
Abstract
Introduction
Parkinson's disease (PD) is characterized by tremor, rigidity, bradykinesia/akinesia, postural instability, and impaired gait (decreased velocity and stride length). 1 –4 These gait abnormalities place people with PD at high risk for falling. 5,6 Physical rehabilitation interventions are frequently prescribed to improve balance, mobility, strength, and activities of daily living. 7 –12 These interventions may be prescribed on an individual or group basis.
Computer-mediated virtual environment platforms have been used for motor rehabilitation for decades. Movements learned by people with disabilities in virtual environments transfer to real-world equivalent motor tasks in most cases and even generalize to other untrained tasks in some cases. 13 The Nintendo® Wii™ system (Nintendo of America, Redmond, WA) offers a low-cost alternative to high-end head-mounted virtual environment systems. Players interact with the Wii system by making normal motions (i.e., swinging an arm) that control the movements of virtual objects on the screen. The input device, the Wiimote, detects acceleration in three dimensions as well as rotations about the two axes perpendicular to the force of gravity. The rapid response of the system provides a smooth, easy-to-learn, human–computer interface that is much less expensive than high-end virtual environment systems.
There is increasing interest in the use of games within the health field. One of the benefits of games is that they can adapt to the patient's actions to maintain a high level of engagement. Adaptive computer games evolve as players learn new skills by increasing the difficulty of challenges, thereby allowing the player to stay within an “area of maximal engagement,” which is similar to Vygotsky's “zone of proximal development.” 14,15 In educational situations, the zone of proximal development is where maximum learning occurs. In physical training or rehabilitation situations, being in the “zone” fosters continued and mindful effort on the training goals.
Developing games for people with disabilities involves unique design challenges because the “area of maximal engagement” for this type of player is likely to be different from that of an unaffected person. Game developers use a combination of usability testing and “tuning” approaches when targeting players with disabilities to properly calibrate the game difficulty to the players' abilities. 16 –18 Observation and rapid, iterative changes are essential for success.
Studies in patients with stroke, 19 –21 traumatic brain injury, 22,23 cerebral palsy, 24 and PD 25,26 have shown successful motor rehabilitation using interactive technology. Esculier et al. 26 reported high functioning subjects with PD improved their balance, mobility, and functional ability playing preselected off-the-shelf Wii games. However, many commercially available games are not suitable for people with marked disability who require specifically targeted exercises and routines to achieve therapeutic goals. Neurorehabilitation usability studies have found that off-the-shelf games may actually provide negative auditory and visual feedback because patients are not fast enough or efficient enough to perform the movements required to successfully play the game. 27,28 Because of these user limitations, researchers are now developing games specifically targeted for rehabilitation in particular populations.
After successfully offering a 1-hour group class for gait and balance training for people with PD 8 at the University of California, San Francisco (UCSF), training program developers G.A.D. and M.M. sought to broaden access by providing a home-based program. In late 2007, Red Hill Studios (RHS), a developer of educational and health games, suggested building a set of games that would utilize the recently released Nintendo Wii motion-sensing system to detect patients' movements as they performed the training exercises. RHS and the UCSF clinicians partnered to obtain National Institutes of Health funding through the Small Business Technology Transfer grant program. The goal of this Phase I study was to test the feasibility of creating a comprehensive computer game-based training program, demonstrate safety for clinic and home use, and test usability and appeal with end users. The team also sought to develop a remote data capture transmission system with the ultimate goal of enabling healthcare professionals to remotely prescribe personalized gaming regimens and monitor progress.
The specific aims of the study were to demonstrate: 1. Technical feasibility of adapting the classroom training program to a computer-based platform 2. Safety of the proposed program for clinic and in-home use 3. Ease of use of the proposed program and 4. Appeal of the proposed program.
