
Abstract
Introduction
In recent years, telemedicine technology has been studied in various patient groups using different approaches and interventions and focusing on different outcomes. Studies on telemedicine in general have discovered that although the initial installation costs can be high, the services are billable, and the long-term cost savings to patients and providers in terms of time and travel are immense. 1 Telemedicine may in fact have a more profound impact on healthcare delivery in developing countries than in well-developed ones. 2
Since the 1990s, mobile telephones have become easily available and highly popular. The short message service (SMS), in which text messages are sent and received by mobile telephones, is increasingly being used for access to information. There are many reports of the use of SMS in medicine such as patient reminders, psychological support, chronic disease management, behavior modification, reporting of critical medical events or laboratory results, and even for surveys. 3 With the sophisticated Internet and computerized technology advances available today, reports on information technology-based pharmaceutical care models have been emerging. Preliminary usage of SMS has paved the way for a simple, fast, and efficient means in diabetes management whereby a cohort of diabetic patients had expressed good acceptance of such a system in communicating their diabetes data. 4
SMS technology has also been earlier implemented to improve patients' attendance at clinics. 3,5 Furthermore, SMS messages are suitable for direct patient communication, privacy, confidentiality, rapid information delivery, receipt of responses, and convenience. This technology also allows for the transmission of a substantial number of messages simultaneously, hence reducing labor expenditure. Technological difficulties were seldom encountered, and the technology was generally easy to use. 3
Despite the encouraging and supportive outcomes of SMS technology implementation in several chronic diseases, reports on its use in the epilepsy population have been virtually nonexistent. Therefore usage of SMS technology is also expected to be beneficial for improvising epilepsy educational programs and healthcare services, which could indirectly enhance the level of health-related quality of life (HRQoL) among epilepsy patients (people with epilepsy [PWE]). As such, we intended to develop and assess the feasibility and acceptability of using an SMS-based epilepsy educational program in a sample of the epilepsy population.
Subjects and Methods
This study was divided into five phases, starting from the development of an epilepsy education module, followed by the development of the mobile epilepsy educational system (MEES), study design and sample selection, data collection, and finally statistical analysis.
Phase 1: Development of Epilepsy Education Module
Adopted from several established epilepsy education programs, 6 –9 the module was developed with special focus on patients' needs. It aims to help patients achieve a better understanding of their disease, to gain more self-confidence, and to shoulder more responsibility, thus supporting patients to become experts in managing their own illness. This module, which incorporates epilepsy educational issues, was developed mostly with reference to the Modular Service Package Epilepsy (MOSES). 6,8 MOSES, as its name suggests, has a modular structure with nine comprehensive submodules covering the following topics: (1) living with epilepsy, (2) epidemiology, (3) basic knowledge, (4) diagnostics, (5) therapy, (6) self-control, (7) prognosis, (8) psychosocial aspects, and (9) network epilepsy. Whereas MOSES was comprehensive and intensive, our module, on the other hand, was rather brief and simple to suit the sociodemographic backgrounds of PWE, especially in East Coast Peninsular Malaysia, who are in general poorly educated. Moreover, no such epilepsy module has ever been developed in Malaysia, making this effort important to be practical and effective to suit patients' needs and necessities. Eleven submodules were included: (1) basic knowledge, (2) history and statistics, (3) living with epilepsy, (4) diagnosis, (5) treatment/therapy, (6) prognosis, (7) self-control, (8) myth and facts, (9) psychosocial aspects, (10) laws and acts, and (11) reference. The module was written in Malay and supplied to patients during baseline for a 3-month period, who were instructed to complete a submodule per week at home based on the schedule provided in the user manual. Details of the module are presented in Table 1.
Epilepsy Education Module
AEDs, antiepileptic drugs.
