
Abstract
Introduction
Several sources of information indicate a marked disparity between the need and supply of available child and adolescent psychiatric services. The Center for Mental Health Services 1 in 1998 estimated that 9–13% of 9–17 year olds had serious emotional disturbances and that 5–9% had extreme functional impairments. A 1999 report from the U.S. Surgeon General, 2 however, indicated that only 20% of emotionally disturbed children and adolescents received any mental health treatment. This severe shortage of available child mental health services is further compounded by an inequitable distribution of service providers 3 ; therefore children who live in poverty or rural areas are less likely to have access to child and adolescent mental health services. The field calls for strategies to explore new models of service delivery to efficiently utilize the professional resources currently available.
Attention deficit hyperactivity disorder (ADHD) is the most common childhood psychiatric disorder. 4 It is associated with an increased risk for antisocial behavior, substance abuse, early school termination, underemployment, and continuing social problems. A survey of pediatric primary care providers in the Pediatric Research in Office Settings network indicates that the ongoing management of patients with ADHD is ranked fourth in importance in their list of inadequately addressed questions in pediatric primary care research. 5
The hallmark symptoms of ADHD, including inattention, hyperactivity, and impulsivity, often lead to impairment in the parent–child relationship and contribute to increased stress among parents of children with ADHD. 6 Over time, parents may develop maladaptive and counterproductive parenting strategies to deal with these problems. 7 Effectively modifying poor parenting practices is of great importance, as poor parenting is one of the more robust predictors of negative long-term outcomes in children with behavior problems. 8 The efficacy of parent training in treating ADHD has been evaluated in many published studies. 9 –12 These studies suggest that parent training results in improvements in several important areas for children with ADHD, including parent-rated oppositional/aggressive symptoms, internalizing symptoms, teacher-rated social skills, parent–child relationships, and reading achievement. 10
Telepsychiatry has been proven to be an effective model in adult populations for collecting history, establishing diagnosis, and managing pharmacological and psychotherapeutic treatments, as well as providing consultation for primary care physicians working in remote and rural areas. 13 Studies also suggest high provider and patient satisfaction and economic efficiency of telepsychiatry. 14 The benefits of videoconferencing are well documented; however, there are very few randomized controlled trials to carefully compare the effectiveness of videoconference to traditional face-to-face conferencing. 15 To our knowledge, there are no existing data on the effectiveness of videoconferencing on parent training for children with ADHD. Results from an efficacy study on Web-based parenting skill program for young children with traumatic brain injury, however, were encouraging. 16
We hypothesize that parent training through videoconferencing will be as effective as face-to-face training in improving parent–child relations and the child's social skills and reducing ADHD symptoms. It will also be accepted to the same degree as the face-to-face presentation.
Subjects and Methods
Participants
Parents of children with ADHD between 6 and 14 years (mean, 10.37 years) of age were recruited from the University of California Davis School of Medicine Psychiatric Outpatient clinic and MIND Institute (Sacramento, CA). To be eligible for the study, children had to meet DSM IV-TR criteria for a primary diagnosis of ADHD. Participants with significant medical conditions that were not stable on their current outpatient treatment regimen or with severe psychiatric disorders (i.e., bipolar disorder, autism, schizophrenia, major depression) were excluded from participating. Concomitant medication treatment and psychosocial interventions including individual psychotherapy and school educational intervention were allowed, but parents were asked not to change the medication or treatment regimen during the videoconference training unless the child was admitted to the hospital or emergency room in order to hold treatment effects constant. The study was approved by the University of California Davis Institutional Review Board. All participants provided assent and parents provided consent at the beginning of the first evaluation. Families were paid $50 after finishing a 10-week session.
Baseline Assessment
All participants were screened and assessed for psychiatric disorders using a structured interview (Diagnostic Interview for Children and Adolescents [DICA], parent and child versions). 17 Parent and teacher versions of the Vanderbilt ADHD diagnostic rating scale, Parent Child Relationship Questionnaire for Child and Adolescents (PRQ-CA), Social Skills Rating System (SSRS), Children Global Assessment Scale (CGAS), Clinical Global Impression—Severity (CGI-S) score, and Clinical Global Impression—Improvement (CGI-I) score were collected as part of the initial assessment. Mothers were asked to complete the Beck Depression Inventory to assess maternal depression. Medical history, demographic data, and information about past and current treatments for ADHD and other psychopathology were collected through face-to-face interview following a standardized format developed by the ADHD program of the University of California Davis MIND Institute. The DICA interview was administered via a computer. In addition, a face-to-face clinical interview was conducted by a child and adolescent psychiatrist at the beginning of the study to confirm the diagnosis. After review of all available information, diagnoses were confirmed independently by two clinicians including the child psychiatrist who conducted the clinical interview. Disagreements were discussed by the involved clinicians and resolved by consensus.
