
Abstract
Introduction
The need to consistently and accurately represent the information contained in medical records is defining the way in which models for semantic content of medical data are being designed and developed. This is reflected in efforts such as the Working Group 3 of the ISO/TC 215 (
In this context, asynchronous or store-and-forward telemedicine networks providing remote diagnosis services for examinations of different kinds can play an important role in the continuous acquisition of reliable epidemiological data because they can encompass a wide area and gather data not only from major hospitals, which can be oriented toward more complex pathologies, but also over a wide range of primary healthcare facilities and small hospitals. This potential capability of such a system is able to deliver a more detailed and reliable panorama of the morbidity distributions in a large population. 2 A desirable feature is the capacity to efficiently perform data mining and correlate data stored in medical reports. It serves not only the medical needs to represent and detail the scenario in the specific telemedicine network in which it operates, but also to help public health managers on the smart allocation of resources. 3,4
The Digital Imaging and Communications in Medicine (DICOM) Structured Reporting (SR) standard offers an interesting solution for the structured, semantic-related representation of medical data that, because of its structure, can be used in a much broader context than the originally intended radiology field. 5 This approach has the advantage extending the application spectrum of a picture archiving and communication system (PACS) so that it may provide the back-end of a typical asynchronous telemedicine system. 6
The main difficulty in implementing and applying the DICOM SR is the necessity to consider the combination of different customization factors necessary to provide the end users with a user-friendly structured reporting application, while handling the complicated DICOM SR objects transparently. 6 One issue in electrocardiography (ECG) that has been discussed for a long time is the lack of a standardization of terminology in ECG findings reports. 7 In order to improve a semantic interoperability mechanism, Surawicz 7 discussed how to increase the accuracy of electrocardiogram interpretation and stimulate the interest of the interpreters. The author claimed “the objective is to increase the accuracy of the ECG diagnosis report and possibly be of more interest to the overreaders by providing opportunity to refresh and update their knowledge of electrocardiography.” There are numerous factors that have to be taking into account—including the motivation of the interpreting cardiologists—to provide tools that facilitate the production of standardized findings reports without oversimplification and consequently loss of accuracy in the interpretation.
In this article we describe the design of a structured document model compliant with the DICOM SR to meet the demand for large-scale telemedicine networks. We also present the development of a specific structured vocabulary in cardiology context in according to standards and guidelines of the Brazilian Society of Cardiology (BSC). This article also describes the fundamentals and some results obtained and details the development and implementation of the DICOM SR application.
Our work differs from previous approaches because we apply systematically DICOM SR to achieve detailed findings reports in ECG in the context of a large-scale public telemedicine network. 2,8,9 This allows, for instance, the morbidity traceability in a multimodality asynchronous telemedicine network using structured vocabularies as the report foundation.
Materials and Methods
In this section we review briefly a few key concepts, which we consider important on the context of this work, and give the background of our study.
DICOM SR
The DICOM SR is an extension of the DICOM medical imaging/teleradiology standard, published in 2000. 5,10 A DICOM SR document consists in a semantic network composed by a sequence of nodes called Content Items. The nodes in this network are connected through a set of semantically labeled hierarchical relationships such as “CONTAINS.” 9
DICOM SR defines an information architecture designed to code and exchange clinical data. It provides support for a structured writing format by adding precision, clarity, and validity to a clinical document, even if it was originally designed for being used in the context of radiology information systems. Documents in DICOM SR format can be used anywhere where a formalized and structured description of medical records is desired. 5
In the last decade several studies aiming to the deployment of the DICOM SR in health institutions and their professionals' routine were published. Riesmeier, as noted by Clunie, 10 described the prototype of an SR editor and viewer using DICOM SR. This work resulted in a functional prototype that extends some features of the OFFIS DICOM library, resulting in their incorporation into an application called DICOMscope. 11
Bortoluzzi et al. 12 developed a prototype of a structured report editor called the Cyclops DICOM SR Editor. This editor was also able to generate templates for different DICOM modalities.
