
Abstract
Introduction
With rising rates and increasing burden of chronic illness management, newer strategies have included distant support for self-management, 1 such as home telehealth (HT) programs, which have been shown to improve chronic disease self-management and patient adherence to care plans, effectively monitor exacerbations, and decrease healthcare services utilization. 2 –6 Specific to heart failure (HF), the literature supports the use of HT programs with remote telemonitoring to improve health outcomes and/or decrease health service use. 7 –12 However, one significant problem repeatedly noted has been the amount of time and resources wasted on patients with poor rates of device utilization who are subsequently disenrolled from the program. 13,14
The Department of Veterans Affairs (VA) has had an HT program since 2003. Although there is evidence for its benefits, little is known about the association among device utilization or adherence rates, potential predictors of adherence, and subsequent outcomes. A study of Veterans with HF reported higher dropout rates for those assigned to use the Health Buddy® (Bosch Healthcare, Palo Alto, CA) device, one of the commonly used HT devices in the VA, 15 –18 compared with other research arms of the study (i.e., telephone, home visit, or Health Buddy and home visit groups). 14 No significant differences were found among groups in terms of demographic variables. A follow-up qualitative study interviewed a small sample of participants from the parent study (n=13) and found that difficulties in using the device, boring/repetitious content, limited answer options, and inadequate duration of use (either too long or too short) were reasons for nonadherence. 14 However, the follow-up study was limited because only 1 patient from the nonadherent group was interviewed. Reported rates of adherence to the use of HT devices such as the Health Buddy have ranged from 64% to 96%, depending on the technology used, the population studied, the duration of study, and the method used for calculating adherence rate. 19 –23
Within the VA HT program, monitoring of adherence to telehealth devices is routinely performed. Level of adherence is calculated as the total number of sessions completed divided by the total number of all sessions possible, then multiplied by 100 to get the percentage adherence. 24 However, no firm conclusions can be made about either patterns of adherence or subsequent outcomes associated with adherence rates because of methodological weakness and differences in study characteristics and parameters (e.g., different types of devices used, population studied, diagnoses targeted, and duration of studies [rate of adherence is usually better when evaluated in short rather than long durations]). 21,25
Recent studies from the VA HT program have noted that the current lack of information regarding all aspects of patient adherence is a significant limitation to understanding HT impact on outcomes. 26,27 It is important to examine potential predictors of adherence to the use of HT devices so that modifiable factors can be targeted. Furthermore, determining the relationships between degree of adherence and both clinical outcomes and healthcare services utilization rates may enable us to determine the optimal “dose” of adherence or device usage.
The objectives of this study were (1) to examine rates of adherence to the use of Health Buddy over the first 90 days after enrollment in the VA HT program by Veterans over age 65 years with HF, (2) to identify potential predictors of high adherence to Health Buddy use in this sample at different time intervals within the first 90 days, and (3) to determine the relationship between high patient adherence to the Health Buddy at these early time points and both clinical outcomes and health services utilization at 90 days after enrollment. To our knowledge, the present study is the first to examine early adherence to the use of a telehealth device, its predictors, and outcomes in older Veterans with HF enrolled in the VA HT program.
Subjects and Methods
The sample for this study included Veterans enrolled in HT programs in Veterans Integrated Service Network 22 (Southern California and Nevada) between June 1, 2006 and June 1, 2008, who were over the age of 65 years at enrollment and had HF as identified by the Disease Management Protocol, a series of predetermined questions used for monitoring targeted disease exacerbations plus health information specific to their Health Buddy device. 18 The Health Buddy is a store-and-forward asynchronous communication device that allows for in-home messaging and transmission of information. It weighs less than a pound, is approximately 5×9 inches in size, and has four buttons for responses and text management and a high-quality color liquid crystal display screen. It requires only a power supply and a telephone system to operate. 16 The patient is expected to log-on daily and answer questions based on his or her predetermined Disease Management Protocol using the response buttons. After the session is completed, information is transmitted to a secure password-protected Web site where a telehealth care coordinator, usually a nurse, reviews patients' responses, which are prioritized based on preset alerts for specific signs and symptoms. 20 The nurse then contacts at-risk patients for further information, assists them in obtaining needed care, and helps motivate them in maintaining self-management behaviors important in preventing HF exacerbations. 24,25
HT programs in Veterans Integrated Service Network 22, which comprises five individual VA facilities, were identified as belonging to one of three departments: Geriatrics, Ambulatory/Primary Care, or Home Care Services. Two of the facilities had fewer than 10 patients who met the inclusion criteria for this study and therefore were combined for analysis with other facilities having HT embedded in the same department. One facility had 69 patients enrolled in their HT program embedded in Ambulatory/Primary Care. Two facilities with their HT embedded in a Geriatrics Department had 2 and 116 patients, respectively, for a total of 118 patients. The last two facilities had their HT programs embedded in Home Care Services, with 8 and 53 patients, respectively, for a combined total of 61. This disparity in program sizes was due to the fact that each HT program was initiated locally, and the enrolled patient number was dependent on starting date, effectiveness of recruitment activities, and type of patient targeted. 28
This retrospective cohort study used secondary data from two VA databases. After Institutional Review Board approvals were obtained, subjects were identified through the VA Austin Information Technology Center. Data obtained included adherence to the telehealth device, results of a patient satisfaction survey, and perceived health status. The VA National Patient Care Database provided the VA facility and department in which the patient's HT program was embedded, patient sociodemographic characteristics, co-morbid conditions, and data on evaluated health status and health services use.