Randomization
Caregivers were given options of which day of the week (Tuesday or Thursday) they would prefer, and a staff member, blinded to the caregiver's choice, was then randomly assigned either Tuesday or Thursday as the videoconference group and another time as face-to-face group meeting day.
Videoconferencing
Real-time videoconferencing was conducted with the therapist in a conference room and parents in a separate conference room. The two rooms are connected by a secured and established Tandberg 6000 videoconferencing system provided by University of California Davis Center for Health and Technology.
Interventions
Ten sessions of weekly parent training through either videoconference or face-to-face delivery were conducted using a manualized treatment based on that of Barkley. 4 Topics in the manual address basic behavioral management skills such as building positive relationship, paying attention to the child's play, issuing effective commands, attending, establishing a home token system, using time out, daily school behavior report card, and anticipating future behaviors. Each session is followed by a homework assignment for caregivers to practice the learned skills at home. The therapist had extensive training in behavioral approaches and parenting methods. A sole therapist delivered the treatment to both groups. The therapist met with another peer weekly to review the session and also ensure the treatment fidelity. A non-mandatory skill training and homework group was offered to the children of both groups while parents attended the parent training group in order to provide child care for the parents during the training sessions.
Outcome Assessments
Parent and teacher versions of the Vanderbilt ADHD diagnostic rating scales and SSRS, parent-rated PRQ-CA, clinician-rated CGAS, CGI-S, and CGI-I were collected at baseline and the end of treatment. The parent-rated Likert scales were collected at the end of the study.
Primary Outcome Measures
The PRQ-CA, developed by Kamphaus and Reynolds, 18 is a 71-item, parent-rated scale to evaluate a parent's perspective of the parent–child relationship (or the perspective of a person serving a similar role). It assesses seven dimensions of the parent–child relationship, including attachment, involvement, communication, discipline practices, parenting confidence, satisfaction with school, and relational frustration. The parents were asked to rate each item on a 4-point scale. The results were interpreted based on the instructions of the PRQ-CA manual. 18 The t scores, 90% confidence interval, and percentile rank were calculated against the normative data provided by the Parenting Relationship Questionnaire manual. The F-index, designed to detect excessively negative responses, and the D-index, designed to capture excessively positive responses, were also calculated based on the instruction of the manual. The t scores derived from the PRQ-CA were used in the data analysis. Extreme F-index or D-index ratings were not found in this sample.
Secondary Outcome Measures
The Vanderbilt ADHD diagnostic parent and teacher rating scales consist of 47 items to assess the core symptoms of ADHD (Inattentive and Hyperactive subscales) based on DSM-IV diagnostic criteria, other disruptive behaviors (Oppositional Defiant and Conduct subscale), screening questions for mood and anxiety symptoms (Mood and Anxiety subscale), and two performance subscales (Overall Academic Performance and Overall Classroom Behavioral subscales). The raters (parents and teachers) were asked to rate each item on a 4-point scale. The sums of points from each subscale were used for the purpose of statistical analysis. The Vanderbilt Rating Scale has been widely used to confirm the diagnosis of ADHD. 19
The CGI-S scale is a 7-point scale (1–7) to rate the severity of the participant's illness at the time of assessment; the CGI-I scale reflects the clinician's assessment of overall change from baseline to end point rated on a scale from very much improved (score of 1) through no change (score of 4) to very much worse (score of 7). To rate the CGI-S and CGI-I, the clinician reviews all collected rating scales and meets with parents at the beginning and the end of the study to review the parent's impression of the child's symptoms.
