
Abstract
Introduction
Telehomecare, in other words, home remote monitoring, has been shown to benefit patients with chronic diseases in many research trials. 1 Of these, patients with chronic obstructive pulmonary diseases (COPD), diabetes mellitus, and congestive heart failure have been received the most attention. 2 In these cases, biomedical data are remotely collected and transferred via the Internet to a central hosting service. 3 It is expected that this technology will be commonly used in hospitals and for home monitoring in the next few years. 4
In addition, there are many studies related to decision support applications in telehomecare. Related studies can be divided into two main and three subcategories. These are online and offline studies as main categories and as subcategories adaptive computer-based, rule-based, and statistical-based studies. 5 –8
In the literature, phone-based studies facilitate biomedical data transfer in real time to increase the mobility of patient monitoring. They also make critical care easy before the patient is on the ambulance. In the study of Tachakra et al., 9 someone who lives in the Highlands of Scotland a hundred miles from the nearest hospital can be given a routine check-up by mobile phone; the system can also be used by emergency rescue teams and in sports science to take measurements of athletes while they are training. In addition, Bluetooth® (Bluetooth SIG, Kirkland, WA), Zigbee, wireless local area network, third-generation, general packet radio service, and radio frequency technologies are commonly used in data transfer. In these studies, different policy engine types evaluate the data, and the results will be accessible almost anytime and anywhere through a mobile device. 9 –14
According to the new estimates of World Health Organization for 2030, COPD is predicted to become the third leading cause of death. 15 Studies related to remote tracking of patients and the frequent occurrence of mistakes in patient care plans show that a new approach is necessary. 16 Because of these reasons, we have developed a novel mobile adaptive tracking system (MATS).
This article is organized in five sections. In the first section, MATS is presented. The materials and methods of the system are presented in the second section. In the third section, the results are evaluated. After that, discussion about the system is presented. Finally, in the fifth section, the conclusion and recommendation of the issue of MATS for chronic pulmonary patients in their home environment are presented.
Mats
In this article, designing and testing of the system with chronic pulmonary patients in their home environment are described. The system, shown in Figure 1, consists of portable spirometry, a smartphone, extensible markup language (XML) Web services, a firewall, a Web server, and classical and mobile device-compatible Web pages. After the acquisition of pulmonary function test (PFT) data with the Bluetooth virtual serial port protocol, data are processed in real time on a smartphone with a back propagation artificial neural network (BP-ANN) classification algorithm. The results are sent through short message service (SMS), and all data including patient information are stored in the Web server database. In addition to the generated and measured data, additional information related to the chronic pulmonary diseases can be accessed on Web pages.