The Andersen Behavioral Model guided this study of the relationships of predictors and outcomes to early adherence to the use of the Health Buddy. 29,30 This model was chosen because it provides a framework to study potential predictors and outcomes of patient health behavior, including adherence to the use of a telehealth device, which is the focus of the present study. Variables associated with, and therefore potential predictors of, adherence to the use of the Health Buddy included (1) the healthcare system (i.e., department in which the HT program was embedded [Geriatrics, Ambulatory/Primary Care, or Home Care Services]), (2) predisposing (i.e., age, marital status, sex, and caregiver availability [presence of ICD9 codes V60.4 and V60.3]), (3) enabling (i.e., income and availability of non-VA insurance), and (4) need (i.e., Charlson Comorbidity Index) factors related to HT enrollment. Co-morbidity was measured using specific International Statistical Classification of Diseases and Related Health Problem codes (ICD-9 codes) to calculate the Charlson Comorbidity Index using the Dartmouth–Manitoba codes developed by Romano et al. 31
Adherence to the use of the Health Buddy device was defined as the number of days that the patient completed a HT session in each 30-day time frame (TF), with TF 1 being Days 1–30, TF 2 Days 31–60, and TF 3 Days 61–90 after enrollment. Adherence was calculated using the dates that the patient logged in and completed a session. Partial responders were deemed nonadherent for that session. Because the variable was highly skewed, adherence was categorized using an 80% cutoff and coded as either low adherence (0–79%) or high adherence (80–100%) as previously described. 32,33 Because patient dropouts and nonadherence rates tended to be highest early in the course of the intervention, 13,34 only early adherence to the use of the Health Buddy in the first 90 days after enrollment was examined. To determine how adherence changed over time, adherence was studied in 30-day TFs (TF 1, TF 2, and TF 3) as well as longer intervals.
Potential outcomes of adherence examined included (1) patients' perceived health status (i.e., quality of life measured using the Veterans RAND 12 Item Health Survey [VR-12]), (2) evaluated health status (i.e., severity of psychosocial stress, Global Assessment of Function, and mortality), (3) patient satisfaction, and (4) use of health services (i.e., rate of emergency room [ER] visits, Primary Care and Cardiology Clinic visits, hospital admissions, and length of hospital stay). Quality of life measured by the VR-12 survey obtained at the 30th session yielded two scaled scores, a physical health summary measure (Physical Component Score) and a mental health summary measure (Mental Component Score), 35 as previously reported. 36,37 Patient satisfaction was determined by a standard VA HT survey administered via the telehealth device after the 30th session, asking how helpful the care coordination staff and interactions have been and whether the patient would recommend the program to others. 13 Only fully completed VR-12 and patient satisfaction surveys were included in the analyses.
DATA ANALYSES
Descriptive statistics were used to summarize sample characteristics and determine the distribution of adherence at various TFs. To test for significant differences between average adherence during various TFs after enrollment (TF 1, TF 2, and TF 3), a repeated-measures analysis of variance was used with post hoc pairwise test based on a Bonferroni correction.
To determine the relationship between potential predictors and adherence, Spearman's rho was used for continuous variables, and Pearson's chi-squared (or Fisher's exact test if the cells had ≤5 subjects) was used for categorical variables (using high adherence). Subsequently, the relationship of each potential predictor grouping (based on the Andersen Model) to high adherence at different TFs was analyzed using binary logistic regression. Because certain cells for female gender and caregiver availability/living alone status were quite small (some with fewer than 3 patients), neither variable was included in the logistic regression.
