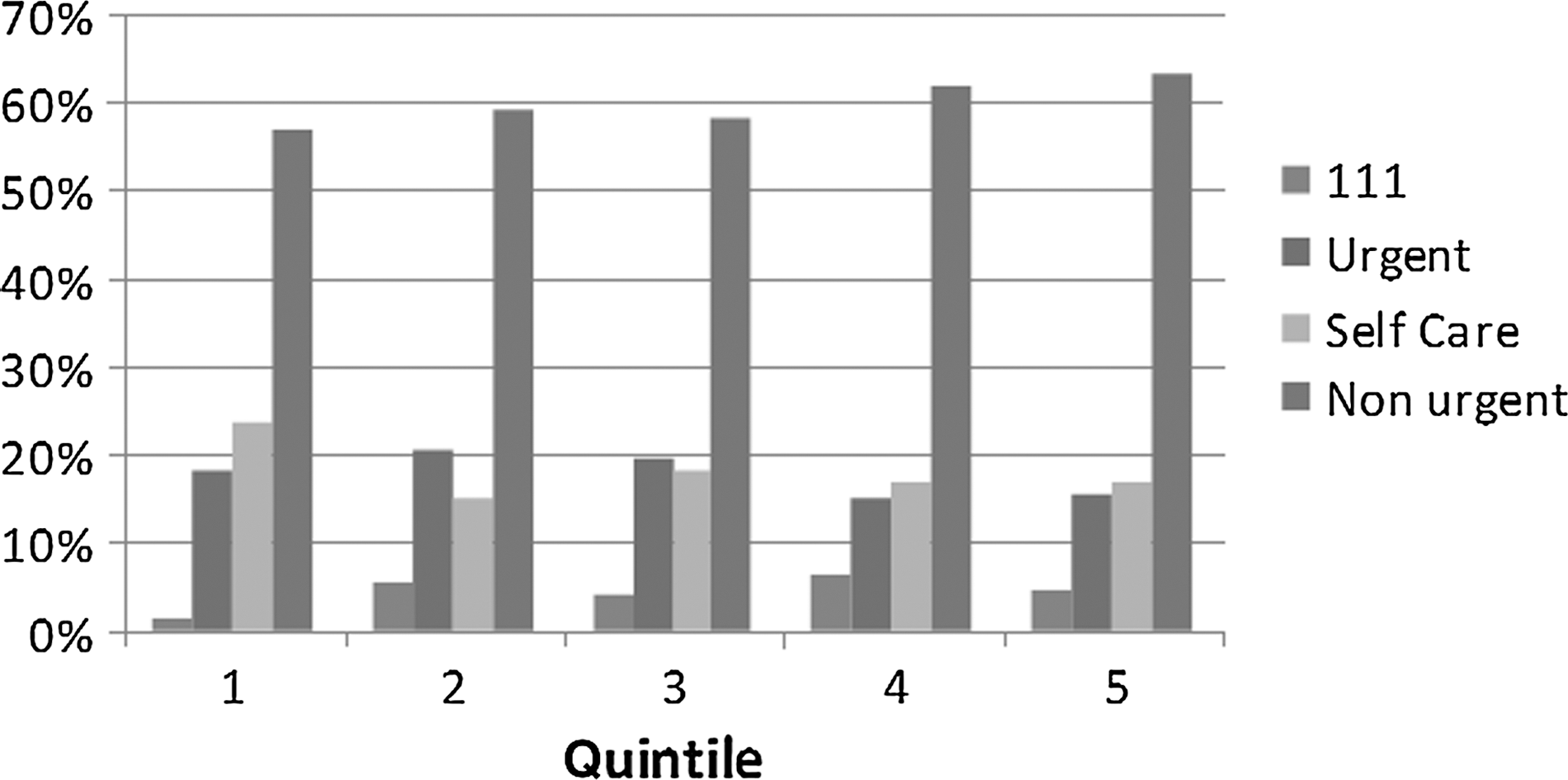
Men only: New Zealand deprivation quintile (from 1=least deprived to 5=most deprived) by acuity.
Overall, there was a trend for younger men to be triaged to higher dispositions than women, although the opposite was true in the older age groups (Fig. 9 and Table 1). No differences in acuity could be discerned among men from different ethnicities.