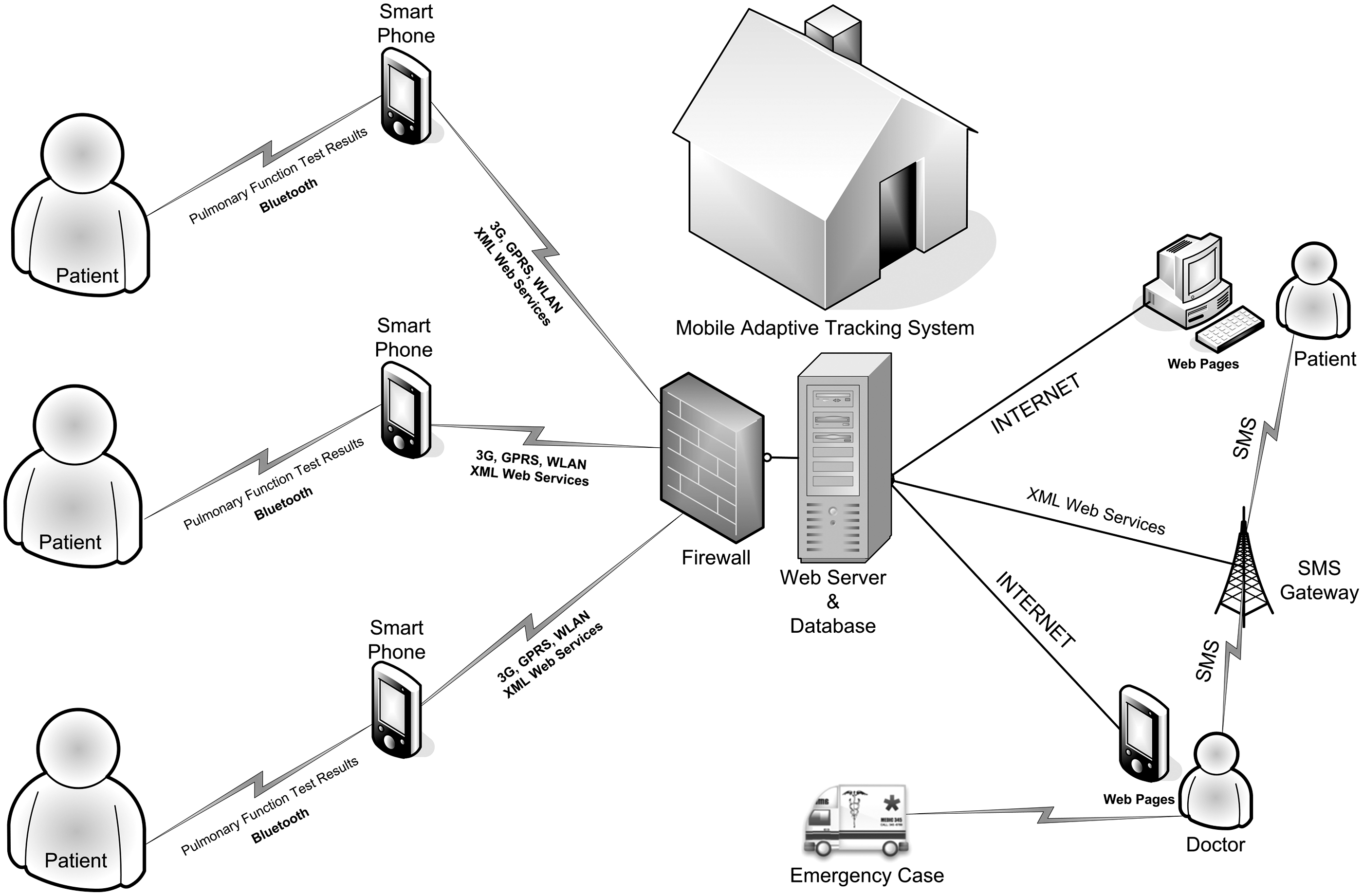
Mobile Adaptive Tracking System architecture. 3G, third-generation; GPRS, general packet radio service; SMS, short message service; WLA, wireless local area network; XML, extensible markup language.
The developed system has portable spirometry (produced by Thor Medical Systems, Budapest, Hungary) that has an automatic internal calibration. In addition, the Nokia (Espoo, Finland) 5800 is used as the smartphone. The parsing of received data, the real-time evaluation of data, and the generation of the classification results are achieved on the smartphone. The XML Web service is used to store measured and generated data to the remote server database, and vice versa. General packet radio service, wireless local area network, or third-generation networks can be used for transferring the data from a smartphone to the remote server database.
The system has a firewall and a Web server. These devices have an open-source operating system. Apache, Apache Tomcat, MySQL, SSH, and phpmyadmin are installed on the Web server. These are open-source Web server software. Apache is used for hosting the Web pages. Apache Tomcat is essential for the running of Java-based applications. MySQL is used as a database. SSH is used for remote access. In addition, phpmyadmin is used for administration of the database. The Web server hosts Web pages and stores data in the database. Patients' personal information, test results, the generated classification results, and the data of Web pages are stored in the database. In addition, classification results and recommended actions are converted automatically into the SMS XML template. Then, an SMS is sent to the patient or doctor for information and emergency purposes by means of a private company's SMS gateway.
Statistical PFT data can be accessed at anytime and from anywhere through the Web pages. The doctor and the patient can send an e-mail to each other through the Web page for treatment purposes. This two-way system has led to remote tracking and self-management. Useful information related to lung diseases is also given in the Web pages. JQuery plug-in is used to plot flow–volume and volume–time graphs. These graphs consist of approximately 1,000 points that are retrieved from the spirometry. The smartphone receives and transmits volume–time and also flow–volume loop data to the remote database. The database stores the data of these graphs. Each point in the loop data can be examined through the Web page. In Figure 2, the flow–volume graph can be examined point by point in the Web site.
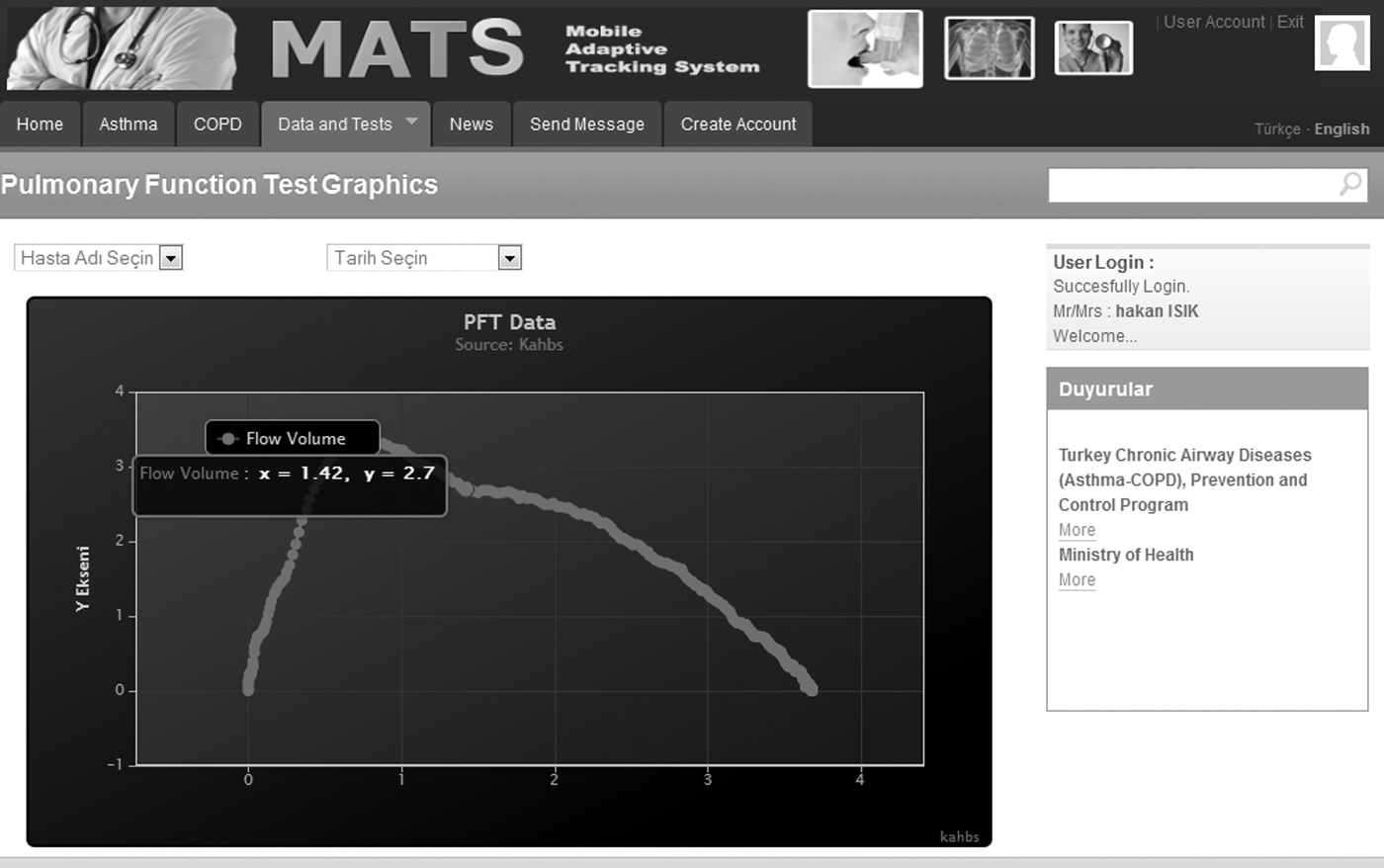
Classical Web page of the Mobile Adaptive Tracking System. COPD, chronic obstructive pulmonary disease; PFT, pulmonary function test.
Because of the small screen and limited data transfer, the mobile Web page is also designed for a smartphone. All data can be seen and tracked on the mobile Web page.
