
Abstract
Introduction
In 2005, the Gulf Coast experienced unprecedented devastation of infrastructure and resources. The Regional Coordinating Center for Hurricane Response (RCC) at Morehouse School of Medicine, Atlanta, GA, was subsequently established to support Gulf Coast recovery. The RCC seeks to promote telehealth solutions emphasizing post-disaster mental health needs. Telehealth is understood as the utilization of electronic information and technologies towards three principal activities: clinical services, education, and administration. 1,2
The RCC's strategic approach is twofold: (1) engage partners as collaborative architects of sustainable telehealth solutions balancing autonomy with efficiency and (2) report on these efforts to advance the understanding of developing telehealth solutions.
A review of telehealth research in the mental health arena reveals several largely descriptive positive efforts. 3,4 Other studies report mixed results with limited generalizability. 5 –9 Still others focused on key development issues, including feasibility, acceptance, 10,11 satisfaction, 12 cost-effectiveness, 13 –16 and comparative effectiveness with face-to-face services. 12,14,17,18 Available evidence suggests telehealth can generate dependable results, produce good satisfaction, lead to improved clinical status, 12,19,20 and offer significant value (e.g., capacity) in the care of injury, disease, and mental illness. 21
Despite evidence of effectiveness, telehealth remains largely at the periphery, hampered by an array of challenges 22 including inadequate resources, 3 provider resistance, 3,14,23 workflow integration, 3,4,24 –26 regulatory and technology issues, 3,15,18,20,21,23,26,27 diagnostic fidelity, and confidentiality. 20
The experiences of RCC partners constructing post-disaster telehealth solutions offer valuable development insights spanning a range of organizations, intentions, implementations, and outcomes. We sought to document this diverse knowledge base using a qualitative research framework to identify shared challenges, successful tactics, and recommendations for scalable sustainability.
Subjects and Methods
Data were collected from key informants across Alabama, Mississippi, and Louisiana and with national organizations with Gulf Coast recovery interests. Eligible informants represented all organizations engaged by the RCC regardless of whether collaboration resulted. Participating informants were categorized by their roles (i.e., administrative, advocacy, clinical, or technological). Semistructured interviews were conducted through videoconferencing or telephony if videoconferencing was unavailable. Open-ended questions queried personal and organizational experiences with telehealth across all stages of consideration, implementation, utilization, and maturation. Follow-up probes elicited detailed information on organizational structure, finances, technology, policies, protocols, perceptions, barriers, benefits, and outcomes.
Data Collection
Forty-nine potential informants were invited to participate. Written consent was obtained prior to interview. Interviews averaged 1 h for informants actively engaged in telehealth and 30 min for those not engaged. Two facilitators conducted each interview and reviewed interview transcripts for completeness and accuracy.
Data Analysis
The research design was qualitative-descriptive. 28,29 Interview transcripts formed the dataset. Structural coding methodology was used with Atlas.ti6© (ATLAS.ti Scientific Software DevelopmentGmbH, Berlin, Germany) qualitative analysis software 30 to label and index data related to each interview question. 31 Following collaborative agreement on code relevance, eight study analysts generated a master list of codes and subcodes highlighting relevant telehealth themes.
Three analysts individually coded each transcript by interview question and master code list. Independently coded transcripts were merged and collaboratively reviewed to verify consistency and resolve discrepancies. This produced “consensus-coded” transcripts for formal query. Analysts reviewed queries and identified relevant themes as the basis for the study's report. Twelve informants willing to review and validate conclusions formulated comments on the report. 29
Results
Key informants represented 23 of the 24 organizations approached by the RCC (95.8%). Thirty-eight informants participated (77.6%), including 17 administrative, 8 clinical, 9 technical, and 4 advocacy stakeholders. One administrative informant's interview rendered no relevant telehealth information and was excluded. More than half of the respondents (n=22, 58%) represented organizations in Louisiana, seven respondents (18%) represented organizations in Mississippi, and three (8%) represented ones in Alabama. Four respondents represented advocacy organizations at the national (n=3) or regional (n=1) level, and two respondents were located in Georgia and Oregon, respectively.