Hussein et al. 6 illustrated the challenges when implementing DICOM SR support for PACS workstations. Their work resulted in a prototype of an editor and viewer for structured reports integrated with a teleradiology system called CHILI. 6
Arnold et al. 13 described the prototype of a Web-based SR system for onsite–offsite clinician communication. The prototype presented is a Web-based application with PACS integration where report issuing is also based on the DICOM SR standard, but using only plain text as input. From these studies, only Hussein et al. 6 went beyond the mere prototype stage, but its application remained restricted to regional teleradiology networks.
Other studies described the need of index clinical information using proper vocabularies. In 1998, Korman et al. 14 already discussed this need by publishing a proposal of a minimal standard terminology necessary for applying DICOM SR in gastrointestinal endoscopy. In this study, the authors stated that, despite advances in technology used by video endoscopy professionals, only few advances have been made to improve the quality of the information related to the examination. In 2010, Welter et al. 15 pointed out that the use of DICOM SR provides interchange with PACS workstations, offering the possibility of further data mining.
Santa Catarina State Integrated Telemedicine and Telehealth System
The Santa Catarina State Integrated Telemedicine and Telehealth System (STT/SC, in Portuguese) is a large-scale public telemedicine and telehealth network, operating since 2005 as a state government-sponsored initiative in the southern Brazilian state of Santa Catarina. This network, which now connects 401 healthcare institutions in 291 municipalities throughout the state and is still growing, offers a varied palette of synchronous and asynchronous services to assist the patient's health, such as telediagnosis, second opinion, real-time, and collaborative reporting and continuous education, among other services, performing an average of 75,000 examinations/month. 8,9,16 STT/SC users have access to DICOM imaging and signal studies through specially developed Web-based and smartphone software platforms accessed via an integrated portal that enables visualization, analysis, discussion, and report writing from examinations. 8,9,16
Structured Vocabularies
Structured vocabularies are collections of terms, organized according to a methodology in which it is possible to specify the relation between concepts with the purpose of facilitating the access to information. Structured vocabularies normally have formal semantics and are usually described hierarchically. 17 These vocabularies can be used by DICOM SR implementations to define the semantics of individual content items. A particular implementation can use dynamically one or more vocabularies. In our work we used two specific medical vocabularies: the health sciences descriptors vocabulary (DeCS), as a source for clinical information descriptors, 17 and a special vocabulary developed from clinical practice guidelines of the BSC. 18
Health sciences descriptors
DeCS 17 was created by the Pan-American Health Organization from the medical subject headings (MeSH) 19 vocabulary, in order to allow the use of a common indexed terminology in three languages (English, Portuguese, and Spanish). This vocabulary provides a consistent and unique environment for information retrieval regardless of language. 9,19 The DeCS vocabulary presents an extra axis of descriptors coding public health concepts. DeCS makes use of a hierarchical structure in such a way that, from a specific descriptor, it is possible to reach its ancestor, descendant, and siblings.
Guidelines of the BSC and the Cyclops SR vocabulary
Cardiology reports, in particular ECG reports, in most cases present the same basic textual structure: findings description+findings localization. Unfortunately, in some cases—especially because of software deficiencies—physicians do not have any auxiliary tools or guidelines to follow when writing a report. 9
Aiming to standardize and support the writing of ECG reports, in 2009 the BSC published a document called “Guidelines of the Brazilian Society of Cardiology for Reviewing and Writing Electrocardiographic Reports.”
18
In 2010, the Santa Catarina State Health Office, in order to standardize the ECG findings reports produced by the STT/SC, created a commission to propose technical solutions that possessed the potential to allow the automated real-time production of morbidity statistics with the highest level of detail. Because the BSC had already published the mentioned guidelines, the commission decided to develop a structured vocabulary on the basis of these guidelines, which was called BSC/CSR (
Results
Creating a Dicom Structured Report from Structured Vocabularies
The process of customization or implementation of DICOM SR in a clinical environment consisted in three major aspects: (a) the SR presentation (viewing and printing), (b) the user interface, and (c) the data structure used to store the report information as well as the algorithm responsible for handling the data. 9 Our approach was developed to be able to cover these three aspects and an additional aspect, involving data-mining capabilities. Taking the aspect of data mining and also the quality assurance of reports written in the STT/SC as key factors when implementing this methodology, the report information foundation was built in order to be capable of using structured vocabularies such as MeSH 19 and DeCS 17 in a transparent manner.
