
Abstract
Introduction
The present study is focused on daily telerehabilitation (D-TR) for gait at home and at the hospital. 1 –3 When designing a complete D-TR process for patients, it should be borne in mind that patients should be furnished with properly designed methodologies for executing specific motion tasks and the assessment of relevant parameters. In general, such a process should feature three basic elements in both the hospital and the home: (1) instrumented walkways (IWs), (2) walking aids or supports (WAs), and (3) parameter assessment equipment.
IWS
The IWs 4 used in D-TR comprise stairs, slides, walkways instrumented with handrails, and grounds with different rugosity (a measure of small-scale variations or amplitude in the height of a surface) and/or the presence of obstacles. There are also daily-life paths for different areas at home, such as paths with slides, stairs, etc., and grounds of varying rugosity. Figure 1 depicts a possible scenario for rehabilitation purposes in the hospital or at home: a pathway embedding a cascade with different walkways—(a) with and without handrails, (b) stairs, and (c) a slide—with rugosity values of ρ1, ρ2, and ρ3 and with the presence of obstacles. Figure 2 shows a cascade of flat walkways that constitute a complex pathway in the form of a labyrinth (for both neurological and cognitive rehabilitation) for D-TR purposes at home [(1) linear, (2) curved, and (3) linear with obstacles].
Possible rehabilitation pathway with a cascade of three rehabilitation tools: handrail, stairs, and slide (ρ x is the rugosity).
A horizontal view of a rehabilitation pathway at home with a cascade of three walkways (linear walkway, curvilinear walkway, and linear walkway) with different rugosity (ρ x ) and obstacles affixed along the walkways.
WAS
These range from the plain cane 4 up to systems for body gravity reduction 5 and include:
• Assistive devices such as canes, crutches, and walkers. They redistribute and unload a weight-bearing lower limb, improve balance, reduce lower limb pain, and provide sensory feedback.
• Orthoses for supporting parts of the body load (hip, knee, ankle, etc.) during deambulation. Nonexhaustive examples are ankle foot orthoses, hard braces worn on the lower leg to support the ankle and the foot junction during walking and that furnish elastic propulsion to subjects with neuromuscular pathologies affecting normal gait. The Codivilla spring is a well-known example.
• Reciprocating-gait orthoses and advanced reciprocating-gait orthoses. Reciprocating-gait orthoses and their evolution of advanced reciprocating-gait orthoses 6,7 are orthoses designed to assist the gait with alternated footsteps, for example, in the paraplegic patient. Reciprocating-gait orthoses and advanced reciprocating-gait orthoses are the only orthoses that allow these patients to walk independently, but they are poorly used because of their encumbrance, weight, and unpleasant esthetics, resulting in most patients preferring to use a wheelchair.
• Systems reducing body gravity. These range from swimming pools up to complex systems 5,8,9 such as the walking assistance and rehabilitation device, a pneumatic system for body weight relief in gait rehabilitation. 5
Parameter Assessment Equipment
Parameter assessment equipment ranges from the very simple wearable step counters up to complex, expensive optoelectronic systems:
• Optoelectronic/ultrasonic solutions. The gold standard approach
10
used in movement analysis is based on the measurement of the position of markers affixed on body segments by means of optoelectronic technology (
• Wearable solutions. The wearable solutions are given by those systems that can be embedded in a pocket. The following are nonexhaustive examples:
∘ Wearable motion sensors with accelerometers and gyroscopes. As an alternative to the optoelectronic/ultrasound in the 1970s, Morris
11
and Padgaonkar et al.
12
showed the potentiality of accelerometric techniques. Research laboratories
13
and industries have recently proposed different solutions that use both accelerometers and rate gyroscopes, for example, the MT9-a sensor from Xsens (
∘ Wearable step counters. The step counter (or pedometer) is conceptually very simple in design and requires no additional software or expertise to access or interpret data. Step counting is an important index of motion activity, currently used in the prevention of obesity, in applications for the prevention of cardiovascular problems, in diabetes care, and, more generally, in motion monitoring and rehabilitation. 14 However, problems still exist concerning their accuracy. 15 The authors have designed and constructed new solutions to these problems. 16,17
• Wearable solutions for activity monitoring. The ability to accurately monitor the amount of daily physical activity is particularly important in the elderly, as regular physical activity is associated with both physical and mental health and is a primary way to study health-related quality of life. For this reason for the last two decades many authors have investigated techniques for activity monitoring (some even use the smartphone).