Seven key elements critical to telehealth success were identified from informants' accounts (Fig. 1). Table 1 summarizes relevant informant experiences and recommendations, and Table 2 highlights representative quotes clarifying each key element.
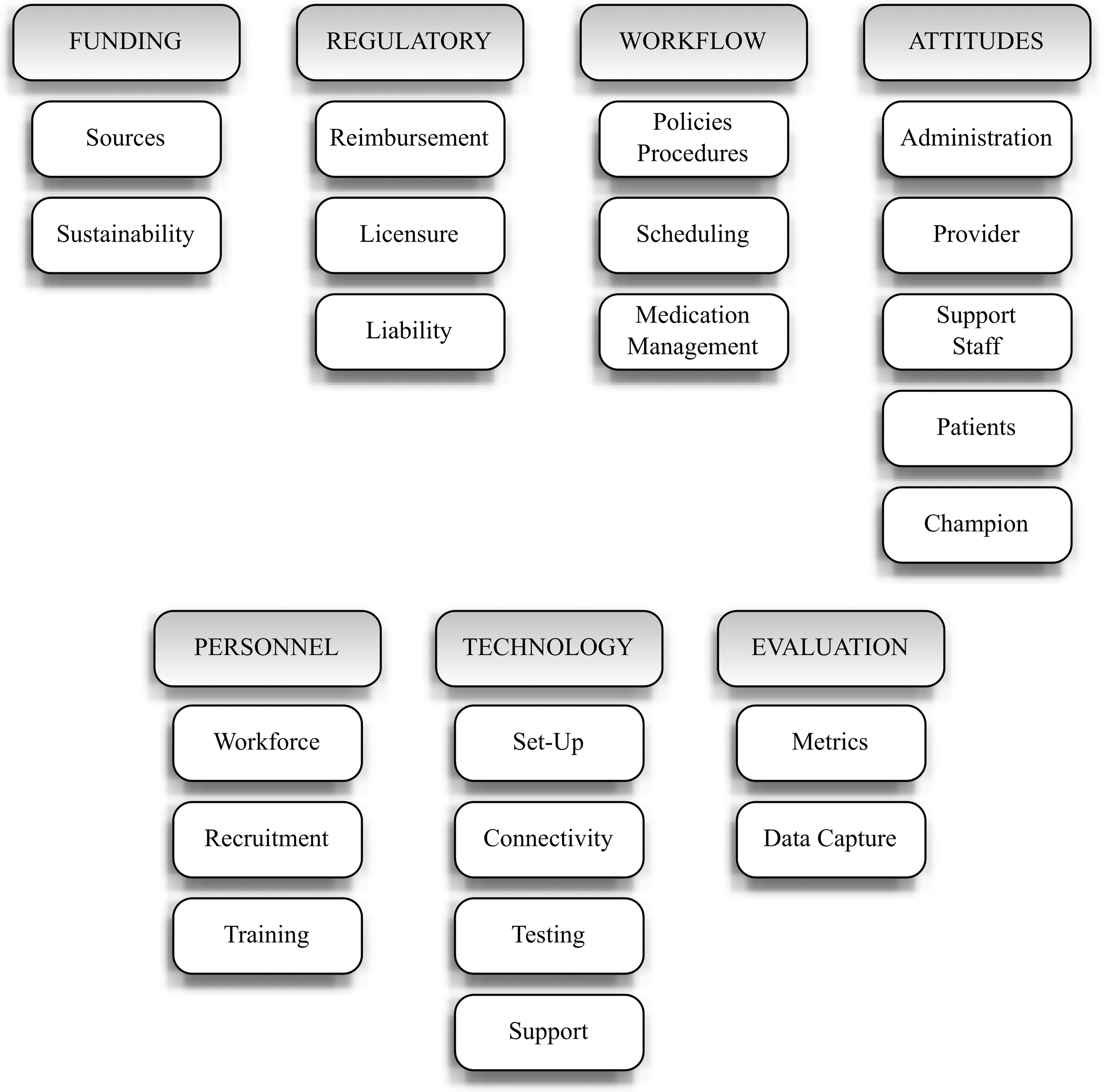
Key elements in telehealth development.