The system developed has an adaptive feature with the artificial neural network algorithm. This algorithm has the ability to learn how to classify inputs based on the data given for training. In training, the algorithm changes network weights and bias values to adapt new structures. The system is also considered as cost-effective. The total cost of the system is only 900 Euros. There is no operating cost except for SMS. The cost per 40 SMS is only 1 Euro. In addition, The Ministry of Health in Turkey has started a national control program for chronic airway diseases (asthma, COPD) under the Global Alliance Against Chronic Respiratory Diseases umbrella in 2009. Approximately 8.5 million handicapped people are living in Turkey. With this program, they are visited in their home environment by the doctor, nurse, and a support person. The limited number of experts, time, and budget are main problems. It is believed that the system will reduce the number of visits of patients and medical expenses in this program.
To enhance the utilization of spirometry and the new system, a user-friendly system manual and a video program for operating the system have been prepared. In this manual, the user can understand how to perform a PFT with spirometry and to send test results. Moreover, clear instructions and troubleshooting steps of the manual give detailed information. The video program provides a visual description of the manual. It can be seen on the Web site.
The detailed information about the system is also given to the doctor such as how to track a given patient with Web pages, to manage SMS-based information, and to interpret data. In addition, the video for the doctor provides visual information with regard to this issue.
Materials and Methods
Subjects
The system developed has been tested with the patients in their home environment. In Tables 1 and 2, the features and information about patients are presented. The ages of patients are between 29 and 70 years. The selected patients have common features. For instance, they already have a mobile phone, and they have performed a PFT in the hospital previously. In addition, they have some general knowledge on avoiding hazardous factors such as perfume and polluted air. They also know about their treatment and the plan for drug usage.
Features of Patients
COPD, chronic obstructive pulmonary disease.
Personal Information of Patients
Before trial of the system at home, the patients visit the PFT Department of Atatürk Chest Diseases and Thoracic Surgery Training and Research Hospital. PFTs of young and old patients are observed in the hospital environment. In addition, detailed information about PFTs and patient cooperation has been given to the patient by the technician of the PFT Department such as how to use the spirometry and troubleshooting steps. Then, the selected patients are visited at their homes.
In the BP-ANN classification, data of 486 adult volunteers (313 normal individuals, 136 patients with obstructive disease, and 37 with restrictive disease) were used in this study. The dataset for the analysis was divided into 80% training set and 20% test set, consisting of 389 and 97 samples, respectively.