18
–21
Commercial solutions are also available today. An example is the LifeGait System (MiniSun LLC, Fresno, CA), a device small enough to fit in the palm of a hand. The LifeGait System has been supported by a U.S. National Institutes of Health grant (
• Portable systems. Portable systems are those that can be furnished in a suitcase to patients at home or in the hospital. An example is the GAITRite® system (CIR Systems, Sparta, NJ),
22
mainly used in motion laboratories. The GAITRite system automates measuring temporal (timing) and spatial (distance) gait parameters via an electronic sensorized carpet connected to a personal computer (
Objective
The global aim of this study was to design, construct, and test a kit for the integration of all the above elements (IWs, WAs, and parameter assessment equipment) and devise a D-TR process adaptable to both clinical and home environments that will keep the rehabilitation treatment alive and monitored. The solution must be simple and suitable to quantify the daily assessment and to furnish useful parameters of a patient's physical and physiological conditions during care therapy, wherever the patient is performing his or her rehabilitation task (hospital, gym, physiotherapy room, or home).
It should be borne in mind that to date the assessment of the improvement of subjects under a rehabilitation process while exercising on IWs or cascades of IWs (pathways) is difficult to achieve by means of optoelectronic systems because of the complexity of the setup and the shadowing effects of the markers. The use of other portable systems such as the GAITRite system—which uses a sensorized carpet—is not feasible in consideration of the length (10–20 m) and geometry (stairs, obstacles) and the need to investigate grounds with different rugosity. For these reasons, the assessment of improvement in rehabilitation subjects during exercise is mainly based on subjective observation and not on automatically furnished parameters such as kinematic ones.
Because the focus is on gait, the idea was to design a simple, portable kit—as an alternative to the complex and expensive instruments currently used—that may be easily interfaced or integrated with existing IWs both for self-monitoring, while patients are exercising with their own aids, and for clinical reporting. Figure 3 illustrates the final scenario as it has been planned in the study. The portable kit equipped with an accurate step counter and information and communications technology solutions should allow the automatic measurement of parameters useful to the clinician (e.g., time, velocity, and number of steps during the execution of an exercise in a cascade of IWs) and the configuration of those parameters in the form of a report to send out by means of a communication unit over the local or wide area network.
General block scheme of the station-to-station rehabilitation and assessment system. CU, central unit; LAN, local area network; WAN, wide area network.
Materials and Methods
The methodological flow we followed was (1) definition of the architecture of the clinical system and modeling parameters and (2) design and construction of the hardware solution and software interface.
Architecture of the Clinical System
The aims of the system were as follows:
• During a rehabilitation task of a predefined protocol, monitor the steps on an assigned walkway of a defined length and determine all the relevant parameters of velocity and time.
• Preprocess this information to obtain other useful gait parameters.
• Format this information into an ASCII text file, easy to send to a communication center for postprocessing purposes and to store in a database-specific format.
The complete architecture (hardware and software) of the system is as follows: the hardware unit allows for the telemetric acquisition of the rough data from the subjects. The data are sent out by means of an USB acquisition card (model NI-DAQ USB-6008; National Instruments Corp., Austin, TX) connected to a PC. A software interface, designed with LabVIEW version 8.2 (National Instruments Corp.), preprocesses the information in the PC, rearranges it in an ASCII text file, and uploads it through a local or wide area network connection for the final postprocessing and archiving.
Design and Construction of The Hardware Solution and Software Interface
The minimum hardware solution consists of the following:
1. Step counter
Different step counters can be used in the hardware solutions, such as sensors based on accelerometers, rate gyroscopes (
2. Detectors along the path
This study has focused on the case of a pathway consisting of a cascade of two IWs with handrails.
The assessment of the start, intermediate, and final position of the path is central to detect the duration (in time) of the exercise associated to each walkway. This timing also acts as a temporal window for step counting. Only the steps actually monitored during this timing interval are used to increment the total number of steps. Three couples of photo-emitter/detector (PHO-DE) devices (model PEM10D; Wellean, Gavere, United Kingdom) and relevant mirrors have been used in the cascade with two consecutive walkways; they were positioned at the start and the end of the first walkway and at the end of the pathway (second walkway). The first PHO-DE couple detects the T start of the task, the second detects the T int at the end of the first walkway (and start of the second walkway), and the third couple detects the T stop, the final timing of the task.
3. Central unit
The central unit is telemetrically connected with the other components of the equipment and provides the following functions: A. Real-time assessment of the number of steps B. Step counter recharge C. Elaboration of the timing-related rough data D. Biofeedback seven-segment light-emitting diode representation of the data E. Connection to send the timing parameters to a PC
Figure 4 shows the components of the kit. Figure 5 shows the timing (some channels are available for further applications and/or expansion of the cascade of walkways).