Phase 2: Development of The MEES
MEES is an SMS-based system that can be run on a computer to facilitate healthcare services by sending text messages to a patient's mobile telephone. The system was divided into three parts, including (1) epilepsy education module, (2) drug-taking reminder, and (3) clinic appointment reminder. Patient details such as full name, identification card number, and mobile telephone number were entered into the system during recruitment. Considered as an interactive education program, MEES allowed patients to send queries and comments regarding the services or their illness via SMS to the number 39111. The comments and queries were immediately attended to and replied to by the research assistants. However, if the queries needed expert opinions, patients were advised to seek medical consultation from the clinicians at their respective clinics. An introductory SMS was delivered a day after recruitment indicating the beginning of SMS. Table 2 shows the introductory SMS.
Introductory Short Message Service
SMS, short message service.
The first part of MEES (the epilepsy education module), which made up approximately 70% of the entire system, was designed specifically with the aim of enforcing knowledge among PWE. Consequently, conversion of the epilepsy education module into text messages has been carried out. The gist of each submodule was compressed into simple text messages and programmed into the MEES. Besides the introductory and closing text messages, two simple SMS texts generated from each submodule were automatically delivered to patients with a gap of 4 days. The text messages were scheduled to be consistently delivered at 10:00 a.m. each time for patients' convenience. Other than the automated SMS delivery, modification to the contents of the module was allowed if necessary. An example of a delivered SMS is given in Table 3.
Epilepsy Education Module
The second part of MEES incorporated the drug-taking reminder. Patient medication details containing drug name, dosage, frequency, time, and duration were entered into the system. The system then generated a drug-taking reminder according to the patients' prescribed medication. Inevitably, considering the different prescriptions for different patients, the drug-taking reminder has to be sent manually. In contrast to the automated epilepsy education, research assistants were required to personally click the “Send” button in the MEES in order for the drug-taking reminder to be delivered to the patients. They were reminded once every month about their medication. Within a 3-month period, three SMS texts were delivered to each patient. Editing and alteration of the drug-taking reminder were also permitted if necessary. An example of a drug-taking reminder is shown in Table 4.
Drug-Taking Reminder
The last part of MEES was the clinic appointment reminder. Patients' next clinic appointment details were obtained during recruitment and entered into the system. A reminder was generated and delivered to patients a day before the clinic appointment date. Similar to the drug-taking reminder, research assistants needed to manually send the clinic appointment reminder because of the different dates for each patient. This reminder highlighted details such as date, time, and venue of the clinic appointment. Editing of the details was also allowed if necessary. Table 5 gives an example.
Clinic Appointment Reminder
A closing SMS was delivered to patients after 3 months thanking them for their participation in the study and marking for the end of the services. The closing SMS is shown in Table 6.
Closing Short Message Service
Phase 3: Study Design and Sample Selection
This was a prospective randomized interventional study in epilepsy outpatients. Patients were recruited using convenient sampling from the Neurology Clinic of three general hospitals in East Coast Peninsular Malaysia: Hospital Tuanku Ampuan Afzan (Pahang), Hospital Raja Perempuan Zainab II (Kelantan), and Hospital Sultanah Nur Zahirah (Terengganu). Patients were included if they were existing epilepsy patients who had been on regular treatment, 18 years old and above, able to either write, read, or understand and communicate in the Malay or English language, and capable of completing questionnaires (written or verbal), possessed a mobile telephone (and active users), and had provided written consent for participation. The study was approved by the Medical Research and Ethics Committee of the Ministry of Health, Malaysia [protocol reference number NMRR-10-359-5640/ (2) dlm. KKM/NIHSEC/08/0804/P10-158]. Once the ethical approval was obtained, with the permission from hospital authorities, research assistants reviewed the epilepsy patients' medical record a week before data collection for screening and identification purposes of the potential participants.
A feasibility assessment was conducted before data collection. A group of 100 patients from each hospital was randomly selected to estimate the percentage of mobile telephone ownership among PWE. Other than that, the total cost of SMS delivery to patients was also calculated.