Methods
In this study, the BP-ANN-based Mobile Information Device Applet application is developed with the Java 2 Micro Edition environment. This application runs on a mobile smartphone. This application acquires PFT data from spirometry through the Bluetooth virtual serial port protocol. The data are detected with the cyclic redundancy check-16 technique. It is used for detection of errors in received data. Check bits are used to find errors in transmission and received data. If there is an error, the smartphone application sends a negative acknowledgment message to the spirometry and requests retransmission. If there is no problem, the dataset is parsed. Finally, the personal information of the patient and the five important PFT parameters (lung forced vital capacity [FVC], forced expiratory volume in the first second [FEV1]/FVC, forced expiratory flow in the middle of an expiration [FEF25–75], FEV1, and peak expiratory flow [PEF]) are obtained. Then, the data are evaluated by the BP-ANN algorithm.
Evaluation Flowchart of PFT
The evaluation flowchart of the PFT results is shown in Figure 3. This flowchart and the system architecture are designed in accordance with the recommendations of the doctor. The acceptability requirements must be met for the assessing measurement. For instance, the difference between highest and lowest FEV1 values must be less than 200 mL. In addition, at least three actual tests must be applied by the patient. Except for PFTs, all flowchart steps are done by smartphone. For instance, the reference values of the patient are calculated depending on patient's gender and age. With FVC, FEV1/FVC, FEF25–75, FEV1, and PEF as an input attribute, BP-ANN-based classification is performed. If the classification result of the patient is found as obstructive, an additional test is required. After the patient inhales the bronchodilator, a new test is performed. Depending on the difference between the new FEV1 value and the average of the previous results, the patient is considered as having asthma or COPD. For instance, if there is a 200 mL difference between the new FEV1 value and the average of the previous results, the patient's status is reversible, and it is labeled as asthma. Then, the obtained result is sent via SMS.
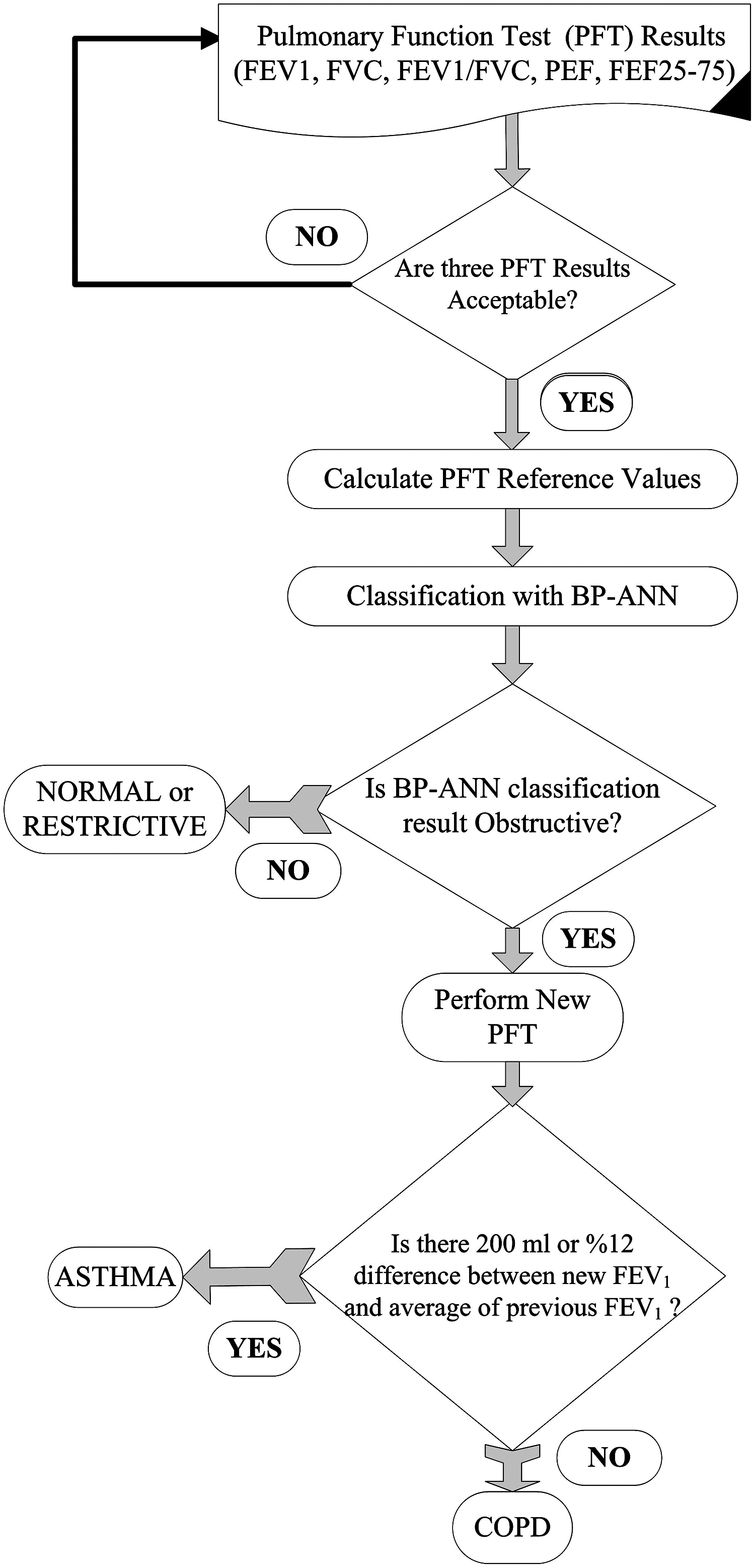
The evaluation flow chart of the pulmonary function test (PFT). BP-ANN, back propagation artificial neural network; COPD, chronic obstructive pulmonary disease; FEF25–75, forced expiratory flow in the middle of an expiration; FEV1, forced expiratory volume in the first second; FVC, forced vital capacity; PEF, peak expiratory flow.