To address the relationship between high/low adherence and both clinical outcomes and health services use, Pearson's chi-squared testing was used after the data were transformed to dichotomous variables using their median values. Because of low numbers, measures of evaluated health status and some indicators of health service use (i.e., ER visits, hospital admissions, and length of stay) were dropped prior to analyses. Specifically, only 3 patients had an ER visit, only 5 had any hospitalizations, and only 9 died within the first 90 days after enrollment. Statistical significance was set at p<0.05, and PASW Statistics 18 software (SPSS Inc., Chicago, IL) was used for analyses. 38
Results
The final sample meeting the inclusion criteria for this study was 248 patients with a mean age of 76.4 years. Patient characteristics and demographics are shown in Table 1. The largest percentage of patients (47.6%) was in HT programs embedded in a Geriatrics Department. Subjects were predominantly male, and most either were or had been married and had a caregiver available. Participants were from a wide variety of socioeconomic levels as indicated by the large standard deviation in income. Our sample had a high mean Charlson co-morbidity burden score (5.00) compared with other reported samples of VA patients first hospitalized for HF (1.72–1.89), 39 indicating poorer prognostic outcomes. This difference is likely due to our sample being older (mean age, 76.4 versus 68.1 years of age) and the population of Veterans targeted for enrollment in the VA HT program being sicker (e.g., those with hard-to-manage symptoms, with one or more hospital admissions, or two or more ER visits in the prior year). 40
Description of Predictor Variables
Data are mean±standard deviation values.
The Charlson Index is the sum of the weights for specific diagnoses that the patient carried, which ranged between 0 to 27, with a higher number noting higher co-morbidity burden.
Table 2 provides a description of patient outcomes. Participants reported poorer physical and mental quality of life compared with the younger general Veteran population as evidenced by Physical Component Score (39.0±12.2) and Mental Component Score (35.8±9.3) scores below 50, an expected finding because national data on older Veterans indicate high rates of chronic conditions and a tendency to rate their health as poor or worse. 41 Patients also reported fair satisfaction (score of 1.71±0.52, with 3 being the highest satisfaction) with their HT experience in the first 30 days after enrollment.
Description of Outcome Variables and Adherence
Data are mean±standard deviation values or mean percentages as indicated.
Physical and Mental Component Scores of the Veterans RAND 12 Item Health Survey (VR-12) are weighted and standardized to the overall U.S. Veteran population with a mean of 50 and standard deviation of 10. Thus, the scores of less than 50 indicate that this study sample reported worse quality of life than the general Veteran population.
Individual scores range from 1 (very poor satisfaction) to 3 (very high satisfaction).
Time frame (TF) definitions: TF 1, Days 1–30; TF 2, Days 31–60; and TF 3, Days 61–90 after enrollment.
Table 2 also illustrates the adherence rates over time. Figure 1 illustrates the daily decline in adherence to the use of the Health Buddy over time by days post-enrollment. Analysis of adherence in 30-day TFs (TF 1, TF 2, and TF 3) showed significant differences among the various TF intervals (p<0.05), and average adherence declined progressively over time, with a 27% decline occurring between the first and third 30-day intervals (p<0.05).