On this proposed model physicians use the interface not only to write the report in a natural plain-text style, but also to link and attach one or more descriptors to the final report. For most DICOM modalities, medical reports are structured using three predefined fields: “Study Description,” “Findings,” and “Conclusion.” At the end, plain-text information and descriptors are automatically attached to the DICOM SR file.
Electrocardiograms encompass approximately 70% of the total number of image and signal examinations performed asynchronously and stored on the STT/SC database, generating a high demand for the physicians who write ECG reports. After a detailed study of the ECG reports previously written in plain-text style and the document “Guidelines of the Brazilian Society of Cardiology for Reviewing and Writing Electrocardiographic Reports,”
18
we developed a specific structured vocabulary in addition to the DeCS vocabulary. This project decision took into account the “Guidelines of the Brazilian Society of Cardiology for Reviewing and Writing Electrocardiographic Reports”
18
and a list of BSC/CSR-based descriptors suggested by a group of experienced cardiologists who work in the STT/SC; this vocabulary was called BSC/CSR (see
The vocabulary uses a unique identifier as its index key. Connected to the unique identifier are one or more descriptors and a full description. The unique identifier is used when writing a report without making use of plain-text style; the physician simply selects which descriptors to link to the report resulting in a completely standardized ECG report without syntactic or conceptual inconsistencies. 9 Figure 1 shows the structure of a BSC/CSR descriptor linking the “Unique Identifier” with description, descriptor, and descriptor synonym.
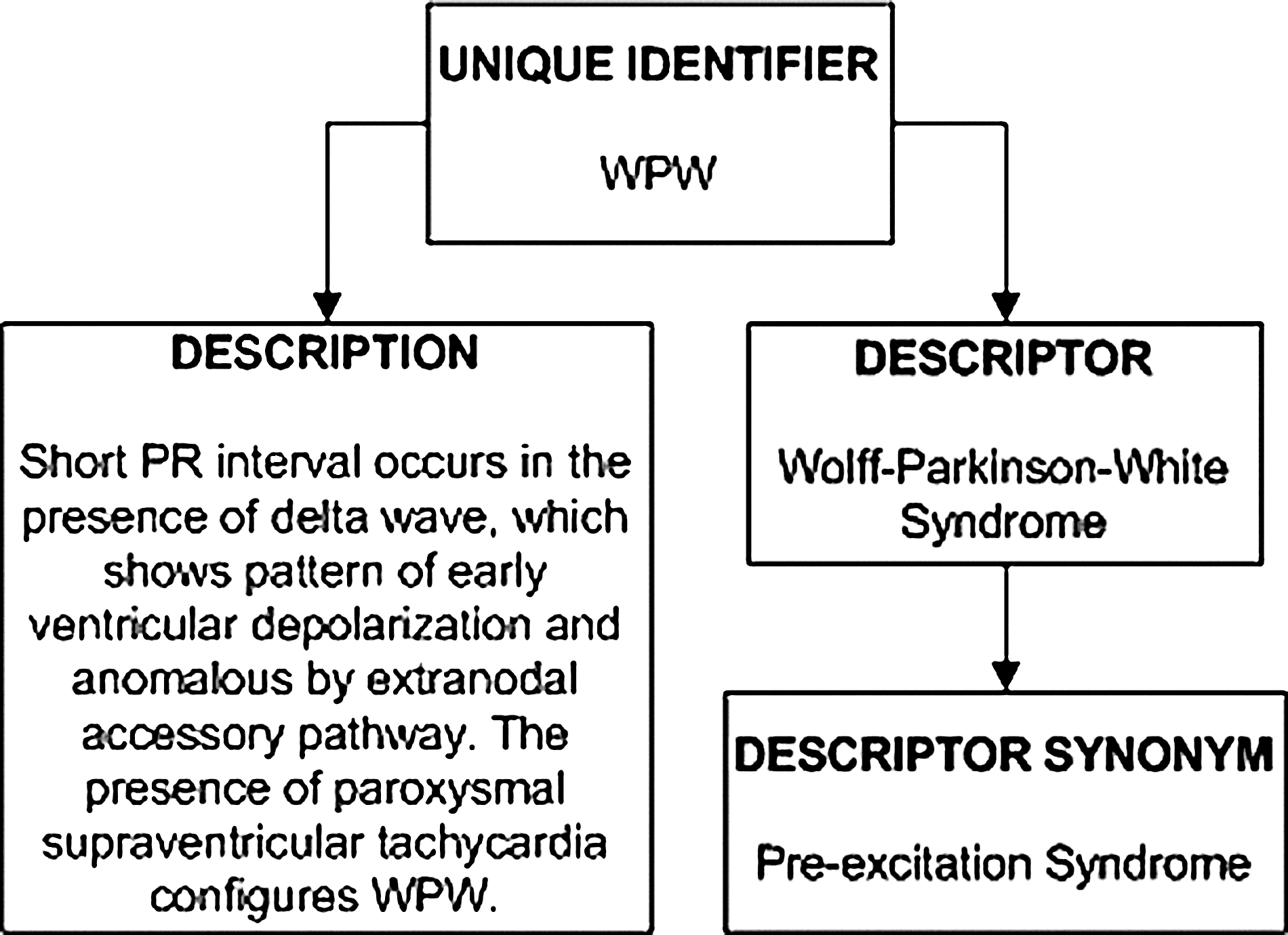