In this study, the BP-ANN is used as a classification algorithm for PFT results. This algorithm consists of the training and the test process. The training process is achieved through the hospital training data. The data include five input attributes and the classification results. Classification results are considered as expected values in the data. After the completion of the training, the testing process is done on the trained network. This process only includes the feed-forward phase. The training process consists of two phases. These are the feed-forward and the back propagation phase. The output classification result is obtained in the feed-forward phase. In this phase, tansig is used as the activation function because it provides more effective results than the other equation. The tansig result can be found with Eq. 1:
where Q[k] is the weighted sum of the inputs of the processing unit k. The artificial neural networks consist of the interconnecting artificial neurons, in other words, the processing units.
The output error is obtained by subtracting the obtained value from the expected value. Then, this error is back propagated. After that, the feed-forward phase is done. This cycle is repeated until the number of iterations is reached. In every cycle, the weight and the bias values are updated. As shown in Figure 4, the network training is carried out by updating the bias and weight values. With this way, the learning cycle of the algorithm is completed.
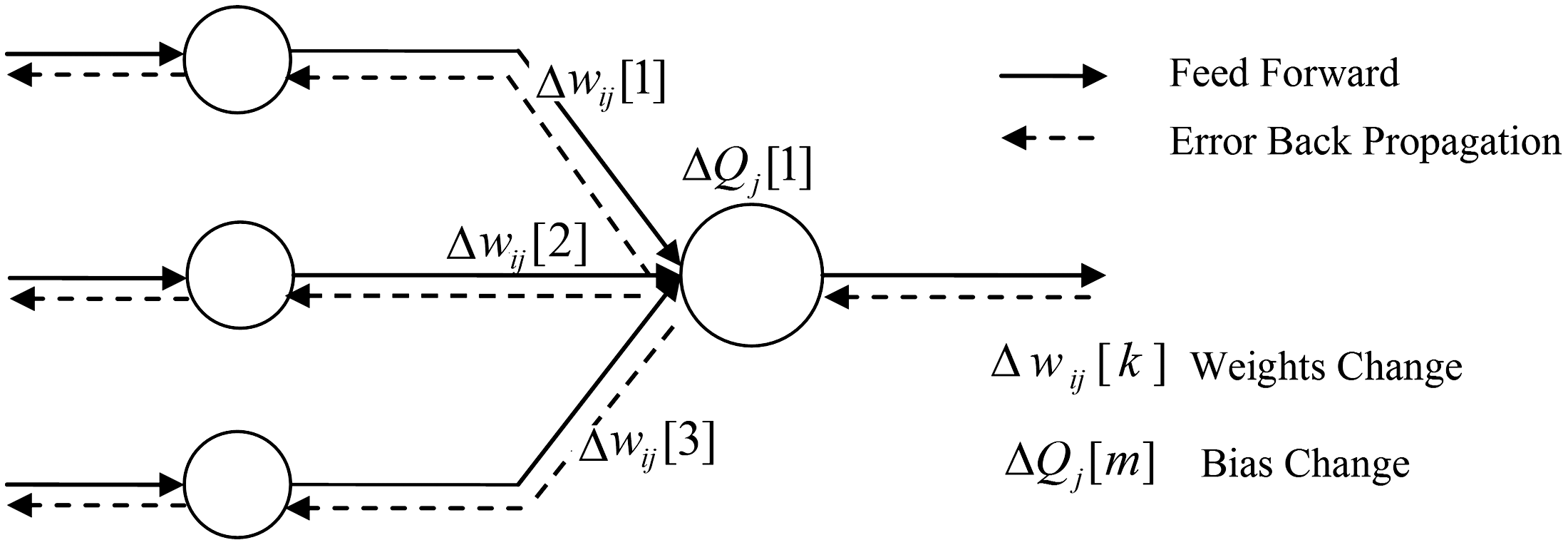
The back propagation artificial neural network learning cycle.
The designed BP-ANN has five input attributes, two hidden layers, and three output parameters as shown in Figure 5. The input and the hidden layers have five processing units.