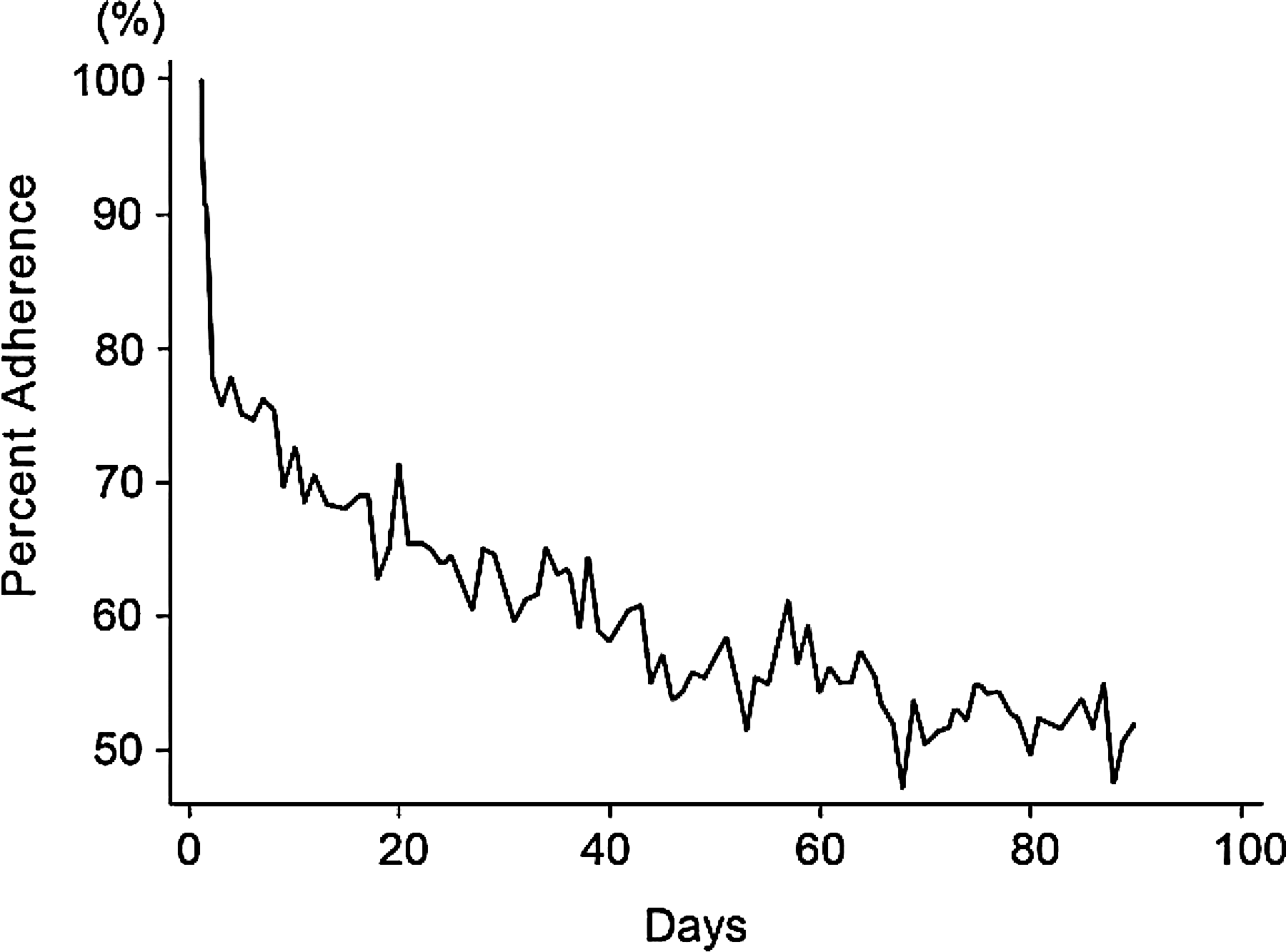
Percentage adherence to the use of Health Buddy by patient day over time (n=248).
The specific department in which the HT program was conducted was a major significant predictor of high adherence in all TFs (all p<0.05). The program embedded in Ambulatory/Primary Care had a significantly higher mean adherence rate in every TF (Table 3). Binary logistic regression showed that patients enrolled in Ambulatory/Primary Care had a 2.2–4.0 greater odds of being adherent (confidence intervals depended on the TFs examined [see Table 3 for details], p≤0.03) at the time intervals studied compared with programs in Home Care Services. Co-morbidity burden showed a weak negative relationship (rho correlation coefficient=–0.13, p<0.05) to mean adherence only in the first 30 days. Other than for the department and co-morbidity, none of the individual or grouped predictor variables examined was significantly associated with adherence in any TF, and no outcome variables were significantly related to adherence in any of the TFs examined.
Mean Days of Adherence to the Use of Health Buddy in Various Time Frames by Department and Odds Ratios
Time frame (TF) definition: TF 1, Days 1–30; TF 2, Days 31–60; TF 3, Days 61–90; TF 1+TF2, Days 1–60; and TF 1+TF2+TF 3, Days 1–90 after enrollment.
Data are mean±standard deviation values.
The odds ratio is the probability of a patient enrolled in a home telehealth program embedded in this department having high adherence (80–100%) divided by the probability of a patient enrolled in a HT program embedded in the Home Care Department having high adherence during the specified TF. The 95% confidence interval is given in parentheses.
p≤0.03.