Subjects and Methods
Samples and Settings
The innovative nature of the program required extensive iterative development with several rounds of evaluation: 1. The operational evaluation used a small sample (n=3) to gather initial data about the user interface and identify therapeutic physical movements to be incorporated into the computer-based games and took place at the UCSF Physical Therapy Health and Wellness Center to enable the use of a suspended safety harness. 2. The preliminary evaluation occurred in two stages (Stage 1, n=3; Stage 2, n=4), again at the UCSF Physical Therapy Health and Wellness Center. Subjects played the prototype games, and the clinical and design teams in conjunction with the subjects identified bugs and difficulties and assessed potential safety issues. 3. In the in-home evaluation, we evaluated the final version of the Phase I prototype games that had been redesigned based on the findings of the preliminary evaluation, with subjects (n=10) in their homes.
In total, 20 subjects were enrolled in this study. Inclusion criteria were consistent with the guidelines for idiopathic PD, 29,30 and subjects met criteria for Hoehn and Yahr disease Stage 1 (unilateral disease) to 3 (bilateral disease, physically independent). 31 Exclusion criteria included persons with features of atypical PD 30 or significant other neurologic, orthopedic, or cardiac problems, cognitive impairment as evidenced by five or more errors on the Mini Mental State Examination, 32 or visual or hearing impairments serious enough to interfere with the ability to interact with the computer-based training program. All subjects consented, and the study was approved by the UCSF Committee on Human Research. At all evaluations, subjects were tested 1–2 h after taking their routine dose of anti-parkinsonian medication to facilitate being in the “on” state.
Measurements/Instruments
Demographics and functional status
Demographic, general health information, and functional status ratings on the Unified Parkinson's Disease Rating Scale (Parts 2 and 3) 31 and the Hoehn and Yahr disease staging 31 were collected on all subjects to characterize the sample.
Perception of exertion
To determine subjective assessment of physical activity intensity during game play, the Borg Rating of Perceived Exertion Scale 33 was administered upon completion of the gaming session.
Experience feedback survey
Table 1 gives the survey used.
Experience Feedback Survey
Questions were developed for each stage of the testing.
Computer platform
The PC-based games were developed using a computer programming platform, Unity 3D (Unity Technologies, San Francisco), and incorporated the Nintendo Wiimote controller, which detects acceleration in three dimensions (x,y,z) through the use of low-cost accelerometers. The PC-based platform provided greater flexibility in developing the prototype games (as opposed to the closed system of the Nintendo Wii console). In addition, the computer programming environment allowed us to capture engineering data necessary to properly tune the system for the intended audience. Data from the Wiimote were acquired through the computer's Bluetooth® (Bluetooth SIG, Kirkland, WA) receiver and sent to the Unity real-time three-dimensional programming environment. The short transmission and response time (tenths of a second) between the Wiimote and the computer minimized signal latency creates a fluid interface in which the user quickly learns to act through the interface instead of acting with the interface. 34 This allows the user to focus on how he or she is manipulating the virtual objects on the screen, as opposed to how to operate the interface device (Wiimote).
Procedures
There was close collaboration between the RHS and UCSF teams during development of the game prototypes. The steps in the process of translating the classroom training to a gaming format are depicted in the flowchart given in Figure 1. The operational and preliminary evaluation feedback enabled several rounds of iterative game redesign (Figs. 2 and 3). First, the clinical team (UCSF) identified a set of five therapeutic movements that could be the focus of potential games. The design team (RHS) defined a set of “game gestures” designed to elicit the therapeutic movements selected by the clinical team. The design team narrowed the number of game gestures to three possible options (because of budget constraints of the Small Business Technology Transfer Phase I grant) and developed algorithms to identify the game gestures based on the data provided by the Wiimote. For example, in one game, the game gesture consisted of the subject standing up and then sitting down. When the game program detected that the game gesture had been successfully performed, it provided feedback in the form of a game action. For the standing up/sitting down gesture, the game action involved propelling a railroad handcar down the track. Given the exploratory nature of this research, we took advantage of production efficiencies to develop rough prototypes for two other games. The two other games provided different technical challenges, which allowed us to expand our knowledge of gesture-based games. For the second game, trunk rotation movement was developed into a zoetrope game, where a movie would play at the correct speed if the rotation was done at optimal speed and radius. For the third game, diagonal reach across midline movement was developed into a clothes toss game (Table 2).