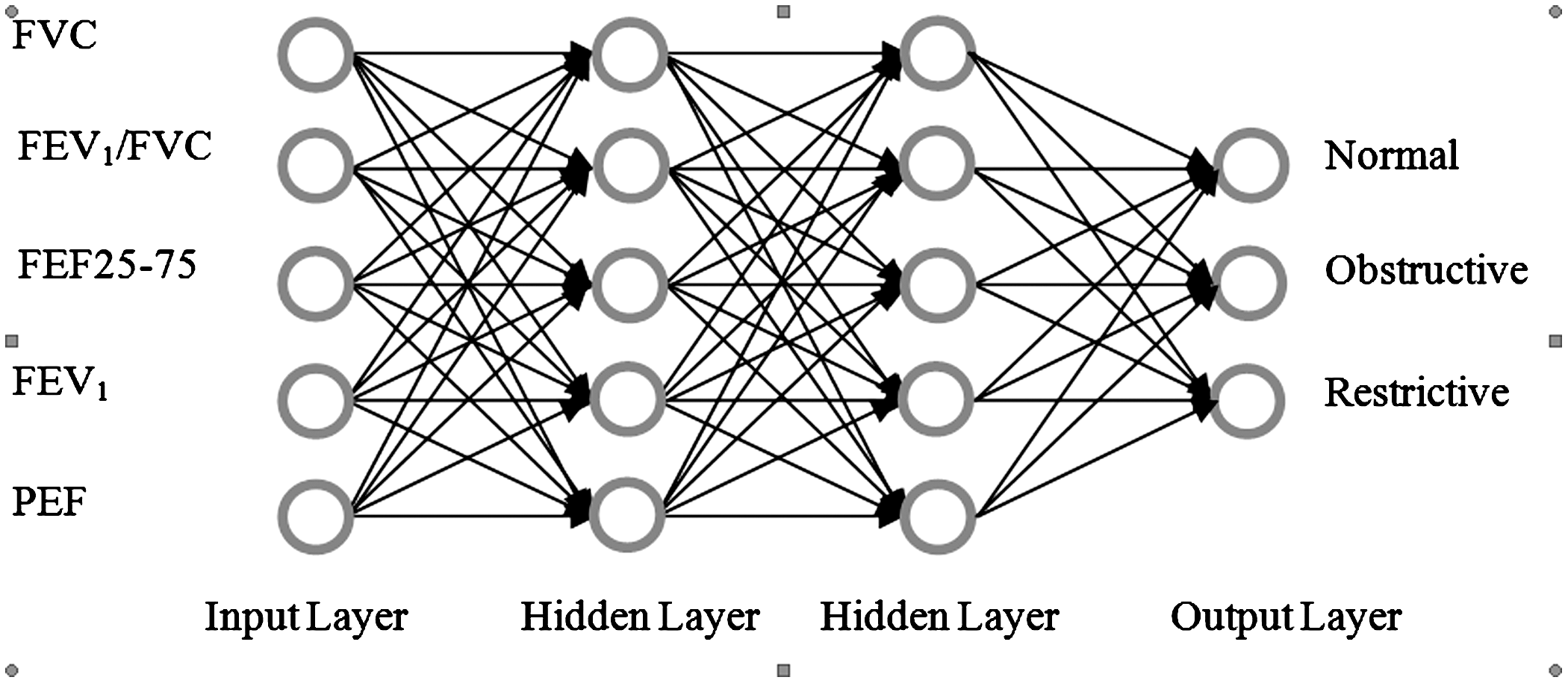
The back propagation artificial neural network architecture of the system. FEF25–75, forced expiratory flow in the middle of an expiration; FEV1, forced expiratory volume in the first second; FVC, forced vital capacity; PEF, peak expiratory flow.
The performance of the BP-ANN is evaluated on real data. These training and test data, obtained from Atatürk Chest Diseases and Thoracic Surgery Training and Research Hospital with the permission of the Ministry of Health, contain five attributes.
In the BP-ANN, these five parameters (FVC, FEV1/FVC, FEF25–75, FEV1, and PEF) are used as input attributes to measure the lung capacity and power. The BP-ANN training is performed every 1,000 iterations in 1,000 times training. The total training cycle has 1,000×1,000 iterations. The learning rate and the momentum are taken as 0.05 and 0.9, respectively. The result of the BP-ANN is the classification of chronic lung disease pattern. These patterns are normal, obstructive, and restrictive. In addition, the COPD and asthma differentiation can be performed for obstructive patients.
Results
In this study, the different architectures of BP-ANN were tested, and the best architecture with the highest accuracy, specificity, and sensitivity was selected. The results of the different BP-ANN structures for the test set are presented in Table 3.
Performances of Different Back Propagation Artificial Neural Network Structures
AUC, area under the curve.
In the four-layer case, the 5-5-5-3 configuration has the best results in classifying respiratory patterns. This configuration has 98.7% accuracy, 97.83% specificity, 97.63% sensitivity, and 0.946 correlation value. In addition, this configuration has an area under curve (AUC) value of 0.971 as shown in Figure 6. Different four-layer configurations have similar results. As a result of the smartphone's high speed processor (434 MHz), the evaluation delay has not been seen in the four-layer configuration.