Key Informant Experiences with Telehealth Development
Signals a critical component.
EMR, electronic medical record; IT, information technology; TH, telehealth.
Key Elements and Representative Quotes
Attribution of quotes is given by (transcript number paragraph: line).
BMI, body mass index; RCC, Regional Coordinating Center for Hurricane Response, USA, University of South Alabama.
Funding
Inadequate funding was reported to impact both engagement and implementation (Table 1). Most programs received external funding to acquire videoconferencing equipment. Funding, however, was often inadequate to cover the full cost of implementation, secure technical support, and cover staffing requirements. Informants also reported unanticipated expenses following implementation (e.g., client transportation needs). The most vulnerable telehealth initiatives were completely reliant on external funding. Well-defined funding commitments were evident where telehealth was an integral part of the organization's strategic model.
Regulatory
Informants consistently identified three regulatory challenges: reimbursement, licensure, and liability (Table 1).
Reimbursement is a longstanding challenge impacting telehealth viability, particularly for organizations serving the uninsured. Providers reported difficulty receiving telehealth reimbursement (regardless of payer), variability of reimbursement across states, billing complications at both ends of the encounter (due to limits on co-pay splitting), and complications with reimbursement for specialists and sub-specialists.
Provider licensing and credentialing were pervasive impediments to telehealth implementation. Ensuring that providers are authorized at both the provider and patient sites can be burdensome. To ease this burden, informants recommended a national telehealth licensure mandate, including expedited disaster protocols specifying longer authorization terms given the longitudinal efficiencies of telehealth presence. Absent telehealth licensure provisions, providers must maintain licenses in states where both the providers and patients are located. Informants also highlighted the importance of appropriate nursing credentialing for personnel who facilitate the telehealth encounter with prescriptions, medication coordination, and follow-up scheduling.
Liability concerns were not widely reported and depended on the nature of the program and state-specific liability caps. Some program directors expressed interest in better guidance on telehealth service coverage. Reported measures taken to ensure coverage included seeking attorney advice on policy adjustments.
Workflow
Three critical workflow elements were identified: policies and procedures, scheduling, and medication management (Table 1).
Informants discussed the lack of guidance related to established telehealth policies and procedures resulting in the novel development of manuals for many organizations. Other workflow challenges included (1) coordinating telehealth policies and procedures across organizations, particularly with screening, scheduling, managing medications, and co-managing patients, and (2) identifying skilled professionals responsible for maintaining confidentiality, facilitating encounters, and responding to emergencies, whether clinical or technologic.
Storing and sharing clinical records including personal health information were considered a challenge. Electronic health record solutions, ideally with multimedia capabilities, were deemed essential to telehealth success. Absent an electronic health record, documentation was faxed to remote sites despite recognition of potential personal health information security risks.
Scheduling was one of the greatest procedural challenges identified. Clear communication protocols between sites were deemed critical. Patient “no shows” had a deleterious impact at both ends of the telehealth encounter. Managing these missed appointments was particularly difficult when the only service option was via telehealth. Strategies used to ensure appointment compliance included phone reminders, letters, and other assistance (e.g., childcare, transportation).
Managing medications was also challenging where on-site providers were not authorized to write controlled substance prescriptions. Telehealth providers reportedly used overnight delivery of hand-written prescriptions when necessary.
Attitudes
Attitudes toward telehealth implementation were a consistently reported theme, particularly provider resistance and stakeholder buy-in. Informants identified several contributors to provider resistance, including limited understanding, negative preconceptions, dislike of technology, misaligned expectations, limited training opportunities, preference for traditional encounters, complacency, fear of revenue loss, and fear of being watched or recorded. Strategies suggested for addressing provider resistance included exposure to successful telehealth programs and early provider inclusion in the development process.