The CGAS is a numerical scale (1–100) used to rate the general functioning of children. The CGAS for each child was rated at the beginning and the end of study by a child psychiatry fellow based on the initial description of Shaffer et al. 20
We designed the Likert scale to measure the degree of acceptance of the training program and communication modality by parents. It consists of eight questions about the usefulness of the training program and four questions about the quality of and caregiver's preference of communication modality. The caregivers were asked to rate each item on a 4-point scale. The summary of points from the Usefulness of the Training Program and the Preference of Communication subscales were used for data analysis.
The SSRS is used to provide a detailed picture of a child's social behavior from the viewpoint of the respondent. 21 The SSRS teacher's version consists of 57 (for elementary school students in grades 3–6) or 51 (for secondary school students in grades 7–12) items, and the parents' version consists of 55 (elementary) or 52 (secondary) items. Those items cover the two domains of social functioning (Social Skills and Problem Behaviors), and the teacher's version has an additional domain on academic competence. The Social Skills scale has five subscales, including Cooperation, Assertion, Responsibility, Empathy, and Self-control; the Problem Behaviors scale covers three subscales, including Externalizing, Internalizing, and Hyperactivity Behavioral subscales. The Academic Competence scale does not have subscales. The raters were asked to rate each item on a 3-point scale. The standard score and percentile rank for all rating scale measures were calculated against the normative data provided by the manual. The standard scores for each scale and a summary of raw scores for each subscale were used for statistical analysis.
Statistical Analysis
Twenty-two subjects were enrolled in the study, with 13 in the face-to-face session and 9 subjects in the videoconference session. Results from all enrolled subjects were used for analysis (Fig. 1). The data from teachers were not included in the analysis because the majority of teachers did not return the rating scales when the subjects finished the study.
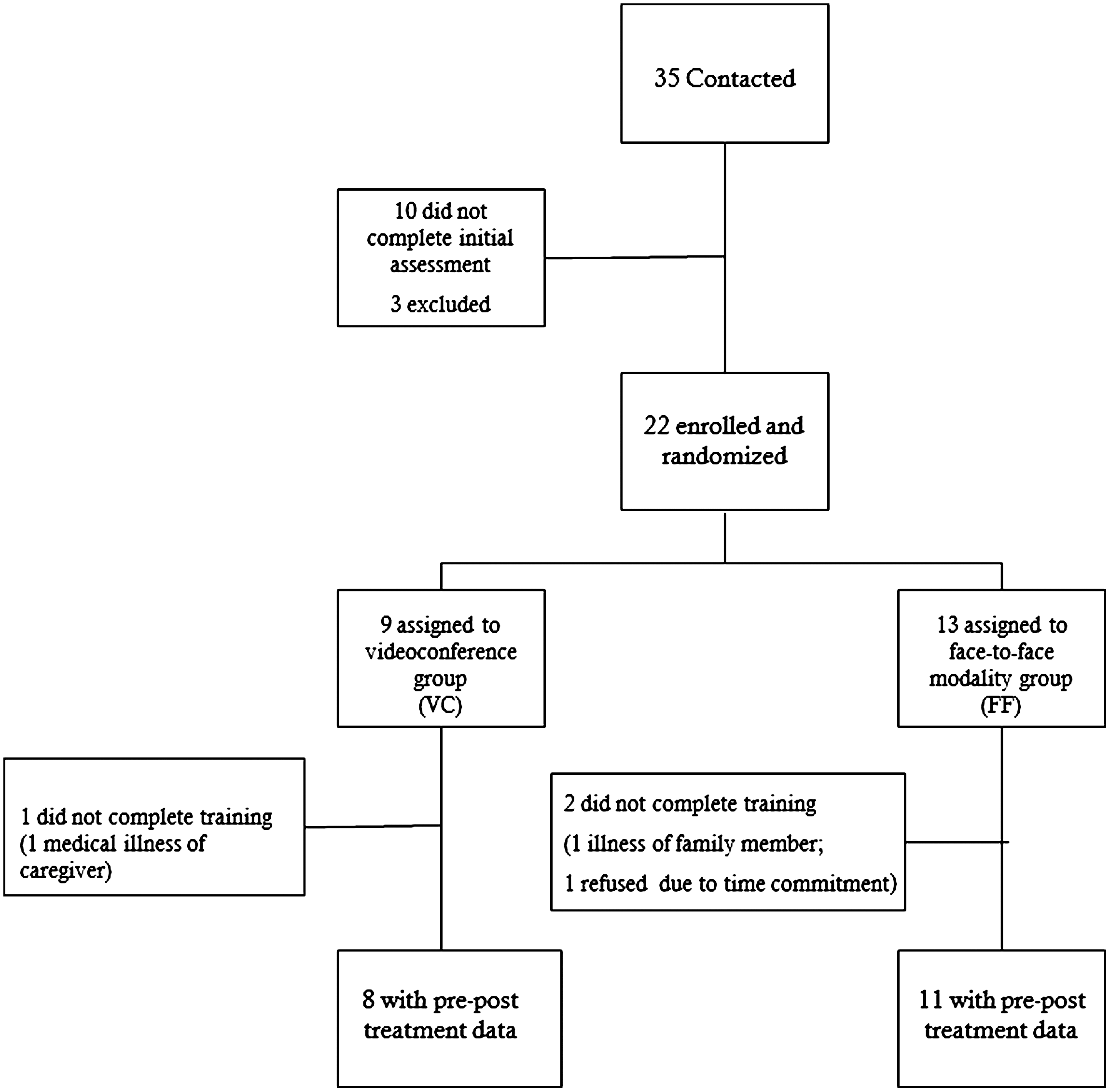
Flowchart of subject recruitment and retention.