The components of the portable kit. GEMU, gastrocnemius expansion measurement unit.
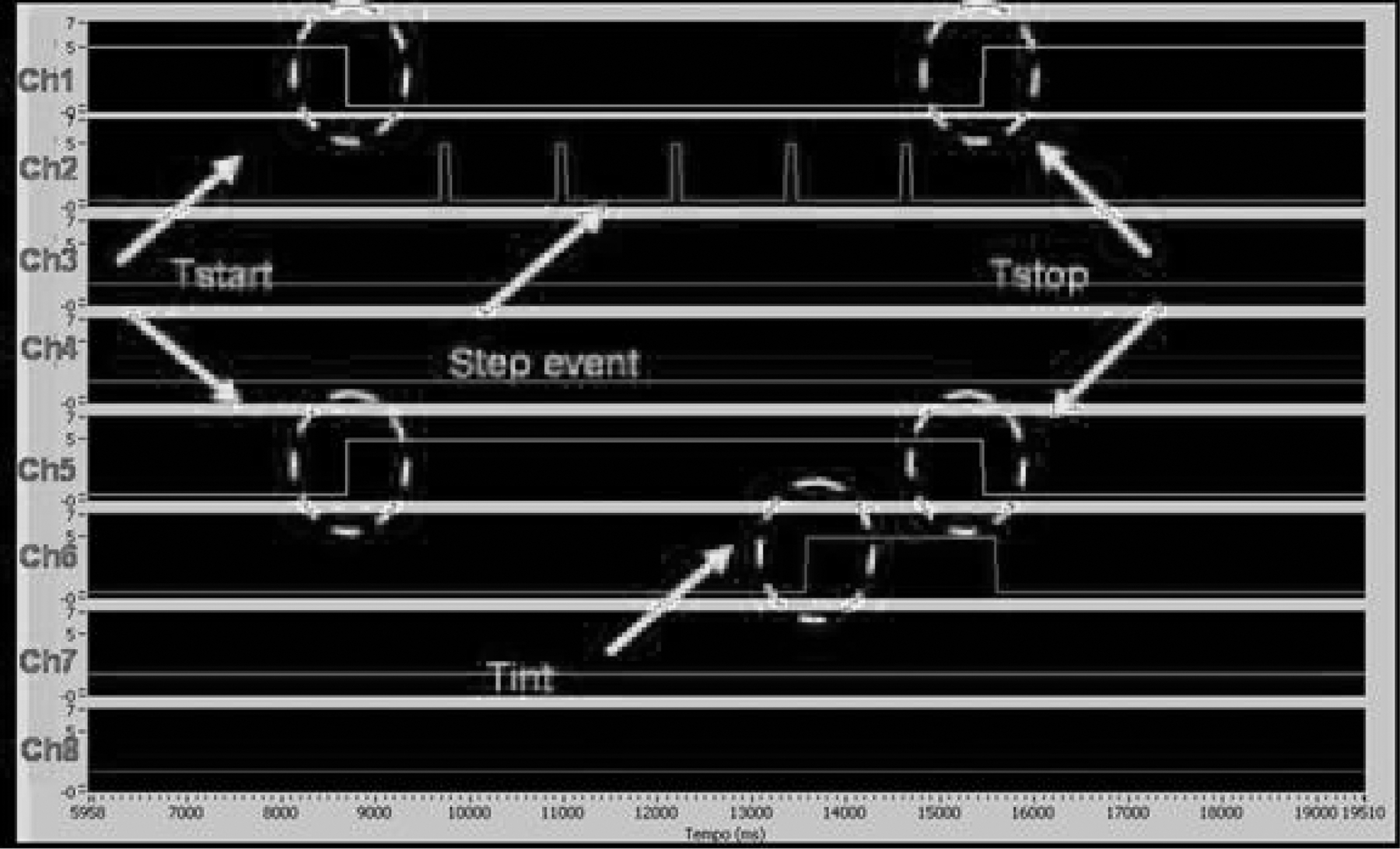
Timing monitored at the central unit on different channels.