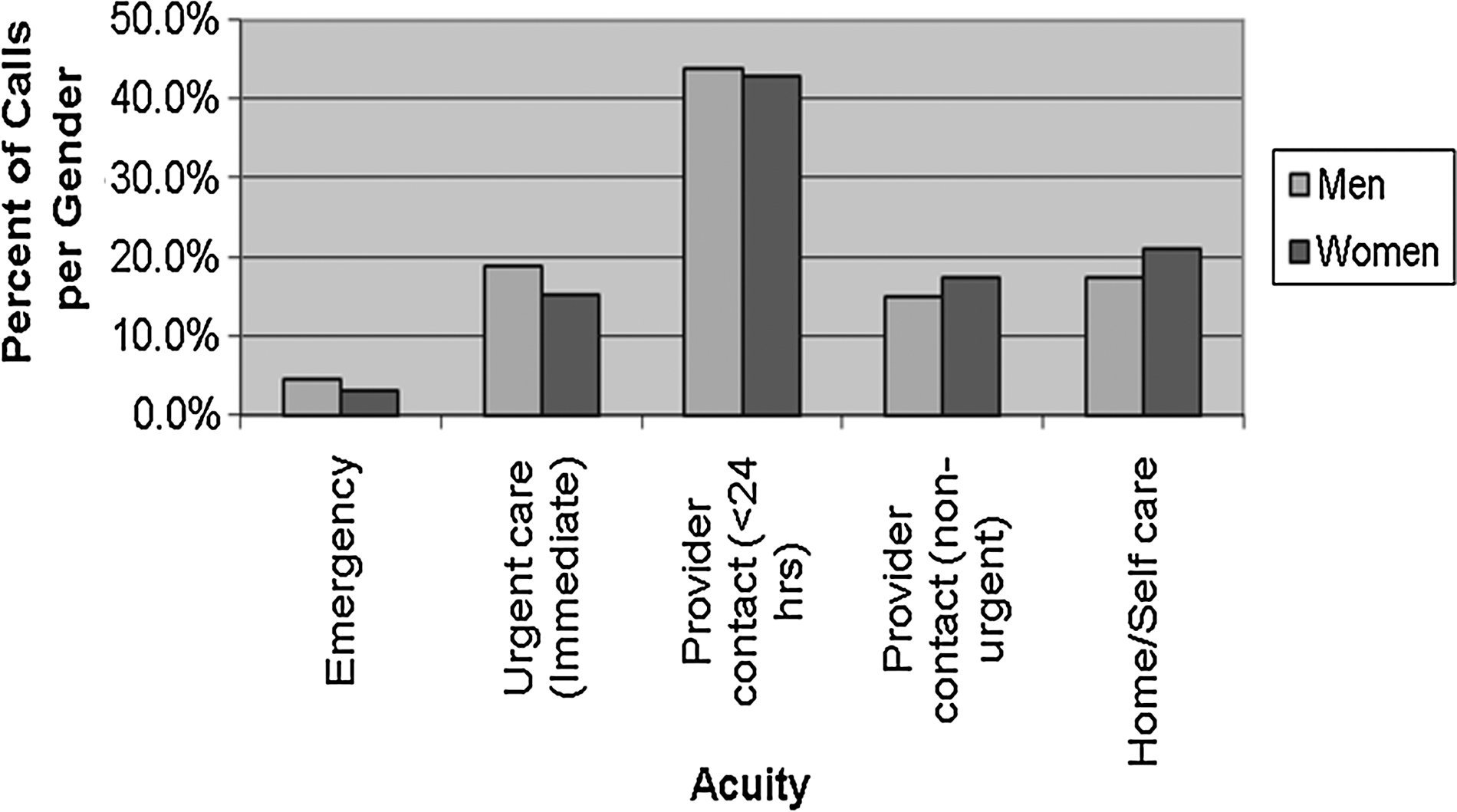
Acuity of call by gender.
Percentages and 95% Confidence Levels for Different Dispositions After Calls by Men, Compared with Those from Women, in Different Age Groups
Data are mean values (95% confidence intervals).
Discussion
We had supposed from the primary care literature that fewer men than women would call Healthline, but that (compared with women) they would be more likely to call after hours, would be more acutely unwell, would therefore take less time to triage, and would be triaged to higher dispositions. Those trends would be more marked in “hard to reach” groups—younger men, ethnic minorities, and the socioeconomically deprived.