Stakeholder buy-in was considered crucial to telehealth success. Administrator buy-in was recognized as broadly impacting telehealth implementation, including adequate physical space, funding support, and staff assignment. Other essential stakeholders included nursing, information technology (IT), and administrative staff. The importance of patient and family acceptance was also noted given patient reports of disliking the technology and concern about equivalence with traditional services. Provider “champions” were repeatedly mentioned as essential to telehealth development as they are noted to attract others to support programmatic success.
Personnel
Gulf Coast workforce issues presented a formidable post-disaster challenge to telehealth development. Informants reported having no personnel capacity to dedicate to telehealth implementation. They described personnel working well above capacity to maintain routine operations, leaving little time for telehealth development. Recruiting certain specialists (e.g., psychiatry) was a noted challenge due to both limited acceptance of telehealth and global supply shortages. Recruiting was complicated by the need to clarify legal, financial, and clinical considerations. Training of personnel on the use of telehealth equipment was challenging because of limited time, funds, and resources. Frequent personnel turnover also created the need for perpetual training, which threatened program maturation.
Technology
Technology challenges were frequently identified (Table 1). Informants indicated that lack of IT support delayed or discouraged telehealth implementation. Smaller clinics do not typically employ IT specialists, presenting both implementation and maintenance difficulties. In some small communities, it was difficult even to find IT specialists. Organizations with IT specialists sometimes fared no better because of lack of videoconferencing expertise and limited vendor support.
Connectivity issues were pervasive. Lack of adequate bandwidth and funding to increase it was reported, predominantly in rural communities. Informants acknowledged that current federal, state, and private initiatives expanding broadband coverage would eventually resolve this challenge. Some organizations implemented satellite connectivity solutions, but transmission quality was found to be inadequate and costly. Another noted challenge was network architecture. Closed networks, firewalls, and equipment incompatibility hampered successful connections. Poor transmission quality was broadly deemed detrimental to telehealth success.
Equipment not performing as expected was another reported challenge. Moreover, limited time and resources to resolve equipment challenges only compounded the issue and ultimately discouraged telehealth use. Informants recommended strong vendor support and thorough equipment testing to minimize operational difficulties that jeopardize telehealth adoption. The issue of catastrophic equipment failure led some informants to recommend back-up equipment and emergency protocols to avoid service interruption and dissatisfaction. Attendant capital costs for back-up equipment, however, further stress a financially vulnerable telehealth model.
Evaluation
Participating key informants occupied different developmental stages from consideration and implementation to utilization and maturation. Evaluation practices, therefore, varied from nonexistent to comprehensive. When asked about telehealth evaluation, informants largely focused on clinical benefits and administrative implications. Commonly reported telehealth metrics for clinical assessment included (1) provider and patient satisfaction, (2) workflow output, and (3) patient outcomes. Administrative metrics included quantification of the efficiency and capacity of telehealth operations, as well as cost analysis (direct, indirect, capital, and operational costs). The electronic health record was widely noted as key to collecting necessary evaluation data.
Discussion
The RCC's initial focus sought to address unmet mental health service demand by developing autonomous, useful, and sustainable telehealth solutions. The resulting collaborations emerged in multiple environments with varied program objectives, which reflected specific organizational priorities (e.g., from primary care to human immunodeficiency virus education). Within this heterogeneous context, our informant reports take on additional significance by building upon existing knowledge found largely in single-program implementations within telehealth.
Seeking to advance our collective understanding of telehealth across all RCC collaborations, however, led to our study's methodological approach. Our study presents firsthand reports of post-disaster telehealth development experiences across three states from a diverse group of organizations. Our qualitative research approach distills disparate experiences into a common knowledge base useful in program strategy development, but also essential in establishing a dimension of “familiarity” necessary for telehealth to move into the mainstream. 23
The seven key elements identified can be found among previous studies, but often independently with support from single programmatic efforts. 3,4,32,33 The developmental guidance offered in this analysis possesses broader applicability for a variety of organizations that are considering telehealth given similar challenges of unmet need with limited resources.