4A. Software interface: parameters from the portable kit
In the case of a single walkway, starting from the number of steps N
step during Δt=T
start – T
stop: • The exact mean velocity V
m (Eq. 1), knowing the distance d and the interval of time Δt masking the exercise: • The approximated step-length l
step (Eq. 2): and thus • As limits of errors: the superior and inferior ranges of step length l
step-sup and l
step-inf (Eqs. 3 and 4, respectively) obtained in the case of the maximal range of errors at the moment of the end of the exercise, in consideration of a±0.5 step:
As a numerical example, in the case of a 10-m walkway and N
step=15 (Eq. 5), from Eqs. 2
–5 we obtain l
step=0.666, l
step-sup=0.689, and l
step-inf=0.645. This result shows that also in the case of maximal errors at the end of exercise, the estimated length of steps differs by a value of about 2×10−2 m (i.e., the contour of a shoe). However, repeated measures associated with statistical models give satisfactory results as shown below:
The data processing according to Eqs. 1
–4 is obtained by the following described software interface. In the case of a cascade of J walkways, the parameters for each walkway I (I=1..J) are the ones described by Eqs. 6
–8:
Software interface: software program
A software program was developed for monitoring the gait of patients wearing different step counter sensors in a cascade of two different walkways (i.e., linear flat floor, with or without obstacles, slide, stairs). The gait parameters were stored in an ASCII text file also containing the patients' name and the features of the walkway (length, type of pathway, type of gait aid). The program was developed with LabVIEW programming language (Laboratory Virtual Instrument Engineering Workbench) version 8.2, accepting signals from different sensors. Customized user interfaces were designed in order to control the patients' gait and to configure the features of the walkway. Figure 6 shows the interface proposed to monitor a gait session consisting on one or more trials. With the “Step Counter Type” control button one can choose from the drop-down menu the wearable step counter sensor (GEMU, rate gyroscope, SECOSP, accelerometers); the table with the header “GAIT AID—PATHWAY TYPE—NOTE” shows the selected features of the walkway. These features can be set by means of the configuration interface illustrated in Figure 7. For each path, the user has different choices for “Gait Aid Type” (NONE, HANDRAIL, CANES, CODIVILLA SPRING) and “Pathway Type” (LINEAR FLAT FLOOR, WITHOUT OR WITH OBSTACLES, SLIDE, STAIRS) and may introduce information on path rugosity in the “NOTE” field.
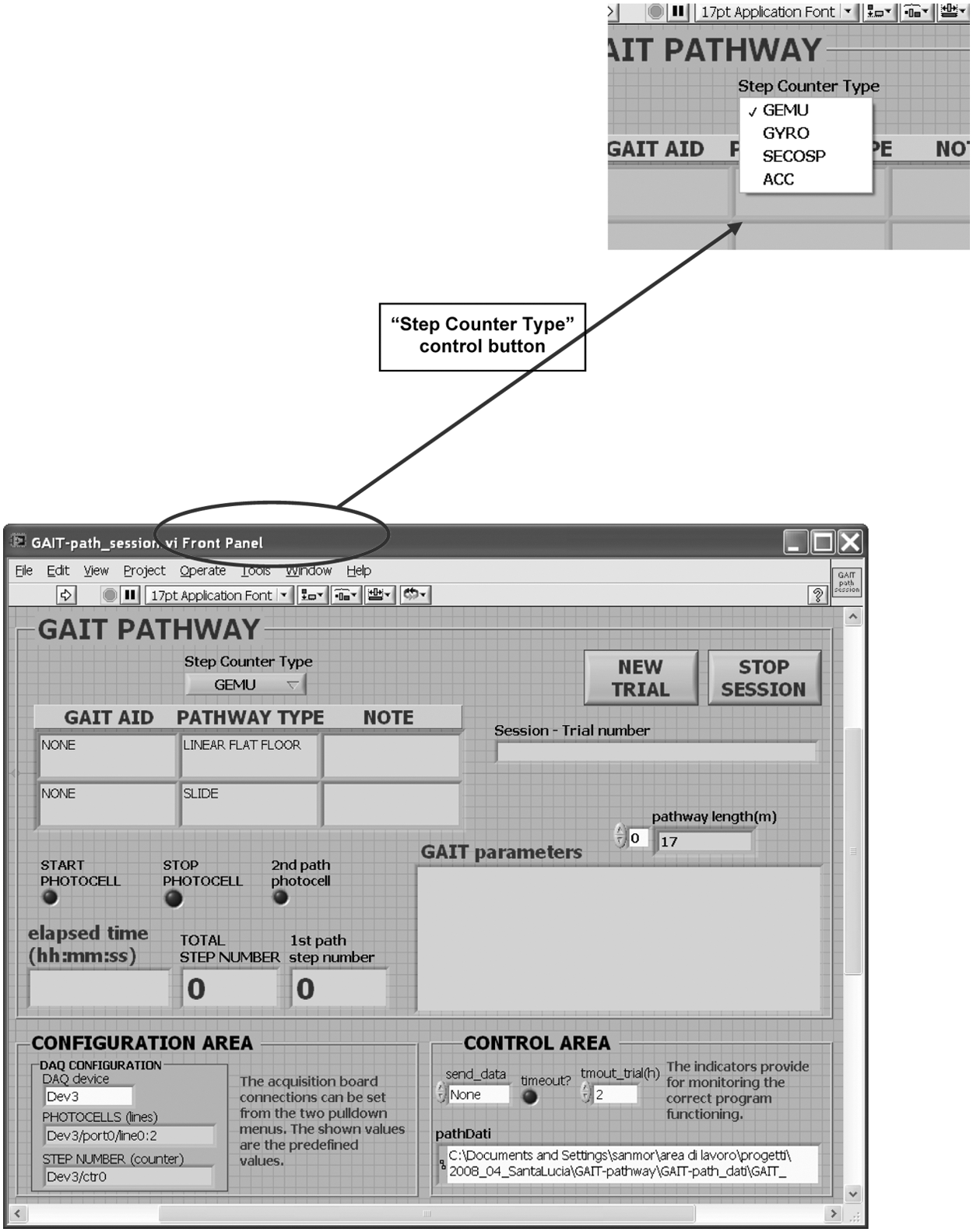
Interface for the monitoring of a session of gait. ACC, accelerometer; GEMU, gastrocnemius expansion measurement unit; GYRO, rate gyroscope; SECOSP, sensorized Codivilla spring.

Interface for the configuration of the whole pathway.
Results
Validation Setup
The validation was conducted using a GEMU. 17 Recruitment of subjects was voluntary and in accordance to the declaration of Helsinki.
Protocol of validation