Phase 4: Data Collection Procedure
The recruitment began in December 2010 and was completed in December 2011. A hospital coordinator was identified and briefly trained to help with patient identification and medical record data collection prior to the clinic day. Data were collected on the epilepsy clinic day itself for the patients' convenience. On the agreed meeting day, the research assistants approached, explained, and invited potential patients who met all the inclusion criteria to participate in the study. An information sheet was given to enhance their understanding on the nature of the study as well as to clarify the particulars needed and what was required from their participation. The numbers to call in case of doubts and queries were also provided. Once they had agreed, participants signed a written consent form before proceeding to be registered in the MEES. Next they were supplied with a printed epilepsy education module and a mobile telephone top-up card initially worth MYR 5. The SMS texts were delivered to patients' mobile telephones for a 3-month period. An introductory SMS was sent to the patients the next day indicating the commencement of the MEES services. After 3 months, patients were contacted via telephone by the research assistants for a follow-up session at the same clinic. During the session patients were requested to complete the feedback form assessing the acceptability of the MEES, including perceptions of the general MEES services and its epilepsy education module, drug-taking reminder, and clinic appointment reminder on open-ended questions. We examined all the qualitative comments and opinions and then categorized them into either “positive” or “negative” remarks.
Phase 5: Statistical Analysis
Data were analyzed using the Statistical Package for Social Science (SPSS) version 16 (SPSS, Inc., Chicago, IL). The Shapiro–Wilk statistics for normality was determined because of the small sample size (less than 100), and results indicated that our sample did not satisfy normal distribution. Subsequently, the chi-squared test for goodness of fit was used to test homogeneity of the categorical variables. Besides that, descriptive statistics were used to calculate median and range for all continuous variables and frequencies and percentages for all categorical demographic variables.
Results
Recruitment of Participants
In total, 51 patients were enrolled in the study with a median age of 25.0 years, ranging from 18.0 to 72.0 years. The number of female participants was slightly higher than that of males (51.0%). Most of the participants were Malay (92.2%). More than half were single, and 84.3% of them were living with family. About 70.6% possessed an education level of equal to or less than SPM/Cambridge O-level equivalent, 25.5% were supportive workers, and 58.8% were earning monthly income of ≤MYR 500.0/ USD 158.5. Details are presented in Table 7.