Among the key elements identified, funding is both a catalyst and a fuel fundamental to telehealth success. Informant experiences underscore that funding considerations require organizational commitments, including support for IT. 3 It is further recognized that cost-effectiveness can only emerge once telehealth activity scales beyond part-time single-solution applications. Scaling strategies range from maturing all three Health Resources and Services Administration–defined activities to shared resource utilization across multiple specialties and organizations. 34
Informant responses emphasize that sustainability hinges on revenue generation. Currently, Medicaid telehealth reimbursement rules vary across states. At least 27 states report some degree of telehealth reimbursement. 35 Medicare restricts which settings qualify as originating sites and pays for a limited number of telehealth services. Clinical psychologists and social workers, however, cannot currently bill for telehealth psychotherapy under Medicare. 36 Private payers generally do not universally reimburse for telehealth services, although some are beginning to follow public payers with selected services. Telehealth reimbursement rules are predicted to eventually match traditional payment mechanisms but will require additional evidence supporting telehealth effectiveness. 37
Informants confirmed the pervasive licensure challenge noted in the literature when seeking specialists beyond state borders. 15,21,23,38,39 Currently, 27 states and the District of Columbia have taken no explicit action regarding interstate telehealth licensure. These states rely upon broad “practice of medicine” statutory clauses and require unrestricted licensure if the therapeutic relationship involves the state in question. Although not explicit, these clauses could be construed to consider telehealth care as falling within the practice of medicine. 40 The Health Care Safety Net Act of 2002 authorized incentive grants for state licensing boards to assess interstate cooperation and promote policy initiatives to reduce telehealth barriers. 41 The Federation of State Medical Boards also supports a special-purpose license to cover telehealth encounters nationally. To date, only 10 states have adopted some version of this model, and state portability remains an ongoing advocacy issue. 42 In contrast, the Nurse Licensure Compact (NLC) proactively supports telenursing. 43 The NLC permits interstate practice for nurses licensed in their home NLC state, provided the nurse acknowledges being subject to each state's regulations. At present, 23 states have joined the NLC. 44 The Advanced Practice Registered Nurse Compact 45,46 developed in 2002 is similar to the NLC and promises further promotion of advanced telenursing practice once implemented.
Informant liability concerns were notably less prominent. Telehealth malpractice policy modifications continue to be specialty dependent and made on a case-by-case basis. 34 Provider liability concerns may also contribute to limited adoption rates found among RCC collaborators. 13
With regard to telehealth workflow, informants repeatedly echoed the importance of clear policies and procedures. 3,4,20 The expressed need for telehealth manuals including templates has been previously recognized. 47,48 The rapidly evolving nature of telehealth creates new challenges and opportunities in developing, distributing, and updating such resources.
As previously reported, 3,4,20 informants confirmed that buy-in at all levels, including patients, is key to telehealth development success. Integration of telehealth into routine operations is noted to be no different than incorporating any new organizational procedure. 49,50 As such, there is notable value in utilizing “champions” throughout the developmental process. 51 Sustained acceptance of telehealth is also supported by incorporating formal telehealth skills training to providers and support personnel alike. 52,53
Our study and others underscore the need to appropriately staff telehealth operations with dedicated and adequately trained personnel, including effective IT support. 3,20,26 Attempting to implement without these provisions risks programmatic failure. Strategies for organizations lacking IT resources might include partnerships with larger institutions employing IT specialists or cost-sharing among organizations. 54
Another technological need identified involves system interoperability. 3,21,39 The 2009 HITECH Act 55 addresses this challenge with an unprecedented investment supporting the deployment of critical technologies (e.g., electronic health record) necessary for telehealth maturation. Also of note is H.R. 2068, the Medicare Telehealth Enhancement Act of 2009, introduced by Congress “to improve the provision of telehealth services under the Medicare Program, to provide grants for the development of telehealth networks, and for other purposes.” 56 This bill highlights governmental interest in telehealth service expansion, telehealth provider credentialing, and provisions for home-based telehealth access. Overall, legislative attention appears to be growing toward realizing the promise of telehealth solutions.