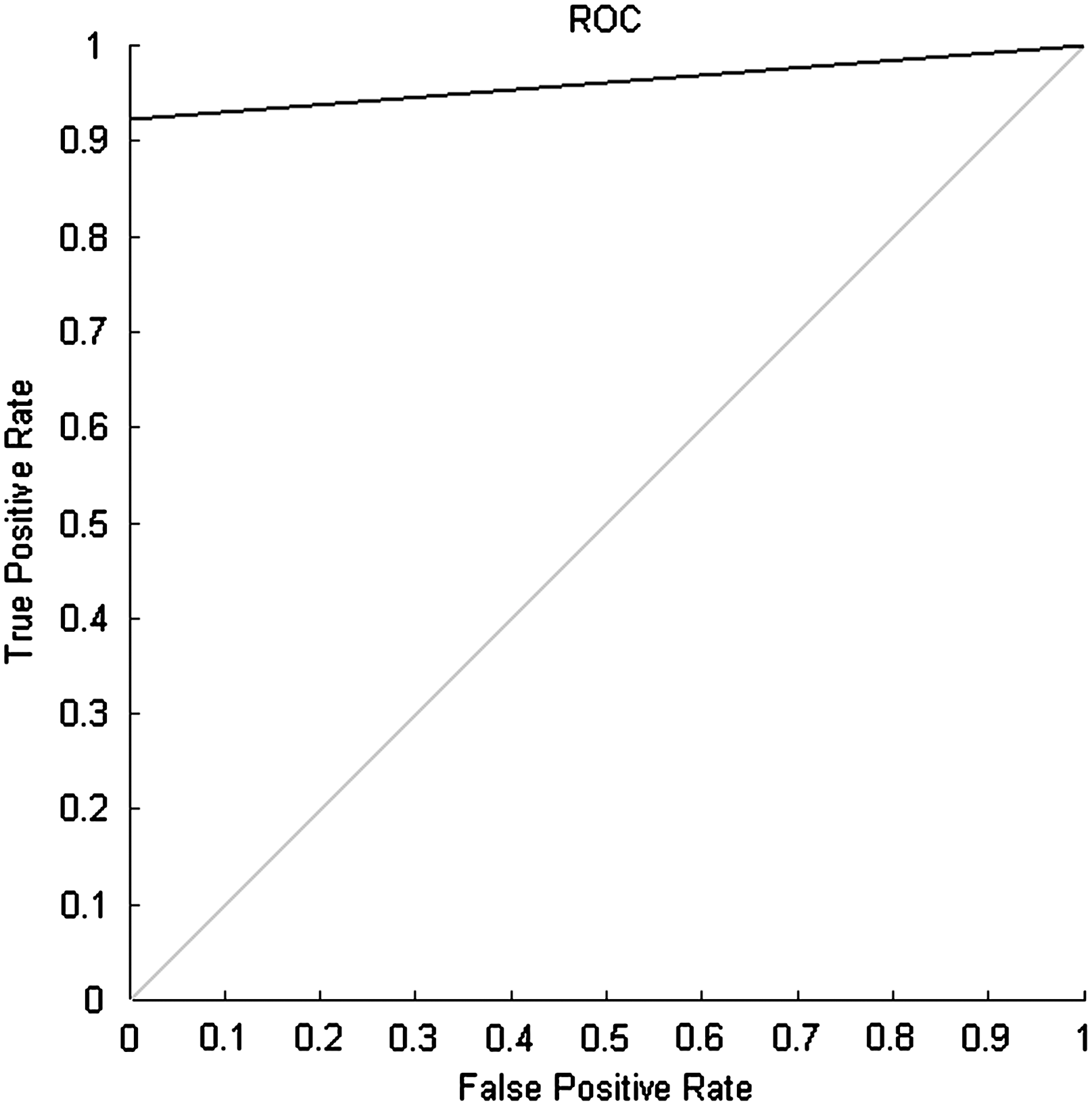
Receiver operator characteristic (ROC) graphic of the 5-5-5-3 configuration.
In this study, the results of the algorithm are promising. When this study is compared with previous studies, 17 –19 it is seen that the classification accuracy has improved (study accuracy is 98.7%).
As is well known, the rule-based Global Initiative for Chronic Obstructive Lung Disease algorithm is frequently used by doctors. They evaluate chronic pulmonary patients' diseases with this algorithm. It uses FEV1 and FEV1/FVC parameters for classification of patients' diseases. Its accuracy is found to be 72.2% with the same test data. The improvement and the utility of the BP-ANN have higher classification accuracy in comparison with the Global Initiative for Chronic Obstructive Lung Disease algorithm.
As displayed in Figure 7, the generated result and the obtained data are shown in the smartphone screen.