Sociodemographic Background (n=51)
Chi-squared test for goodness of fit, p<0.05 was significant.
Feasibility of The MEES: Accessibility, Cost, and Acceptability
Accessibility of mobile telephones
As previously mentioned, we randomly selected 100 epilepsy patients from each hospital to briefly gauge PWE's accessibility toward mobile telephones. From a total number of 300 patients, it was found that 85.7% possessed at least one mobile telephone (Fig. 1).
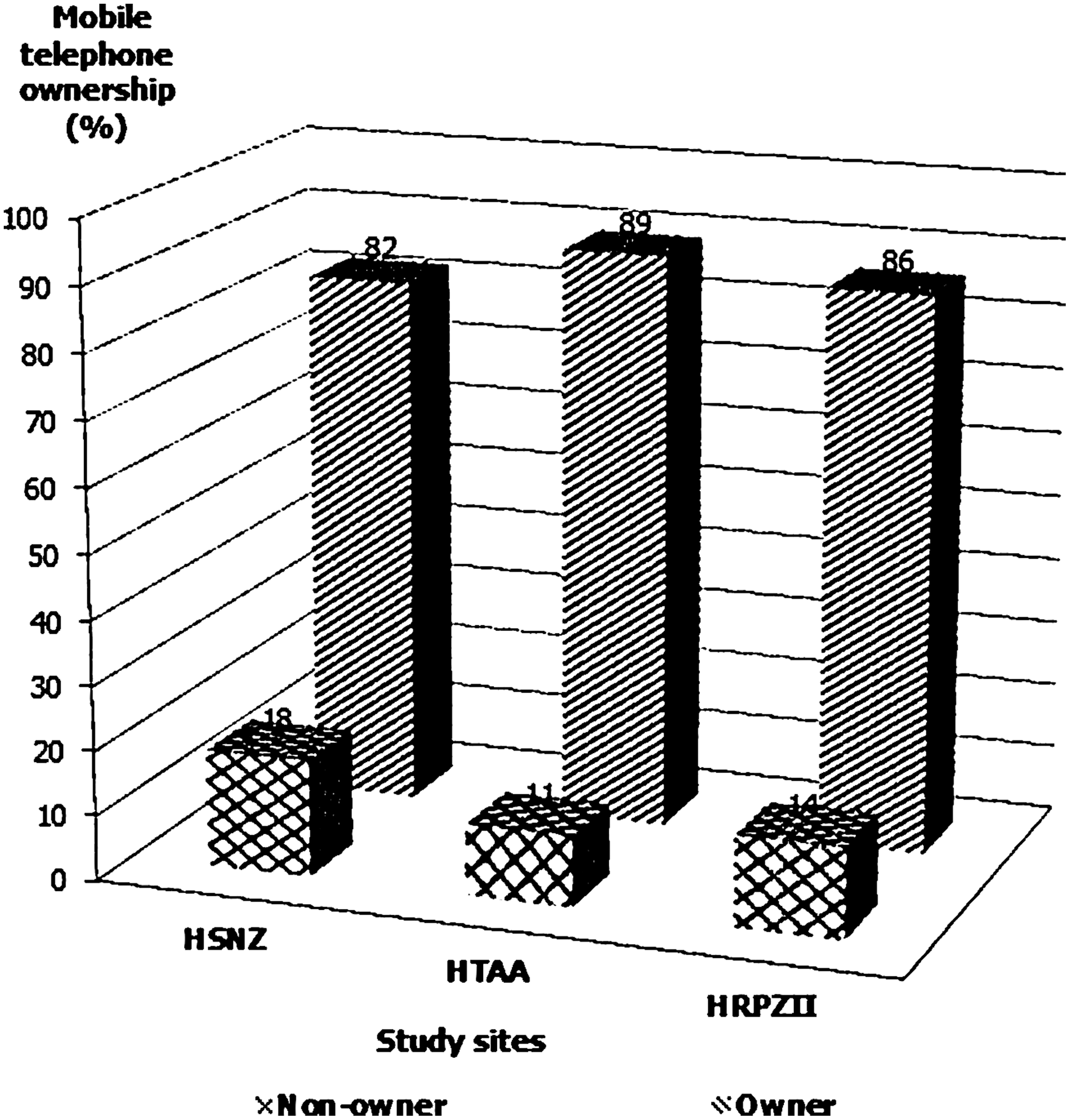
Mobile telephone ownership among people with epilepsy in Malaysia. HSNZ, Hospital Sultanah Nur Zahirah, Kuala Terenggamu; HTAA, Hospital Tuanku Ampuan Afzan, Kuantan; HRPZII, Hospital Raja Perempuan Zainab (II), Kota Bahru.
Cost of SMS delivery
It was important for the MEES to be cost-effective to both patients and healthcare providers. Although no charges were applied to patients, the total cost of SMS delivery charged to the provider, on the other hand, was rather inexpensive. After calculation, the epilepsy education module required a total of 24 SMS texts, and the drug-taking reminder required another three SMS texts (one SMS per month), whereas the clinic appointment reminder needed only one SMS. Therefore, the total number of SMS received by each patient was 28, and the minimal cost calculated was about MYR 0.11 per SMS delivery. Hence, the total SMS delivery cost for each patient was approximately MYR 3.08/USD 0.98 for the entire educational package, which was considered very affordable to many healthcare institutions. Nonetheless, the hidden costs involving its initial development and installation of the system were also included. Additional details are given in Table 8.
Description of Short Message Service Delivery Costing Set-Up
SMS, short message service.
Acceptability of the MEES: general perception of the MEES services and its epilepsy education module, drug-taking reminder, and clinic appointment reminder
Patients were asked regarding their opinions toward the information obtained from MEES. Most found it to be very useful (50.0%), another 24.0% said it was quite useful, and 18.0% claimed it was useful, whereas 8.0% agreed that it has been of “little use.” Overall, participants' acceptance toward MEES was very promising. Subsequent analysis based on sociodemographic characteristics determined that the proportion of patients who possessed a higher education level, earned a higher income, and stayed in urban areas exhibited more favorable perception toward the system compared with their counterparts (Fig. 2). The epilepsy education through SMS was highly acceptable by the patients, of whom almost 94.0% provided positive and favorable opinions. Besides that, the drug-taking reminder and clinic appointment via SMS have also received positive comments at 90.0% and 88.0%, respectively. It was also encouragingly reported that 88.2% of the participants would recommend MEES to other PWEs (Table 9).