Consideration of this study's results should be balanced against several limitations. First, eligible study informants represent a convenience sample of only organizations approached by the RCC. We did not identify other organizations independently pursuing telehealth following the 2005 hurricanes. Second, sample weighting plays out in several ways. Informant geographic distribution reveals a preponderance of Louisiana-based organizations attributed, in part, to the RCC having more familiarity with the Louisiana healthcare landscape. Furthermore, the RCC strategy of approaching only those organizations with strong interest in telehealth resulted in sample weighting toward organizations that ultimately engaged in telehealth. In addition, the variability in the number of informants by organization was related to program maturity and resulted in sample weighting toward mature organizations. Lastly, study results may not generalize beyond post-disaster circustances within the southeastern United States. Although we believe the reported insights hold broader value for vulnerable populations with unmet service needs, it remains possible that the telehealth experiences reported herein may be influenced by variables unique to a post-disaster Gulf Coast.
Conclusions
The Gulf Coast, overwhelmed by disaster, exposed an untenable situation of need far outpacing resources. In response, the RCC seized an opportunity to support telehealth adoption in order to maximize the utility of scarce mental health resources. Within these efforts, a wealth of data pertaining to telehealth development was captured, demonstrating that as telehealth redefines the provider–patient relationship, so must it redefine stakeholder roles, environments, and protocols. 57,58
But more than redefinition, widespread adoption requires cultivating the familiarity with telehealth revealed within our informants' reports. 22,59 We believe that the insights provided by key informants, structured as key elements, might strategically assist other organizations to benefit from rather than repeat lessons learned in early telehealth development. These key elements are offered as a developmental framework to guide implementation efforts. 60
Technology has transformed the way we interact with each other. And though it may seem to have happened overnight, widespread acceptance and usage remain elusive and require recruiting those comfortable with the past—into the future. A far-reaching telehealth adoption strategy will require more than overcoming specific barriers. It will take time, persistence, and vision to move from replicating historic efforts to building upon them.
Footnotes
Acknowledgments
This qualitative study was supported by funds from the Regional Coordinating Center for Hurricane Response at Morehouse School of Medicine under the Office of Minority Health, Department of Health and Human Services (CFDA number 93.004) and grant number MPCMP061011-01-07. Key informants from the following sites permitted us to analyze their interview responses: All Healers Mental Health Alliance; Alta Pointe Health Systems; Children's Health Fund; Coastal Family Health Center; Counseling Solutions; Louisiana Department of Health and Hospitals; EXCELth, Inc.; Louisiana Primary Care Association; Louisiana Public Health Institute; Louisiana State University TeleMed; Mercy Family Center; Mississippi Primary Care Association; Morehouse School of Medicine; New Orleans Health Department; Rapid Evaluation and Action for Community Health in New Orleans, Louisiana; Southern University and A&M College; St. Anna's Episcopal Church; Trinity Counseling and Training Center; Tulane Community Health Center at Covenant House; University of Mississippi Medical Center; and University of South Alabama. Yolanda Dunbar-Johnson, LCSW-BACS, MS, Heidi Sinclair, MD, MPH, Douglas Walker, PhD, and Jeb Weisman, PhD, provided thoughtful comments on drafts of this manuscript. Crystal A. Kinnard, MEd, provided administrative support.
Disclosure Statement
No competing financial interests exist. T.J.K. and M.I.A. are responsible for study concept and design and for study supervision. S.L.E., M.S., A.H.N., and K.M.B. are responsible for data acquisition. M.I.A., S.L.E., M.S., M.L.I., A.H.N., K.M.B., and R.D.F. are responsible for data analysis and interpretation. T.J.K., M.I.A., R.D.F., S.L.E., and M.L.I. are responsible for manuscript drafting. T.J.K., M.I.A., S.L.E., M.L.I., M.S., A.H.N., K.M.B., R.D.F., and A.V.B. are responsible for manuscript revision for important intellectual content. T.J.K., M.I.A., S.L.E., M.S., M.L.I., A.H.N., K.M.B., and R.D.F. are responsible for qualitative analysis. M.I.A., S.L.E., M.L.I., M.S., A.H.N., K.M.B., and R.D.F. are responsible for administrative, technical, and material support.