Structure of a Brazilian Society of Cardiology/Cyclops structure reporting descriptor. WPW, Wolff–Parkinson–White.
Once we established the DeCS and the BSC/CSR descriptor as the set of vocabularies to be used as the set of building blocks for the report, the development of the main application (CSR) was started. This application is responsible for providing a user-friendly interface for the physician, interpreting the input text and correctly encoding it in the structured document, connecting to the DICOM database and server, communicating with third-party software components, rendering the final report, and retrieving the report information. 9 Initially the CSR was developed as a Web-based application. Later an application for smartphones was also developed.
Initially the CSR interprets the text entered by the physician in a user-friendly interface. In this step CSR follows the guidelines established by the DICOM standard, as shown in Figure 2, in order to compose a well-formed XML template. The next step is the encoding process of the newly formed XML template using tools called xml2dsr and dsr2html that convert the XML to a DSR and HTML document. 20 Then CSR translates the generated html file to a specific application, which stores the generated files (.xml, .dsr, and .html) in the DICOM database and in an object-relational database.

Example of a computed tomography DICOM structured reporting template. CSR, Cyclops structure reporting; IV, intravenous.
This process consists in input data through a transparent interface to the user, where the doctor fills in the applications and makes standard forms, separated from fields that characterize the study type, until diagnosis and conclusions from examinations report. The final report proper, encoded as shown in Figure 3, is now linked to the examination's images, and its information is available for analysis anytime by the referring physician.