To explore if there was a group effect (difference in treatment effects between two training modalities), time effect (difference between post- and pre-training), and the interaction effect of group-by-time, a mixed model was fitted for each of the outcomes by using PROC Mixed in SAS version 9.2 (SAS Institute, Cary, NC). The term of group-by-time was not significant in all outcomes; thus, we focused on the main effects of group and time. A Mann–Whitney U test assessed group differences from the Likert scale, whereas repeated t tests were used to test for group differences in treatment effects. The paired t test for numerical data (sums of rating scale and CGAS) and the Wilcoxon test for ordinal data (CGI-S and CGI-I) were used to test for time effects (comparing the pre- and post-intervention outcomes). A Pearson's correlation was used to explore the relationship of parent's years of education and attachment scores of PRQ-CA with all primary and secondary outcomes. Missing data were assumed to be missing complete at random. The statistical significance was defined at alpha of 0.05.
Results
Participant Flow
Participants were recruited by soliciting referrals from the Psychiatric Outpatient Clinic, MIND Institute, and the Pediatric Outpatient Clinic at the University of California Davis, as well as from practitioners in the greater Sacramento and surrounding areas. Thirty-five participants were contacted and consented to participate, and 25 of them finished the baseline evaluation; however, 3 were excluded because the participant's primary diagnosis was not ADHD, but learning disorder. The remaining 22 participants met the inclusion criteria and were randomized to the conditions. Three participants withdrew participations from the study (one caregiver became critically ill after finishing 4 weeks of training, one caregiver's family member became critically ill, and one caregiver decided to choose another intervention; the latter two finished 3 weeks of training), and their data were included in the analysis. Details of subject flow through the trial are presented in Figure 1.
Participant Characteristics
Demographic and clinical characteristics by treatment conditions are reported in Table 1. The t tests for independent samples indicate no significant differences between the groups on major demographic variables and measures, including children's age, mother's depression, and parent's years of education. Although the face-to-face group appeared to have high prevalence of comorbidity, Fisher's exact test indicated no significant differences between groups on diagnosis type, medication treatment, and comorbidity prior to the intervention except that the control group has a higher ratio of boys to girls. The medication dosage was adjusted for 1 subject in the face-to-face group during the course of the study.
Selected Sociodemographic Characteristics of Participants by Study Group at Baseline
Data are number of subjects (%).
BDI, Beck Depression Inventory; h/o dx, history of diagnosis.
Primary Outcome: Parenting Relationship Questionnaire Scores
As shown in Table 2, the t score of discipline practices significantly increased after training (p=0.006) with an effect size of 0.93. The difference between the videoconference and face-to-face groups was not significant (p=0.25). No significant group or treatment effects were observed for other subscales of PRQ-CA.
Pre- and Post-treatment Scores of Parent Training Through Videoconference and Face-to-Face Conference and Treatment Effects
The paired t test was used for statistical calculations.
Higher score indicates improvement.
Higher score indicates increased symptoms.
Indicates p value of Mann–Whitney U test.