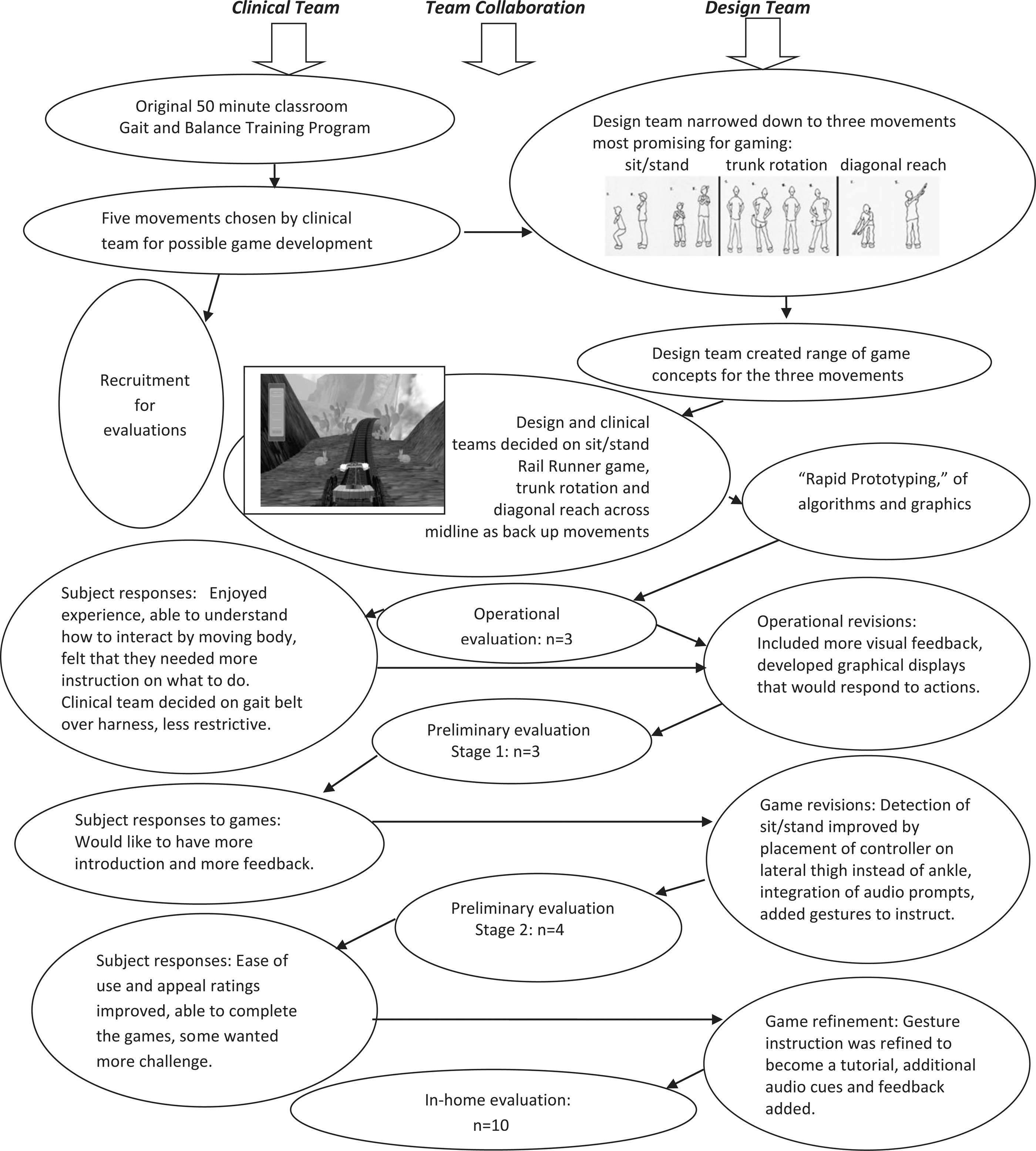
Workflow chart showing the iterative design/evaluate/revise/re-evaluate process.