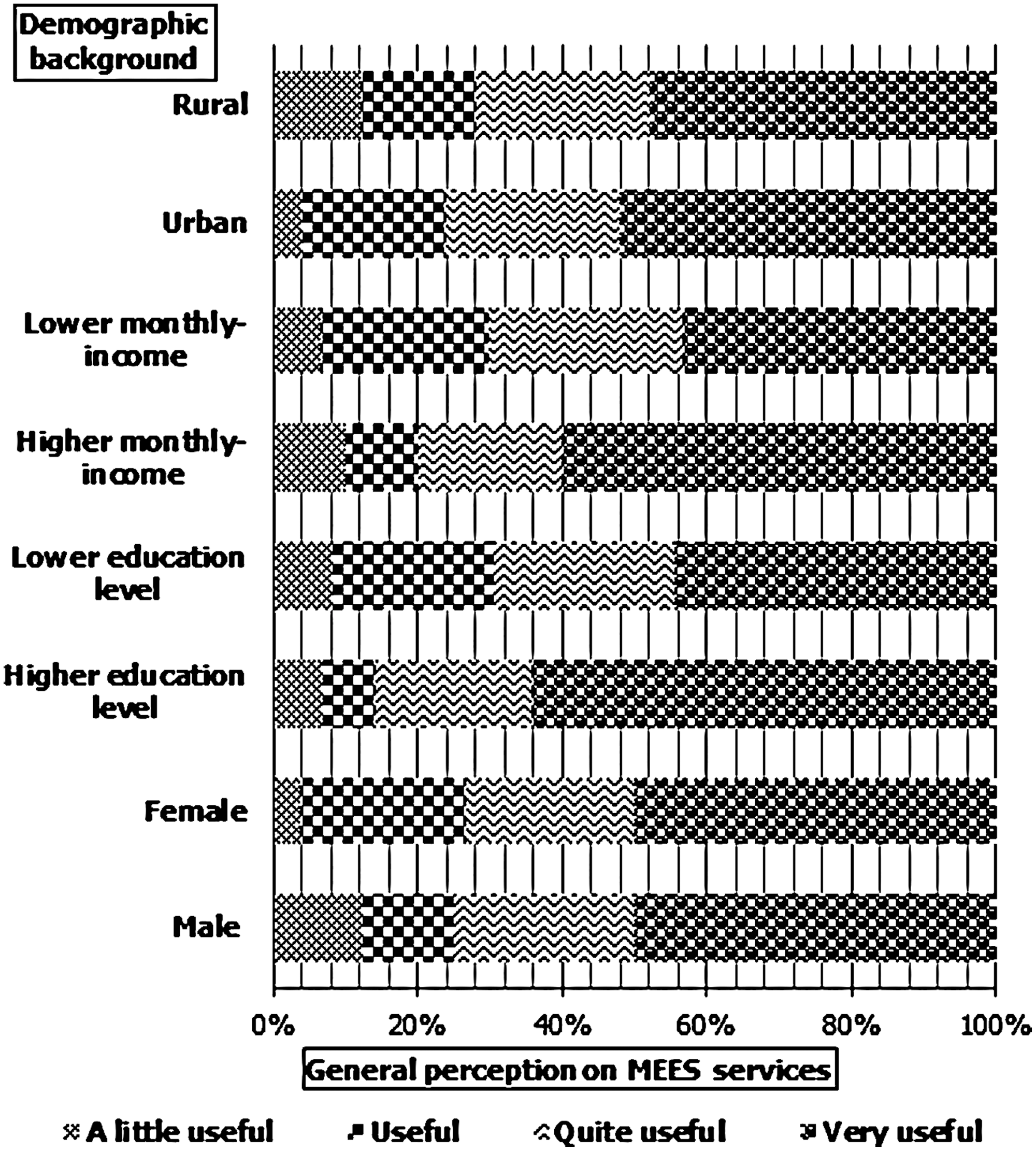
General perception of the mobile epilepsy educational system (MEES) based on sociodemographic background.