The protocol of validation consisted of three repetitions at a maximal speed of three trials, each one starting from a different standing position (1, legs aligned; 2, right leg forward; 3, left leg forward) at the level of the first PHO-DE couple.
Subjects
The methodology was applied to a group of 16 subjects at the second level of the Tinetti test of motion unbalance. 23 There were eight men and eight women, with a maximum age of 70 years and minimum age of 34 years (standard deviation, 15 years), maximum weight of 94 kg and minimum weight of 47 kg (standard deviation, 21 kg), and maximum height of 1.85 m and minimum height of 1.48 m (standard deviation, 0.21 m).
Statistics of the population sample
For the statistical analysis Minitab® software (Minitab Inc., State College, PA) was used. The analysis of the sample based on the Anderson–Darling normality test showed that there was no evidence that the chosen sample did not follow a Gaussian distribution in age (p>0.12), height (p>0.11), weight (p>0.12), and body mass index (p>0.10).
Configuration of the IWs
The pathway has been thought out in order to emulate both the home and clinical conditions. The pathway has the following characteristics: a cascade of two linear walkways with handrails (10 m long). The first walkway is made of parquet; the second walkway is made of moquette and has an inclination of 5°. For safety reasons, subjects were followed by an application giver during the exercise.
Validation Outcome
Statistical significance
Tables 1 and 2 show the final results in terms of velocity and measured step length relative to each of the components of the cascade with the two IWs. There was no evidence that data did not follow a Gaussian distribution; in particular, the Anderson–Darling normality test showed that significance was
• p>0.09 for the velocity and p>0.08 for the number of steps for the first walkway and
• p>0.10 for the velocity and p>0.09 for the number of steps for the second walkway.
Outcomes of the Parquet and Moquette Walkways
SD, standard deviation.
Acceptance of the Methodology
The maximum acceptance score was 3.
Outcome in detail
Each trial was video-recorded. No errors were detected in the step counting by means of GEMU. Table 2 shows the acceptance as investigated on the 16 subjects and on 4 application givers (1 for every 4 subjects) involved in the study on the basis of a method furnished by Hutten et al. 24 Table 3 is the output of a single trial with all the parameters cited above.
Outcome of a Single Trial on the Parquet Walkway
Costs
Table 4 shows the direct costs. The cost of production for the minimum setup has been separated from the cost of the study to allow for the estimation of serial production. The final cost of the prototype equipment was 948 € for materials, assemblage, and testing and 955 € for the study (i.e., about five times lower than the cost of a baropodometric equipment and hundreds of times lower than the optoelectronic equipment). The cost of the software has not been included because LabVIEW version 8.2 generates an executable file (no cost) for the interface. As this software is currently available in biomedical laboratories for the design of general bioengineering instrumentation, there is no sense in including it in the cost forecast.