Operational evaluation.
Preliminary evaluation tutorial screen shots. “Gesture screens” were originally developed for the operational evaluation. With feedback from subjects, the screen shots were expanded, and audio cues were added for better instruction and guidance.
Game Descriptions
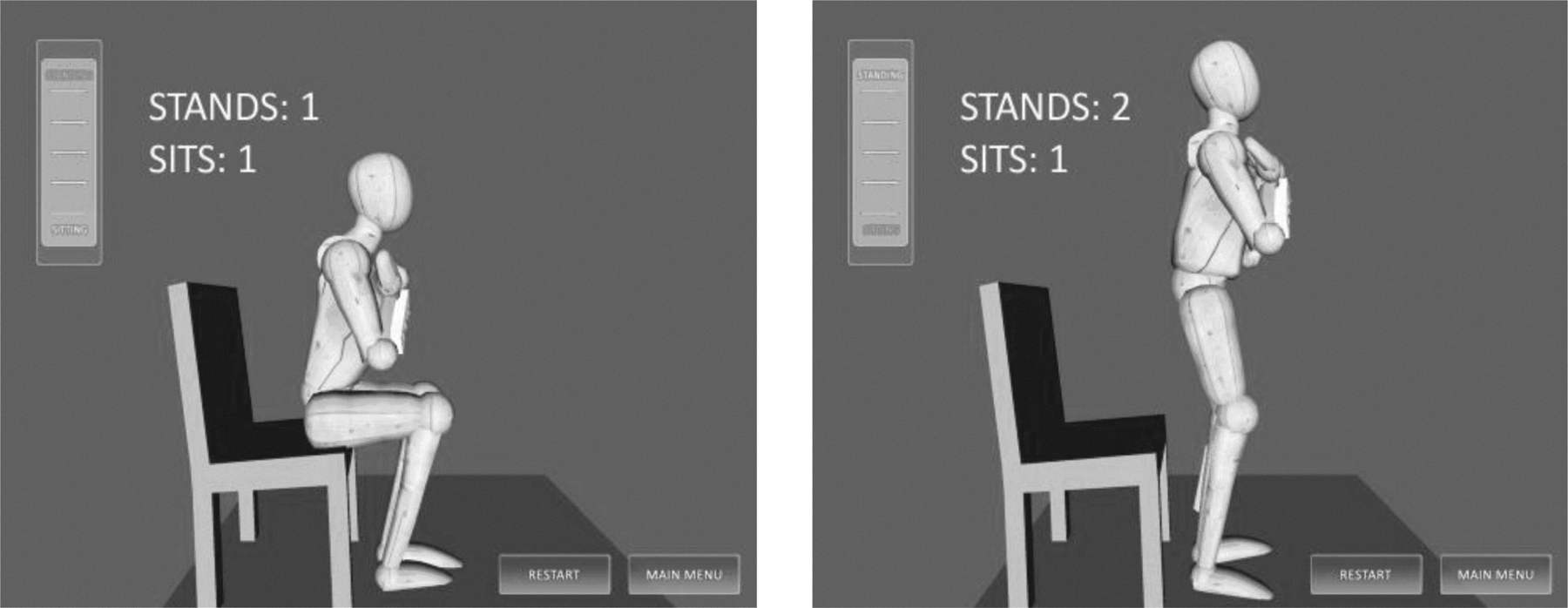
For the in-home evaluations, subjects were outfitted with two Wiimotes: one on the wrist and the other on the opposing thigh using polychloroprene (Neoprene; DuPont™, Wilmington, DE) straps and Velcro® (Velcro USA, Manchester, NH). Clinical team spotters were situated on either side of the subject for safety. The subjects were oriented to the equipment and to study procedures and were encouraged to ask questions along the way. Researchers reinforced the fact we were testing the equipment, not the subject. Subjects were prompted with the tutorial start screen that explained the movement verbally and visually with a simple jointed figure as their avatar (Fig. 4). Subjects practiced the game movements while watching an on-screen avatar that mirrored their movements, providing real-time feedback on performance. Subjects also received audio feedback that provided suggestions for improvement and encouragement. If subjects were having difficulty achieving the correct movement, a clinical team member demonstrated and guided their movement until the desired movement was achieved. After successfully completing the tutorial, the subject then played the “Rail Runner” prototype game several times. A design team member monitored the subject's level of engagement and/or frustration and made adjustments to the speed and difficulty of the game manually on the computer. The same process was carried out for the rough tutorials and prototypes for the other two “back up” game concepts. Rest breaks were given as desired by subjects or if the clinical team perceived the subject was experiencing fatigue. After completion of game play, subjects rated their perceived exertion and answered questions regarding their subjective sense of ease of use and appeal of the games.
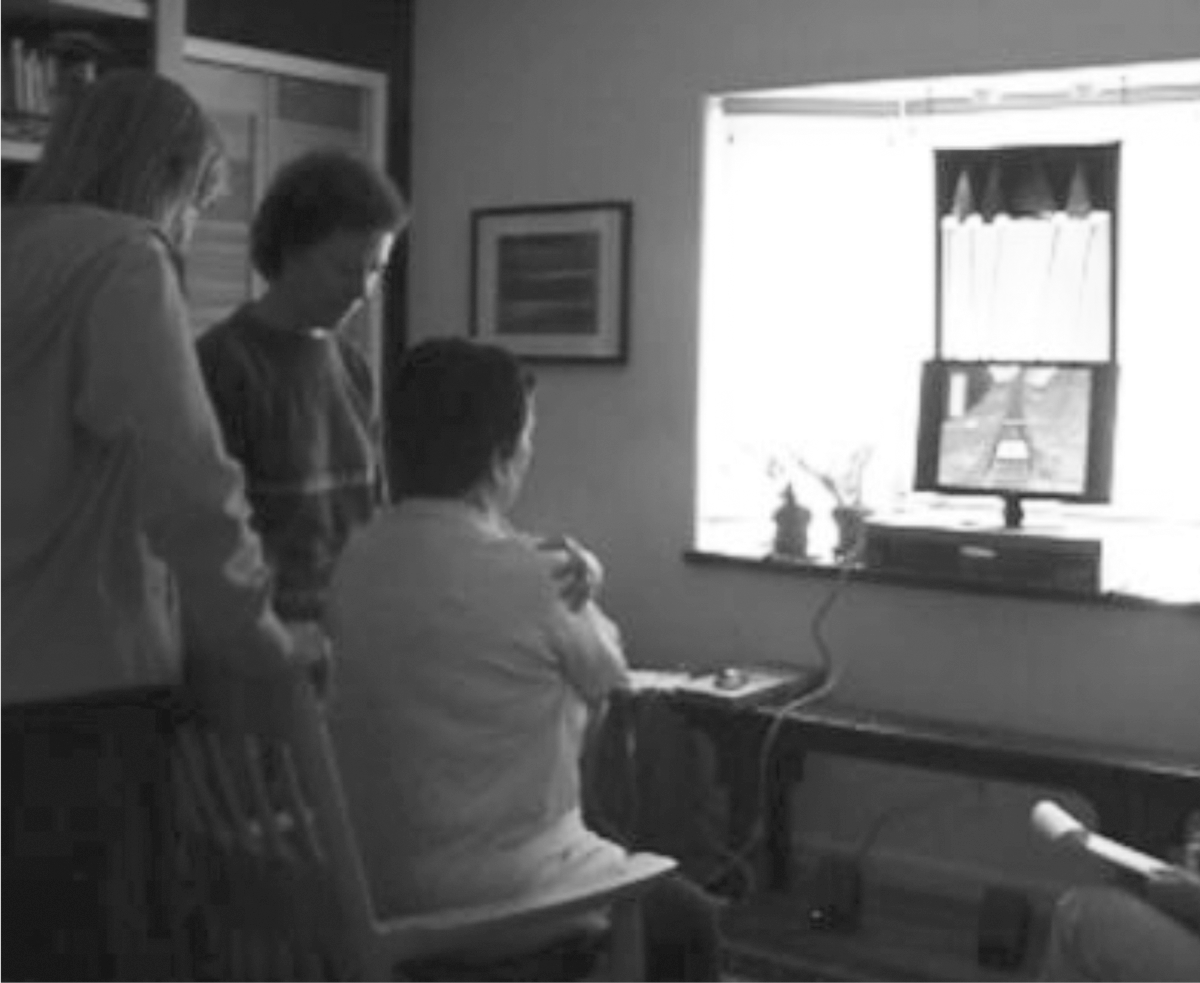
In-home evaluation, using a well-lighted room with a sturdy straight-backed chair for the “Rail Runner” game.
Results
Sample characteristics are described in Table 3. Operational and preliminary testing subject feedback results and the game revisions are described in Table 4 and depicted in Figures 1 and 2 . During the in-home testing, the games performed without technical bugs or flaws during the in-home evaluations, and there were no falls or injuries. After subjects played the “Rail Runner” game, their mean ease-of-use rating score was 3.6 (standard deviation [SD] 1.3) (from 1=very hard to use to 5=very easy to use), and mean appeal score was 3.9 (SD 1.1) (from 1=did not like to 5=liked very much). After subjects played the “back up” game “Virtual Zoetrope,” their mean rating score for ease of use was 2.7 (SD 1.6) (from 1=very hard to use to 5=very easy to use), and mean appeal score was 2.8 (SD 1.6) (from 1=did not like to 5=liked very much). After subjects played the less developed “back up” game “Musical Garments,” their mean rating score for ease of use was 3.6 (SD 0.7) (from 1=very hard to use to 5=very easy to use), and mean appeal score was 3.1 (SD 1.2) (from 1=did not like to 5=liked very much).
Demographic and Functional Characteristics of the Sample
Diagnosis is how many years have lapsed since the subject has been diagnosed with PD.
H&Y is the Hoehn and Yahr score, on a scale of 1–5, with a higher number reflecting more disability.