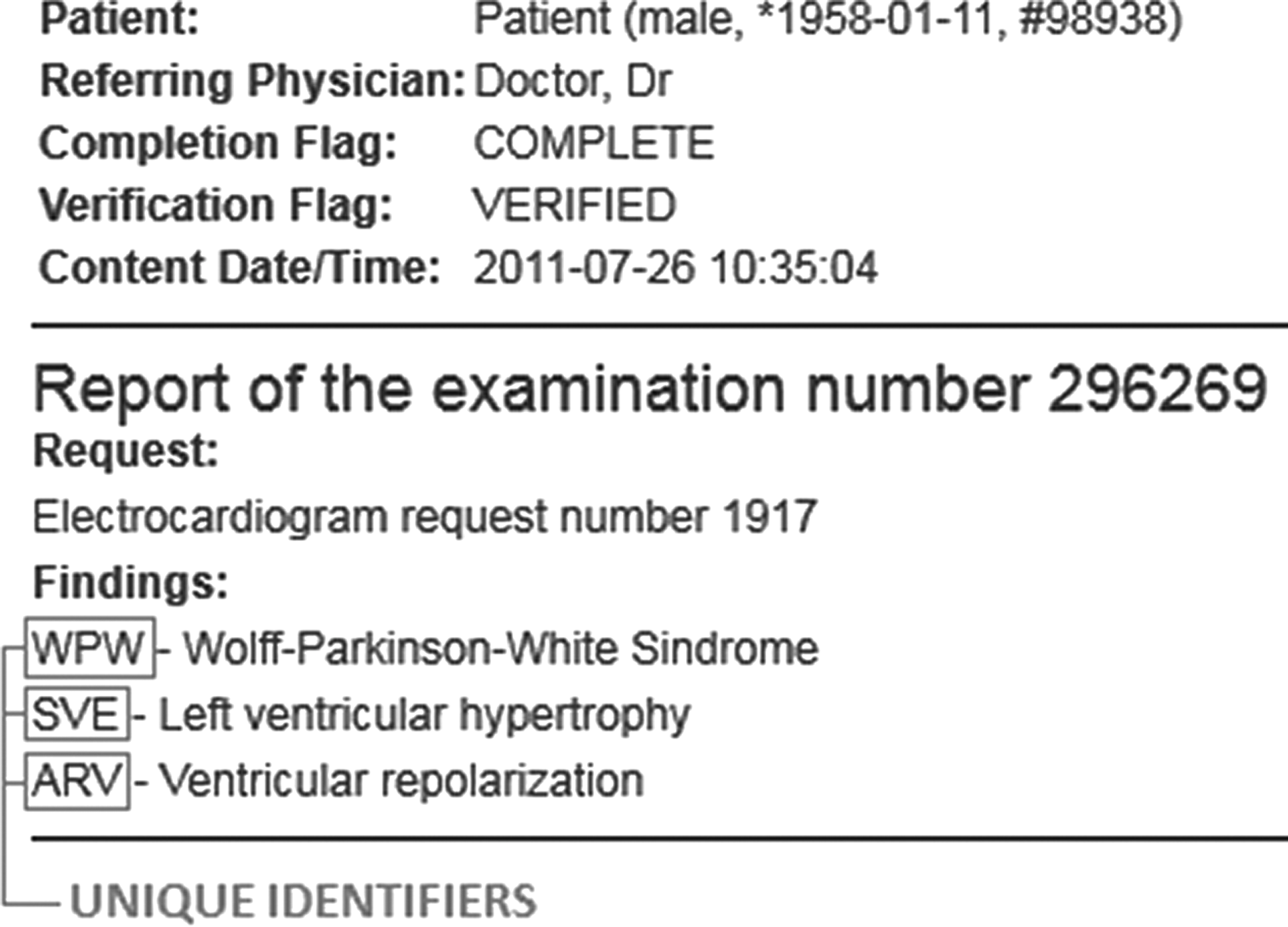
Example of a final electrocardiography report with unique identifiers indexed.
At this point there are several cross-references between the examination and the report. The most important references for the data-mining and traceability process are the descriptors linked to the report by the CSR application. Through the report indexing process we now have descriptors of different vocabularies working as indexes of the report's content. These indexes make it possible to perform data mining, using the report information. It is also possible to compare one or more reports with some other report to establish a relation.
Figure 4 shows the complete report writing workflow of our methodology, starting with the choice of the input interface to the exchange of information between the DICOM server/database, the CSR, the structured vocabularies, and the database using a Web server as the connector. We create a clinical information entry properly indexed, where the indices are unique identifiers for each structured vocabulary. These indices make the analysis and data-mining process simpler, more integrated, and more error-free compared with the storage processes of plain text and consultations by key words.