Feedback on Mobile Epilepsy Educational System
MEES, mobile epilepsy educational system.
Discussion
It is known that most adult patients with epilepsy often know little about their disorder, medication, treatment options, and psychosocial consequences, despite the enormous amount of information available. 10 Today, Internet sites, radio and television, dialogue with physicians and lay organizations, and clinic-recommended books and leaflets are the main sources of information for patients and their families. However, many of the current, easily accessed epilepsy Web sites do not comply with accepted standards for health Web sites, and healthcare professionals are not able to provide repetitive counseling and the necessary instructions to address epilepsy care adequately. Consequently, educational programs are considered extremely important. SMS facilities on mobile telephones were introduced in the early 1990s and now represent one of the most widely used methods of communication. 11 Considering all these gadgets as potential new technologies for effective health education, our study intended to introduce an SMS-based education program and assess its feasibility and acceptability as an alternative to the current education programs, especially among PWE and their families.
Our patients were generally young, unmarried, and with minimal education and were earning low income. These attributes, unfortunately, were the familiar characteristics of PWE in Malaysia. 12 –14 These “undesirable traits” have been passed down for centuries, and PWE have been highly stigmatized. 15,16 Even today, they have to face a number of limitations in their daily lives due to these attributes. 15 It has been widely proposed that knowledge empowerment through epilepsy education could be effective in demystifying stigma, thus indirectly cultivating good perceptions and favorable attitudes toward PWE. 15
With reference to the feasibility assessment, data from the current study indicated that the MEES was highly feasible to both patients and the provider. The percentage of mobile telephone ownership among PWE was unsurprisingly high. This finding could probably be due to the increasing number of mobile telephone users in Malaysia for the past few years. In the year of 2011, the percentage of mobile telephone usage in Malaysia stood at 106.0% of the population. 17 Consequently, as mobile telephone ownership continues to increase rapidly in many countries worldwide, the potential of using SMS to increase the effectiveness and efficiency in healthcare delivery seems to be escalating as well. 11
Budget and cost are pertinent matters for any healthcare providers. Given that it cost only MYR 0.11 per SMS with a total expenditure of MYR 3.08 (USD 0.98) per patient for a 3-month period, the MEES could be considered as economically affordable. However, the hidden costs involving the development and installation of the system in the beginning should be taken into consideration. These costs are generally high, which require a large amount of money to be invested in the early phase of research. In the long run, however, SMS messaging software allows large batches of tailored text messages to be sent at once, minimizing labor costs. All mobile telephones have the ability to accept these messages. SMS reminders required minimal investment in information technology infrastructure, given that the information technology software for sending automated SMS could also be integrated with existing electronic patient health records and hospital administrative database systems. 18 Once the system was in place, the cost of running the service increased very little even as the number of SMS reminders went up. In addition, because the messages were automated, there is no requirement for staff training, hence allowing for a time-, labor-, and cost-efficient system. 19
According to the outcomes on acceptability, other than being feasible, our intervention was also reported to be highly acceptable among patients who agreed that it has the potential to emerge as an effective educational program for epilepsy. Most patients have given their approval and would recommend it to other patients. Comments such as “the text messages were very simple, brief and easy to understand,” “the texts on drug-taking reminder alerted me about my medication,” and “the clinic appointment reminder was very helpful” were given by the participants, suggesting supportive evidence of MEES's acceptability.