Estimated Cost of the Production (Materials, Test, and Construction) and of the Study of the Circuit, Layout and Place & Route, and Software
PIC, programmable integrate circuit; ACC, accelerometer; GEMU, gastrocnemius expansion measurement unit; GYRO, rate gyroscope; SECOSP, sensorized Codivilla spring.
Discussion and Conclusions
Today there is continuous demand for easy, low-cost, interoperative rehabilitation technology to promote and monitor health. One of the most widely used technologies in motion monitoring is the step counter or pedometer. Step counting is an important index of motion activity and useful to monitor the response to therapy in rehabilitation, obesity, and diabetes care. 14,15 Furthermore, when it is accompanied with other kinematic information such as velocity, distance, and time, it could furnish physicians and therapists with useful quantitative information to assess the progress of a patient and useful biofeedback information that may motivate the patient to continue the therapy.
In this article we have proposed a kit that furnishes a solution to the problem of integrating a portable kit with a cascade of IWs for D-TR purposes. The kit comprises a hardware unit for the telemetric acquisition of the rough data from the subjects wearing a step counter and the triggering of the task by means of photocells. The rough data from the hardware unit are sent by means of a National Instruments acquisition board (model NI-DAQ USB-6008) to a PC via an USB connection. A software interface, designed by means of LabVIEW version 8.2, preprocesses the information in the PC according to a model and arrange it in an easy-to-manage text file that can be sent by local or wide area network connection for the final postprocessing and archiving purposes.
The kit has been successfully tested in an application consisting in a cascade pathway of two walkways with different ground rugosity and inclination, simulating both the hospital and the home environment. The acceptance was high.
From a global point of view the kit allows an easy monitoring of gait parameters with further advantages: A. It allows the use of different, properly designed step counters. We have used a GEMU for illustrative purposes, but different step counters can be used in hardware solutions such as accelerometers, rate gyroscopes, or SECOSPs.
16,17
B. It can be used with different ground rugosity. This is an important parameter affecting the lack of balance and, most important, the risk of falling. C. It can be used with different rehabilitation mechanical equipments (stairs, slides, etc.) and aids. D. The customization of complex walkways is also possible for daily monitoring; properly designed walkways in the form of complex paths (also with obstacles) may be designed, for example, at the patient's home to daily assess parameters and encourage motor activity.
Upon comparison with other solutions, the kit has the following advantages: a. Very low cost, not only when compared with optoelectronic solutions
10
but also when compared with other portable solutions such as activity monitoring by commercial solutions (e.g., LifeGait System) or the portable gait analysis systems (e.g., GAITRite
22
). b. Very high accuracy when using properly designed step counters for subjects with problems of imbalance, compared with commercial step counters or wearable systems with accelerometers and rate gyroscopes
11
–13
and activity monitoring systems.
18
–21
c. The comparison with the portable gait analysis system GAITRite
22
shows that the latter furnishes a very fine complete gait analysis limited to carpet distance with constant—not changeable—rugosity. The designed kit allows for a simplified gait analysis unlimited in length, shape (also labyrinths are possible), and rugosity. The two approaches are thus complementary.
To date there seem to be four possible directions for the portable kit improvement in D-TR: 1. Integration with the hospital information service. The equipment could be integrated into the hospital local area network and the hospital information service. 2. Integration with homecare equipment. The integration with homecare units assessing the most relevant medical parameters could allow for a more complete tracing of the rehabilitation care. 3. Enrichment of the equipment with further functions. Thanks to the thorough discussion between biomedical engineers and physicians, the addition of further functions is foreseeable and possible for different categories of pathology/patient. Thus the equipment as presented here represents a baseline version, which can evolve with the suggestions of the experts in the field and new needs of application protocols. 4. Domotics. The fourth direction consists in the integration of walkways at home in domotics. For instance, it could be integrated in a manner allowing for the assessment of gait in daily preferred trajectories. Such an assessment would allow for the measurement of gait-relevant parameters to monitor the improvement (during rehabilitation) or anomalies of motion activity with medical significance. Figure 8 shows an example of a possible monitoring D-TR environment using four walkways.

An example of application of four walkways in an apartment.
Footnotes
Acknowledgment
The authors gratefully acknowledge Monica Brocco for the linguistic revision.
Disclosure Statement
No competing financial interests exist.