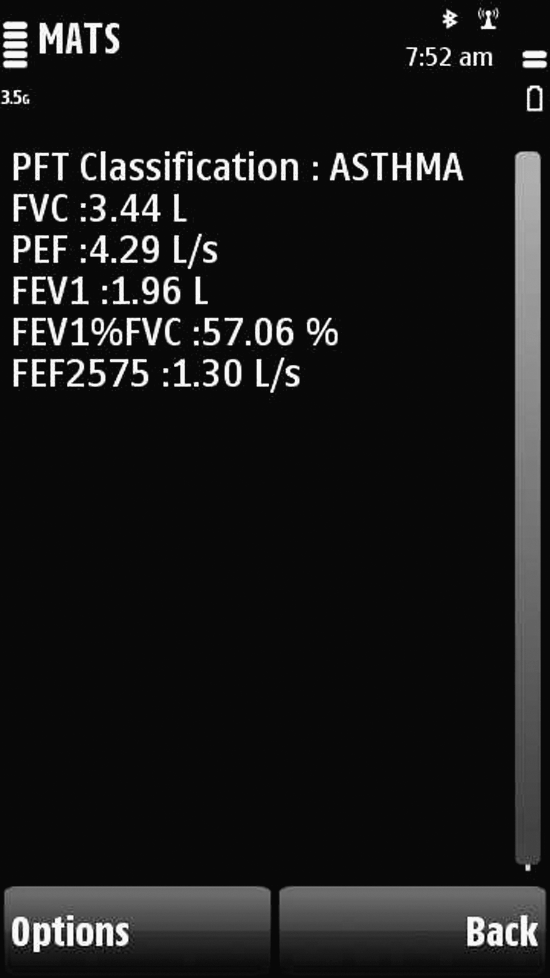
Pulmonary function test (PFT) data and classification result in the Mobile Information Device Applet. FEF2575, forced expiratory flow in the middle of an expiration; FEV1, forced expiratory volume in the first second; FVC, forced vital capacity; PEF, peak expiratory flow.
In the application of the system, it is understood that the training period depends on the usability of the touchscreen smartphone. The training of the system takes about 30 min for those who already use a touchscreen phone, whereas training for elderly patients and normal mobile phone user patients takes about 3 h. The training is completed after a successful performance of the patient's test. Each patient uses the system in his or her home for 7 days. It is believed that patients should be visited periodically to motivate them and to avoid mistakes.
Initially, a 70-year-old patient can perform the test but cannot use the touchscreen smartphone. At the second visit, he or she is able to use the same phone. A 51-year-old patient who already has a touchscreen smartphone can easily use the system. In addition, this patient checks his or her test data with classical and mobile Web pages. In his or her view, he or she can use the system for self-management. In the home environment trial, the initial result of the portable spirometry is compliant with the hospital diagnosis for all patients. According to the patients' point of view, they would prefer MATS because of the possibility of the reduction in the frequency of hospitalization, because of real-time remote tracking by the doctor, and in emergency cases such as ambulance intervention.
It is observed that the doctor who is equipped with 1 week of patient data can give advice to patients regarding bronchodilator and steroid usage. The emergency case SMS that is sent to the doctor prevents some circumstances such as unnecessary directing of the ambulance.
Discussion
The performance results of the system can be increased by adding additional data, iterations, or different machine learning algorithms. Although comparison of the BP-ANN algorithm results with those of other machine learning algorithms would be valuable, it is beyond the scope of the article.
As is well known, the diagnosis of chronic diseases depends on several parameters such as allergy and family history. Therefore, our study focuses on the tracking of diagnosed patients. The main limitation of the system is touchscreen smartphone usage. This difficulty is accomplished by providing additional patient visits. From our point of view, if it is possible to test the system in the long run, it will reduce the number of hospital visits and the deterioration of asthma to COPD.
Conclusions
Advances in biomedical technology, communication infrastructure, and also innovative software provide new opportunities and assist patients' tracking and self-management. In the meantime, the aging of the population and the prevalence of chronic diseases are becoming substantial challenges for our world. In this context, this system providing real-time smart management with mobile and wireless technology of chronic pulmonary patients comfortable in their home environment has been developed. This mobile health system uses mobile and wireless facilities. Patients are equipped with a smartphone-based telemedicine system. The research realized in this work provides effective, real-time healthcare provision. It is intended to measure PFT data at home that currently are only obtained from patients at the hospital. SMS texts related to the emergency and information purposes realize the remote support as well as self-management for patients at home. It also facilitates the tracking of elderly people who have difficulty due to the progression of their illness. The Web pages inform patients and allow them to control their disease themselves. In addition, doctors can easily track patients.
The main innovations of the system are the real-time classification on the smartphone with a new input attribute (FEF25–75) on the mobile BP-ANN algorithm and the SMS-based notification. This SMS includes PFT data, the classification result, and the recommendation such as “please contact your doctor immediately.” This system also performs normal, obstructive, and restrictive classification, as well as asthma and COPD differentiation for obstructive patients. In addition, potential communication problems are avoided by processing of data on a smartphone instead of a Web server. In the case of a communication difficulty, the system will still work without the data to be sent to the Web server. With this study, real-time support and tracking of a chronic pulmonary patient comfortable in his or her home environment is realized. Replacing the doctor, the regular treatment, and the diagnosis are beyond the scope of the study. Modular system architecture enables us to add additional telemedicine instruments such as electrocardiogram, blood pressure, or glucose measurement devices. It is believed that the portable system can be used for handicapped people who have difficulty in reaching healthcare facilities.
Footnotes
Acknowledgments
This work was supported in part by Gazi University scientific research project number BAP-07/2010-55.
Disclosure Statement
No competing financial interests exist.