Discussion
Certain findings in the present study are similar to those reported in other studies of adherence to interventions in patients with chronic conditions. Specifically, patient nonadherence rates tended to be highest early in the course of the intervention, with further gradual dropouts later on. 13,34 In this study, adherence dropped 20% between the first and second 30 days and 7% between the second and third 30 days. In two previous studies in Veterans using the Health Buddy, the reported primary reason for early dropout was patients not wanting to use the device, suggesting a possible need for improved patient enrollment criteria. 13,14 Further study is needed both to determine the types of patients most likely to adhere to daily monitoring by a HT device and to develop new approaches to make daily use of the device more acceptable to patients. 14
Since this study was completed, the VA has developed a Non-Responder Toolkit (November 2008) that is accessible via a Web link from their HT Operations Manual (see
Of interest is that in the present study the department in which the HT program was embedded was a significant major predictor of adherence over all TFs examined. This finding highlights the importance of examining the manner in which HT and other telehealth programs are implemented and administered at the local level. Each VA HT program is unique to its local setting because, although there are detailed national VA HT program guidelines and recommendations on implementation, program operations in local facilities are dependent upon local resources and approaches and the staff involved. 10,42,43
Patients with HF often have multiple other co-morbid conditions that may limit their ability to adhere to a telehealth program. In the present study, co-morbidity was found to have a weak negative relationship with adherence only in the first 30 days. This is similar to findings reported by Clark et al., 44 who found no difference in baseline characteristics, including co-morbidity, between nonadherent and adherent groups of older adults with HF answering prerecorded questions related to their disease.
Finally, this study found that adherence to Health Buddy was not associated with quality of life indices, patient satisfaction, or primary care or cardiology clinic visits in the first 90 days after enrollment. Previous studies have shown an increase in primary care visits after enrollment in the VA HT program, as unmet needs and disease exacerbations were identified, thus decreasing other health service use such as urgent care, ER, and hospital admissions. 45
It remains to be determined how much Health Buddy device adherence is needed to affect outcomes in patients with HF. We could find no previous studies that examined the effects of adherence to HT device use on outcomes in patients with HF. The lack of observed relationships between patient adherence and outcomes in this study may be in part due to both the short TF examined and the reported relatively smaller effect size (0.26) of data monitoring using asynchronous telehealth devices such as the Health Buddy as opposed to the more labor-intensive use of real-time devices such as two-way video (effect size=0.78, p<0.01). 9
Limitations
Because this was a secondary data analysis study, data available for analysis were dependent upon what had already been systematically monitored and collected by the VA HT program and National Patient Care Database. No data were available as to when patients used non-VA services or were on vacation on VA databases at the time of the study. Other variables (e.g., HF signs and symptoms, other behaviors important in the management of HF such as daily weights, blood pressure control, medication adherence, etc.) were not included in the operational definition of the concepts in the Anderson Model used in this study, and thus their relationship with adherence to the use of Health Buddy could not be studied. In addition, patient motivation, self-efficacy in the use of HT devices, HF severity, inpatient status, and reason for enrollment to HT program (e.g., for chronic care versus post-acute care management), which could impact adherence, were not examined. Finally, the study did not extend beyond the 90-day post-enrollment period, which may have been inadequate time for behavior changes to occur that could have affected target outcomes.
Implications for Future Research
Comparing systems and operational factors in HT programs with good adherence versus those with poor adherence may help elucidate causative factors such as differences in staffing, processes, and systems. 46 Prospective longitudinal studies would also be helpful in tracking adherence behaviors over longer TFs. Future studies should also evaluate patient adherence not just to the use of HT devices but also to the behaviors that the devices are used to promote, such as measuring daily weights, responding to questions regarding symptom severity, and improving lifestyle factors, all of which may affect HT program outcomes and effectiveness. 46 In addition, the present study did not examine the characteristics and potential predictors of adherence in those who were only “partially” adherent; it is unclear what predictors may influence this group and how they may differ from those that are either highly adherent or completely nonadherent.
In conclusion, HT programs show potential promise for improving patients' chronic disease self-management and clinical outcomes and decreasing health services utilization. However, further research is needed to improve our understanding of the variations in HT programs and patient characteristics that may impact both adherence and outcomes.
Footnotes
Acknowledgments
We acknowledge the UCLA Doris and Arthur Golden Foundation, whose funding of the statistical and programming services for this study made it possible for this project to be completed. This work was also funded by the VA Health Services Research & Development Service, Veterans Health Administration, U.S. Department of Veterans Affairs (project number LIP 65-121). This material is the result of work supported by the resources and facilities of the VA Greater Los Angeles Healthcare System (GLAHS) and the VA GLAHS Geriatric Research, Education & Clinical Center. Special thanks to the staff of the GLAHS VA Center of Excellence for the Study of Healthcare Provider Behavior for assisting in this project.
Disclosure Statement
No competing financial interests exist.