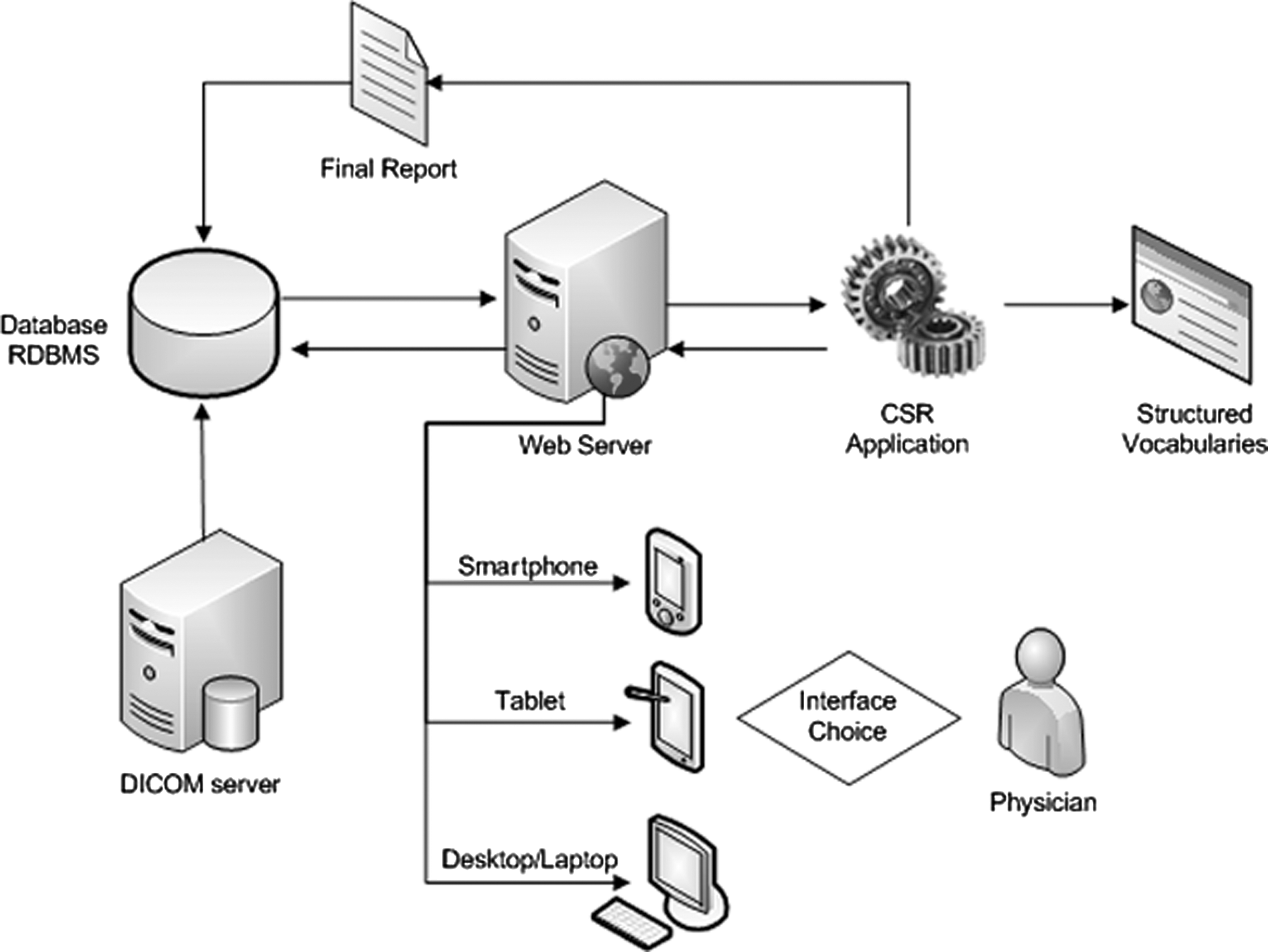
Cyclops structured reporting (CSR) report writing process.
The user interface provided by the CSR provides workflow guidance throughout the report writing process. It runs as a library on the Web server accessing the DICOM server and the structured vocabularies databases, transmitting the same clinical data to different interfaces in different devices. This means that physicians can write and retrieve SRs using smartphones, tablets, or Web browsers in a personal computer.