Indeed, we found that fewer men than women called Healthline, a trend most evident in younger age groups. Younger men were more acutely unwell than women (they were more likely to need to see a GP and were less likely to be able to care for themselves at home than women). European men and Māori women were overrepresented compared with their representation in the general population, and other ethnic groups were underrepresented. Men and women from higher deprivation regions were more likely to call. There were no differences between men and women in time of day or duration of call. There were no differences in the acuity of calls from men of different ethnicities or different deprivation quintiles.
Men (and women) in the 18–29-year-old group were a larger proportion of callers than any other age group. The greatest need for the younger age group is immediate care and to see a GP within a 24-h period. Men 18–39 years old, although more acutely unwell than women of the same age, were less likely to need emergency care than men over 60 years of age, particularly men over 70 years old. Men in the 60–69-year-old age group were least likely to need medical intervention but still presented as unwell.
The highest peak for men's calls was after GP surgeries have closed. Men of all ages believed the current model of healthcare delivery did not suit their needs, and some men deliberately seek after-hours care. 3
Factors that inhibit men from consulting a GP include inconvenient opening times, cost, inability to make appointments, not wanting to make a fuss, 14 and discomfort with the consultation process, particularly if the health concern is not physical. 2 These inhibiting factors may be eliminated with Healthline's service. Telephone health services may act as an important aid to “normalizing help seeking in men.” 21
Young men may be more amenable to telephone conversations, free advice, the “instant” and 24-h nature of the service, and the spontaneity allowed by a few moments on the telephone as opposed to a surgery visit. Telephones provide “virtual anonymity” and have no physical boundaries. This may be particularly important for younger men, 2 although White et al. 12 found anonymity was consistently voiced as important for all men. Telephone use obviates the need for a face-to-face consultation and may be seen as less threatening. Telenurses can assess symptoms without personal details if requested.
Men may resent the cost of a consultation if information alone was the outcome. 3 Thus, receiving free advice over a telephone may be more acceptable as a first approach for some men.
Wasting a health professional's time is a concern consistently identified as an important barrier to help-seeking. 2,12,14 The time-wasting “specter” is not completely eliminated with the telephone; however, a full waiting room cannot be seen. Thus men may be less anxious about time wasting. 21
Although there was no difference in call times for men and women, research is required to determine how gender, social, cultural ideas, and beliefs affect interactions between telenurses and male or female callers.
Although access to Healthline for Māori is as accessible as for non-Māori, 19,22 Māori and Pacific Island men underuse the service compared with women of those ethnicities. Men of these ethnic groups access primary health services less often and have higher “avoidable hospitalizations” than European men. 3,10 In 2003 15.1% of all callers self-identified as Māori, and 79% were “seeking symptom triage” compared with 66% for non-Māori.
Conclusions
This study has identified that the sample profile of men who called Healthline (a New Zealand primary care telephone triage and advice line) for health advice about themselves mirrors New Zealand and international research in face-to-face, primary care services—men access health services less than women, and they are more symptomatic overall than women when they do.
Healthline, however, holds a potential to address this inequality of health service utilization as it is a more anonymous service, addressing men's concern about appearing vulnerable when seeking assistance with their health, and it operates 24/7, addressing some men's concerns about putting their health ahead of their work. Furthermore, it provides affirmation of the need to seek face-to-face primary care services when needed, addressing men's reluctance to seek medical assistance in case it is unnecessary.
As such, in any development of initiatives to address the health inequities of men, Healthline should be considered as a key aspect.
This study now informs further research: our aim is to explore the effect of interventions encouraging men to use this primary care telephone triage service (Healthline) by public education covering (1) the perceived advantages of relative anonymity, (2) 24-h availability, and (3) affirmation, in appropriate cases, of their need to seek face-to-face consultation.
Footnotes
Acknowledgments
We thank the following individuals: Dr. Michael Rains, Principal Advisor, District Health Boards New Zealand; Dr. James Stanley, University of Otago; Andrew Parnell, Wellington City Council; Catherine Munford, Medibank Health Solutions NZ Ltd.; and Esther Greatbatch, formerly Medibank Health Solutions NZ Ltd.
Disclosure Statement
All authors are employed by Medibank New Zealand Ltd., which operates Healthline for the New Zealand Government's Ministry of Health.