CGAS, Children Global Assessment Scale; CGI-I, Clinical Global Impression—Improvement; CGI-S, Clinical Global Impression—Severity; ES, effect size (calculated as the difference between the change scores in post- and pretreatment divided by SD for the change score of pre- and post-treatment); FC, face-to-face conference; PRQ, Parent Child Relationship Questionnaire; SD, standard deviation; SSRS, Social Skills Rating System; VC, videoconference.
Secondary Outcomes
Parent perceptions of the videoconference and the training program
A Wilcoxon rank sum test was used to test whether there was a difference between the two groups on the Likert scale rating of the two subscales: the Usefulness of the Training Program and the Preference of Communication. The results (Table 2) showed no group difference in either of the ratings with the p values for the Usefulness of Program as 0.675 and the Preference of Communication as 0.264. The parents' rating on the Likert scale also indicated that they found the training program to be very useful (average score of 29 out of a maximal score of 32).
Vanderbilt Rating Scales
The results (Table 2) demonstrate significant improvements in all symptom clusters including Inattentive (p<0.001, effect size=1.11), Hyperactive (p=0.002, effect size=0.54), Oppositional Defiant (p<0.001, effect size=1.09), Conduct (p=0.001, effect size=1.12), and Anxiety (p=0.012, effect size=0.56) subscales. There was no significant improvement on the parent-rated Problem in Academic Performance and Behavioral Problems scales (p=0.19 and 0.68, respectively). Compared with the face-to-face conference modality, the videoconference group showed the same degree of improvement on all subscales of the Vanderbilt Rating Scale except better improvement on the Hyperactive subscale score with p=0.016 for group difference.
SSRS
Our results (Table 2) showed an improvement in parent-rated Social Skills (p=0.13, effect size=0.57), but the change on the Problem Behavior subscale of SSRS was not statistically significant. There is no significant group effect on the SSRS rating.
CGAS, CGI-S, and CGI-I
Our results demonstrate that parent training improves CGAS (p=0.011) and CGI-I (p<0.001) but that the change on CGI-S is not statistically significant (p=0.085). Again, there is no group effect on the three global functional scales (p=0.30, 0.47, and 0.44 for CGAS, CGI-S, and CGI-I, respectively).
Discussion
This study compared the effectiveness of parent training for ADHD children via videoconferencing versus traditional face-to-face groups. Telepsychiatry has been shown to be an effective modality for diagnostic work, consultation, and pharmacological treatment in adults. The use of videoconferencing specifically for the purpose of determining treatment effectiveness and modality acceptance in the area of parent training was unique.
This study demonstrates that parent training through videoconference was accepted to the same degree as face-to-face groups by parents as shown in the subscale of Preference for Communication measure. The study also shows that videoconference is as effective as the traditional face-to-face conference modality. Videoconferencing showed the same effectiveness as the face-to-face groups in helping parents develop better disciplinary practices as assessed by the PRQ-CA, in improving ratings on inattentive, hyperactive, oppositional, conduct, and anxiety symptoms on the Vanderbilt Rating Scale, and in improving the overall functioning of ADHD children by CGAS and CGI-I. Our results are consistent with findings from other telemedicine and telepsychiatry studies but add data on the usefulness and effectiveness of videoconferencing for parent training for ADHD. These data support the potential of delivering treatments for pediatric mental health populations that may result in reducing disparities in access to mental health services to families in remote areas.
The results demonstrate a large effect size (0.93) for increasing disciplinary practices in parents, whereas there were minimal changes in other areas of the parent–child relationship. These outcomes were assessed immediately after the training. It would be reasonable to expect improvement on other areas of the parent–child relationship in the long run if the increased disciplinary practices could be sustained to allow parents to gain confidence in their parenting skills and avoid negative or ineffective parenting skills.