The Web and Mobile Interface
We developed a simple, usable and user-friendly interface in order to reduce the change on system impact to physicians. In order to improve the acceptability, physicians are able to use CSR without needing to know how to compose a DICOM SR, as shown in Figure 5.
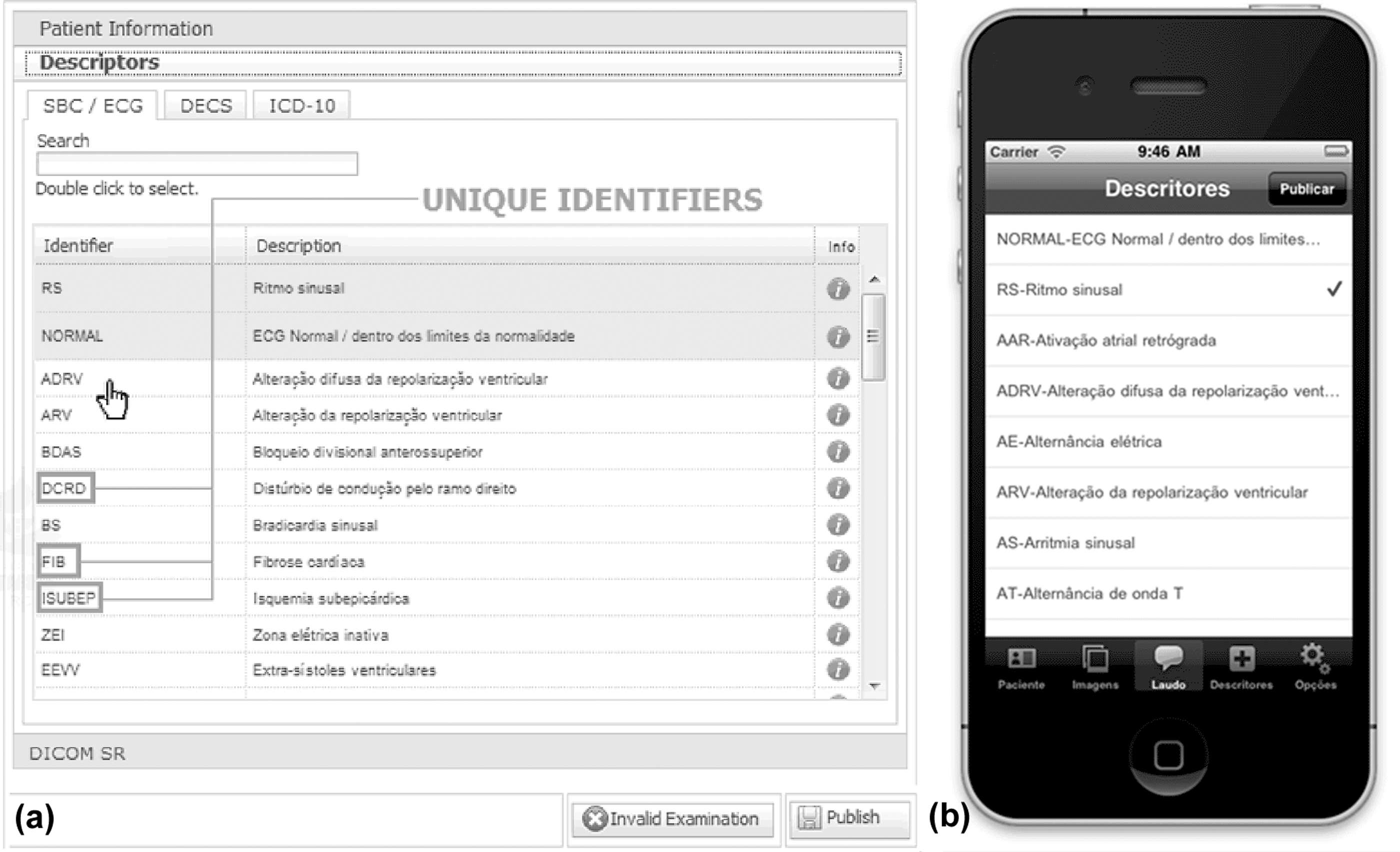
Fast-writing, vocabulary-based interface for electrocardiogram reports. It was developed in two versions:
Figure 5a displays the interface for the issuance of ECG reports. The cardiologist starts the report by choosing the controlled vocabulary that will be used. The use of BSC/CSR vocabulary is mandatory, and use of DeCS is optional. Additionally, the medical professional can add ICD-10 descriptors. After selecting the vocabulary, the user gets to select the descriptors that will be part of the findings description. The algorithm automatically creates an XML model and the DICOM SR object while the report is issued.