F, female; M, male.
Early Testing Design Iterations Based on Subject and Team Feedback
Discussion
The technical performance of the games was high, with no technical flaws occurring during the final prototype evaluation. In the process of “getting under the hood” of the Wiimote system, we identified two key limitations of the device. First, bias error and sampling noise from the accelerometers quickly produced unacceptably large error values for derived velocity and position (due to single and double integration of force data). Gesture recognition software typically used for the Wiimote (e.g., AILive) relies on recognizing sequences of relatively large, short-duration impulses in the acceleration signature, which are suitable for detecting vigorous gestures such as shaking or “batting.” However, the motions of interest for this project were generally slower motions, lacking these large, short-duration impulses. Second, although the accelerometers produce relatively accurate limb orientation estimations when used as three-axis “tilt meters,” they are unable on their own to discriminate rotation purely around the vertical axis. This makes them less reliable in detecting motions such as trunk rotation. We overcame these limitations by focusing on the relatively accurate ability to determine limb orientation combined with the constraints of human body mechanics and developed specific criteria to determine when game gestures were successfully completed. For example, using the accelerometer as a tilt meter (deviations from vertical force of gravity), we calculated the deflection of the subject's trunk and thigh from vertical and used the combined signature of these values as they changed over time to detect the “standing up” and “sitting down” movements.