The current study found parent-reported improvement for inattentive, hyperactive, oppositional, conduct, and anxiety symptoms for both treatment groups. The effect size ranged from 0.56 to 1.11, which is comparable with the findings of one recent meta-analysis 11 that indicated the overall unweighted effect size in pre-/post-intervention studies to be 0.7. However, a recent meta-analysis focused on a randomized controlled trial found that the effect of parent training on ADHD-specific behaviors are ambiguous. 22 The study of Fabiano et al. 11 was more inclusive and compiled 114 individual studies with different study designs, but the review of Zwi et al. 22 only included five studies with a randomized controlled design. Several factors may have contributed to the positive improvement in the child behavior in our study. First, the average years of education in our study population is slightly more than 14 years, which is higher than many previous studies. However, when we looked at whether parent's years of education were correlated with ratings of children's symptom severity, the only significant finding was a positive relationship between the mother's education and ratings on the Vanderbilt Anxiety subscale (p=0.022). This finding indicated that mothers with higher education might be more sensitive to their children's anxiety symptoms or that ADHD children with highly educated mothers are more anxious because they have higher expectations, particularly in regard to academic performance. Second, the attendance rate for our participants was very high. The majority of parents attended the 10-week consecutive training sessions and turned in their homework except for the three participants who did not complete the training. Third, the study was able to include a children's group, which was held at the same time as the parent group. Although this group was not purely therapeutic in nature, it did attempt to incorporate skill building in organization and time management while offering a structured play and homework time for children. In addition, the children's group probably increased the likelihood that parents attended all sessions.
We hypothesize that good attachment is an important foundation for behavioral management. Therefore, we explored the relationship of baseline ratings of the Attachment subscale in the PRQ-CA with the all outcomes. It is not surprising that we found that better attachment does correlate with larger improvement on the symptom clusters of oppositional defiant disorder on the Vanderbilt Assessment Scale (p=0.018). Previous studies have explored many parent and child factors on the effects of parent training; however, studies specifically focusing on the impact of attachment between parent and children are lacking. Our findings indicated that the parent–child relationship might be used as a predictor of treatment effect, not just as an outcome of parent training for ADHD children.
The current study has limitations. Although our results are robust, our sample size is small. This study was not specifically powered to detect differences between the two comparison groups. There were insufficient data in the literature on this topic to use to generate a power analysis that could be used to inform the sample size for the study. Because the group difference in our study was very small, a much larger sample size would be needed to detect a significant group difference. However, the study provided initial evidence that parent training through videoconferencing for children with ADHD yields results similar to other studies using face-to-face conference procedures.
We had a higher number of boys in the control group (face-to-face group), and the impact of this gender effect is unclear because there is no current literature addressing the interaction of gender and treatment effects in this area. Previous research does find a gender difference in symptom profiles in ADHD children, with boys exhibiting higher level of impulsivity and girls displaying more inattentive problem. 23 A study on parent training for early-onset conduct disorder indicated that girls' and boys' responses to treatment were markedly similar. 24
To ensure maximal participation, we allowed the parents to choose their preferred time for the training. The nature of treatment did not allow blinding. Therefore, the study is not a complete randomized double-blind study. Most of our outcome measures were based on parent-rated questionnaires, which might not completely be objective and could be influenced by factors other than the intervention, such as the parent's desire to please the therapist. The treatment effects were assessed immediately after the training; therefore the long-term benefit of the treatment is unknown at this point. Our sample also may be biased because of a high rate of well-educated, middle class, and intact families who are from Sacramento and Davis area. This population bias might contribute to our favorable treatment outcomes with several reasons. First, the parents might be able to understand and utilize the skills learned from the training more readily because of their familiarity with mental healthcare (most of the children were being treated by pediatricians or child psychiatrists for medication management) and high education. Second, highly educated, urban-dwelling parents are more likely to be familiar with new technologies and therefore feel more comfortable with videoconference communication systems. The outcomes for rural and undereducated parents are unknown given their unfamiliarity with the new technology and mental health but more urgent need for help. A larger study, recruiting more educationally and financially diverse group from areas lacking access to child mental health services, will be important to confirm the effectiveness and usefulness of videoconference in parent training.
Conclusions
This study provides preliminary evidence that parent training via videoconference can be as effective as traditional face-to-face conference for children with ADHD. Videoconferencing can be a useful model to address the access disparity for populations in remote areas who do not have access to mental healthcare.
Footnotes
Acknowledgments
We would like to thank the families for their participation, the volunteer residents and fellows from the general and child psychiatry training programs, Chloe Green, the Telehealth Program at the University of California Davis School of Medicine, and staff members at the ADHD program of the MIND Institute of University of California Davis for their time and great support, as well as sponsorship of the Elaine Schlosser Lewis Pilot Research Awards for Attention Disorder of American Academy of Child and Adolescent Psychiatry.
Disclosure Statement
None of the authors has competing financial interests or any commercial associations that would create a conflict of interest.