It is encouraging that our findings have demonstrated PWE's favorable reception toward epilepsy education via mobile telephone text messages, hence adding to the growing potential for SMS-based educational programs in epilepsy. Even though this emerging technology has many advantages, little or almost none has been published on the use of SMS for healthcare education. A PubMed search identified at least 18 articles that described the use of SMS as an appointment reminder 20,21 and drug-taking reminder, 3 but none reported the use of SMS as an educational tool for epilepsy sufferers so far. Even within comprehensive therapeutic management of chronic diseases such as epilepsy, educational programs for patients are considered to be extremely important. It is unmistakable that more SMS-based interventions for epilepsy education could be advantageous for health outcomes in the long run.
The medication reminder via SMS was also well received among PWE. This result was certainly encouraging considering that medication nonadherence among PWE remains a significant challenge, which could lead to increased risks of seizures, hospitalizations, and higher treatment costs, especially for patients out of hospitals. 3 According to Kripalani et al., 22 between 20% and 50% of patients do not adhere to therapy, and medication compliance in patients who have left the hospital is particularly unsatisfactory. This is undoubtedly alarming because epilepsy treatments require constant patient supervision and strict adherence to the daily drug regimen. Pertinent to these issues, our SMS reminder seemed to be very useful in facilitating drug-taking effectively and could possibly reduce the medication nonadherence rate among PWE.
Nonattendance at outpatient clinics is another obstacle for effective and efficient healthcare. 23 Various reasons for patients not attending the clinic have been reported, including patients' forgetfulness and confusion over the date, time, and location of the appointment. 23 Sending telemedicine-based appointment reminders from hospitals to patients represents a technological application that positively contributes to the healthcare process. Our result showed that patients were in favor of such an SMS clinic appointment reminder. Receiving an SMS reminder a day prior to the clinic appointment was considered helpful and handy. Moreover, sending SMS reminders has been proven to be a simple and cost-effective way to improve nonattendance at epilepsy outpatient clinics. 3 Studies have confirmed that sending appointment reminders in SMS text message format to the mobile telephones of patients or their carers is an efficient and effective means of improving attendance for outpatient clinic appointments. 5 This fact was further supported by another Malaysian study showing that text messaging, if implemented correctly, can be a cost-effective method to increase clinic attendance. 24
A few limitations of this study should be taken into consideration. Although we were able to identify whether SMS messages were successfully transmitted, we did not know whether they were received by the correct recipients. A major reason for omitting patient details from the message was the concern that the mobile telephone contact number might be incorrect or, if correct, it might not be the patient or carer who received the message. 5 Other authors have identified outdated telephone numbers as a problem for reminder studies. 25 Unfortunately, SMS text messages also possess some disadvantages as a means of communication with patients. For example, the use of this emerging technology places those who do not possess a mobile phone at a disadvantage. Even though the uptake of mobile telephone services in the general community in Malaysia is very high and rapidly increasing, 26 a proportion of patients still do not have access to this technology. Inevitably, because of the limited financial resources available to us, the drug-taking reminders could only be delivered once in a month, considering the priority on the epilepsy education module. Although we agree that this could be less effective in terms of improving medication adherence, the positive feedbacks obtained from the patients have directly reaffirmed their favorable perception and acceptance toward the services.
Conclusions
The findings of the present study highlighted the general positive feasibility and acceptability of the newly developed MEES among epilepsy patients, which signaled MEES's potential as an important education tool to be further explored and propagated in the future. Mobile telephone technology therefore holds a promising role in bringing health assessment, education, and other services closer to the patients. Future research should venture into the expansion of telemedicine technology not only for epilepsy but also for other areas of neurology.
Footnotes
Acknowledgments
We wish to thank the Director General of Health, Malaysia, for permission to publish this article and the hospital directors, heads of Neurology Department, and staff of the Sultanah Nur Zahirah, Tuanku Ampuan Afzan, and Raja Perempuan Zainab II Hospitals for their cooperation in ensuring the success of this study. Our gratitude also goes to the Dean of Faculty of Medicine and Health Sciences, Universiti Sultan Zainal Abidin, and all participants and their families for supporting our study. Our final appreciation is directed to the Centre of Research Management and Innovation of Universiti Sultan Zainal Abidin for its financial support [grant UDM/10/BR (029)].
Disclosure Statement
No competing financial interests exist.