The limitations of systems based solely on accelerometers will be avoided moving forward by replacing the Wiimote with an enhanced motion-sensing system that uses gyroscopes and a digital magnetometer to augment the three accelerometers. This modification will allow far superior estimation of limb orientation in three-dimensional space and thus a greater breadth of detectable gestures.
There were no falls or safety issues encountered in any of the three Phase I evaluations. This can be attributed to the close collaboration between UCSF and RHS that produced games suitable for the target audience that did not foster dangerous situations or elicit overexertion. It should be noted, however, that the UCSF team had to closely monitor several subjects while they were playing to ensure safety. Thus, safety strategies and close monitoring will be key components in the subsequent phases of game testing.
The prototype game was challenging for subjects to play because it required them to interact with a computer in a totally new way. The fact that subjects were able to play the prototype game and rated it highly is encouraging. However, each new game will present new user interface challenges because this novel interface requires subjects to physically interact with the game (as opposed to a simple Web activity).
The collaborative team's experience in designing and developing the “Rail Runner” game as well as the “back up” games “Virtual Zoetrope” and “Musical Garments” reinforced the need to follow a highly iterative design/evaluate/revise/re-evaluate process moving forward as we design new games. The development of the two “back up” games gave us the opportunity to test a broader range of motions than would have been possible with just one game and anticipate potential technical issues in new game designs. For example, the hip-rotation game involved a continuous movement (rotating the hips) as opposed to a sequence of discrete movements with specific end points as in the “Rail Runner” game (sit, stand, sit, etc.). Some of the subjects decreased the amplitude of rotation over time, finally reaching a point where the system did not recognize the motion. Given that progressive decrement in amplitude with repetitive motion is common in people with PD, this issue is likely to emerge with any game that does not have specific end points. Our plan is to ensure that the system continues to recognize the movements while also encouraging subjects to exaggerate their motions to achieve therapeutic benefit.
Overall, subjects were intrigued by and enthusiastic about the possibility of using games to perform gait and balance training. The preliminary nature of the Phase I prototype, in terms of graphics, audio, and supporting material, may have affected the subjects' rating of appeal in the final in-home evaluation. Several subjects commented specifically that they would have liked more tutorial/instructional material about the games, which supports the findings of Robertson 35 and the needs of “silver gamers.” Based on these results, we will increase resources for instructional support moving forward.
Instructions were presented to the subjects as both audio prompts and on-screen text instructions. In some cases, the text was not large enough to be read clearly by all subjects. We will establish a minimum text size (number of inches on screen) and dynamically adjust the size of the type based on the subject's system.
One of the issues with the “Virtual Zoetrope” game was that some of the subjects did not know what a zoetrope was (an old-fashioned mechanical device that rotates to display a sequence of images as a movie). The project team assumed, incorrectly, that this device would be familiar to subjects, but for some subjects it clearly was not, and this impacted their performance. Moving forward, we will review potential game concepts with typical end users at an early stage in development.
Summary and Conclusions
This study demonstrated the feasibility of using computer-based games to provide gait and balance training to people with PD. As could be expected when exploring innovative uses of technology, the study involved a fair amount of experimentation and refinement. The ability of the collaborative team of RHS and UCSF to respond to interim challenges and find creative solutions bodes well for future development. The design and production capabilities of the collaborative team were also demonstrated by the “extra” development of two additional prototype games. The inclusion of these games in the Phase I program allowed us to gain valuable information that will greatly inform the Phase II study. Finally, the moderately high variability in the sample population in terms of game appeal, desired difficulty level, and personal abilities has directly informed the design of future games. We will increase the number of games and increase the difficulty range to customize the game challenge to individual abilities.
Footnotes
Disclosure Statement
R.H. and C.B. are employees of Red Hill Studios. G.A.D., J.M., and M.M. declare no competing financial interests exist.