In order to facilitate the use by the medical community, we designed and developed a version for mobile devices. The application developed for these devices has all the features of the original interface: the user still selecting the structured from the vocabulary descriptors chosen and issuing the final report, which is presented on the screen device as shown in Figure 5b.
In the particular scenario of ECG a technician fills in a structured form with the entire patient's information provided by the physician who is requesting the electrocardiogram. Based on this structured information, it is possible to obtain specific numbers of co-morbidities, medicines in use, risk factors, and family history, after the examination is performed and the findings reports has been issued.
With the reports properly indexed, it is possible to examine possible associations between a list of co-morbidities and cardiac risk factors with a diagnosis.
In order to extract data that could be used as an example of the possibilities the system offers, we consulted a group of cardiologists from the STT/SC and asked them to establish groupings for the BSC/CSR vocabulary descriptors because the BSC classification is not organized as a tree but has only one level. This classification was intended to facilitate the high-level analysis and presentation of results directly related to the morbidities described through the BSC/CSR vocabulary. The BSC/CSR vocabulary descriptors were classified into 10 categories. The classifications are shown in Table 1 in relation to the population group of patients stored in the STT/SC. In this study 220,000 ECG examinations stored in our central database from August 2010 until May 2012 were analyzed.
Frequency Values in Brazilian Society of Cardiology/Cyclops Structure Reporting Descriptors
ECG, electrocardiography.
Our methodology allows, for example, inferences over prevalence and odds ratio data from different sources such as co-morbidities, medicines in use, and risk factors. We can also relate it with the final report written by the physician. The methodology behind the CSR application offers a proven and reliable structured for standardization, storage, and retrieval of clinical information. CSR also enables interoperability between different medical systems by offering an efficient mechanism for the distribution and management of medical documents, without the flaws of a system based on plain-text documents.
Discussion
This article presented an approach that uses the DICOM SR standard to accomplish diagnosis over telemedicine networks using structured vocabularies as the report foundation. A multidevice application for both Web-based and smartphone-based platforms was presented, as a viable solution for applying the DICOM SR standard in telemedicine networks with minimum impact over the physicians' routine and also providing a report writing process for electrocardiograms without syntax or conceptual mistakes and a structured input form for other modalities.
In order to evaluate our approach, we presented an example search for statistical data, demonstrating that traceability of morbidity can be achieved, resulting in a reliable, efficient, and data mining–friendly approach. By using structured vocabularies as the building blocks for the reports, together with stored information allows that patient clinical information can be readily crossed with these morbidity data, we were able to achieve data that potentially give us traceability over morbidity rates.
Our applications algorithm is responsible for coordinating the process of issuance of reports through various technologies and devices. The CSR works as a library in an HTTP server, which accesses information from studies in DICOM format from the database and from structured vocabularies. The application allows the transmission of the same clinical information to different interfaces and devices, allowing professionals to write and retrieve information from SRs, using smartphones, tablets, or Internet browsers on personal computers.
Our approach has been used in the context of the clinical routine in a large-scale asynchronous telemedicine network since August 2010, generating more than 220,000 reports using exclusively the DICOM SR standard with an average of 470 reports written daily. Different healthcare professionals such as physicians, technicians, and administrators use this model.
In future work we intend to apply the same methodology to the teleradiology service of the STT/SC, integrating the Radiological Society of North America's RadLex vocabulary into our application. RadLex is a lexicon for the uniform indexing and retrieval of radiology information resources, providing a specific radiology-structured vocabulary for computed tomography and computed radiography modalities. 21
Footnotes
Disclosure Statement
No competing financial interests exist.