
Abstract
Introduction
Diabetes is a chronic illness, consisting of a group of metabolic disorders caused by insufficient production of the hormone insulin that affects multiple organs and tissues and manifests itself as increased blood glucose levels. 1 The World Health Organization acknowledges three types of diabetes with different origin and incidence: type 1, in which insulin production is not observed, is diagnosed about the age of 25 years, affecting near 4.9 million people around the world 2 ; type 2, in which insulin production is insufficient, is observed in adults and is obesity-related; and gestational diabetes, which appears in 1 out of 10 pregnant women and entails the dwindling of insulin production due to metabolism changes. Type 2 diabetes is a progressive disease 3 that is commonly undetected. 4 Before the clinical onset of diabetes, there is a long latent asymptomatic period that may last for decades. 5
Prevention of diabetes involves a paramount challenge. Research has shown that lifestyle and chemical treatments like acarbose 6 in people with impaired glucose tolerance can prevent or delay the appearance of diabetes. 7
This article presents a Web-based application that calculates the risk of suffering from type 2 diabetes (Diab_Alert). The use of the tool does not replace a diagnosis by a physician, 8 but it holds the promise of enhancing users' awareness of the disease. For example, people at high risk can ask for advice from their physician and get basal glucose tests done more often. This tool presents 15 questions that are based on research performed by experts, mainly the Diabetes Population Risk Tool (DPoRT) 9 and the Finnish Diabetes Risk Score (Findrisc). 10 According to the answers provided, the application shows a message with the global risk for each user and accompanies it with a graph that shows the probability of suffering from diabetes in the next 10 years.
Prior Related Work
During the research process, we have studied different methods for predicting the risk of diabetes. It is worth noting these: • The Findrisc questionnaire.
5,10
This is a questionnaire used in the Diab_Alert application to show the users a message with their global risk. It includes eight questions whose answers add points to the total risk score. The risk factors are age, body mass index (BMI), waist circumference, physical activity, intake of vegetables and fruits, hypertension, high blood glucose, and diabetic relatives. • The DPoRT.
9
It is an equation—not a scoring questionnaire or a software tool—that allows prediction of the probability of suffering from the disease in the next 10 years. Our tool Diab_Alert uses this tool to generate a graph that represents for the risk over the years, whereas other tools do not offer the users this kind of representation. Unfortunately, this algorithm may not be accurate for predictions over 10 years, so the application will be unable to display a lifetime risk as desired. • The Australian Type 2 Diabetes Risk Assessment Tool.
11
This method includes some specific questions, such as about Aboriginal, Maori, or Asian descent, which do not interest us, although the rest of the questions are very similar to those of the Findrisc. Thus Diab_Alert is not based on it because the former is designed for the Australian population and the latter is expected to be used mostly in Western Europe. • Enhanced diabetes prediction model.
12
This is a questionnaire on paper, not software. This prediction model asks about glucose level (in mg/dL), triglyceride level, high-density lipoprotein (HDL) cholesterol level, and uric acid, besides the typical factors like age, diabetic relatives, hypertension, and so on. Our application is intended to be user-friendly, namely, as simple as possible so that anyone can use it. Many users might not know their glucose, triglyceride, HDL, or uric acid level the first time they use the Web tool, so the results would not be precise. Moreover, if they know these values, it means they already have a reliable blood diagnosis. Besides, the picture of the risk over the years will not be based on these risk factors; therefore we do not include these variables in the application. • Risk test by the American Diabetes Association.
13
Several questionnaires like this can be found through the Internet. The questions are about age, sex, family, ethnicity, hypertension, physical activity, and weight. The risk factors are the same as those in the Findrisc, except for the waist circumference, and the result only displays the total score without specifying time. So, this method is not used.
Subjects and Methods
Risk Model
As explained above, Diab_Alert is based on two methods that were validated by their authors:
The DPoRT
The DPoRT allows prediction of the probability of suffering from the disease in the next 10 years applying the equation in Figure 1. The constants α and μ have the following values: α (for men)=0.8049, α (for women)=0.7814, μ (for men)=10.5971− 0.2624×(for hypertension − 0.150851) – 0.6316×(for nonwhite−0.1890142) – 0.5355×(for cardiopathy − 0.0485049) – 0.1765×(for smoker − 0.2683483)+0.2344×(education − 0.6944190) – 1.2378×[(age <45 years)×(BMI ≥23 kg/m2)×(BMI <25 kg/m2) – 0.1098877)] – 1.5490×[(age <45 years)×(BMI ≥25 kg/m2)×(BMI <30 kg/m2) – 0.1890539] – 2.5437×[(age <45 years)×(BMI ≥30 kg/m2)×(BMI <35 kg/m2) – 0.0586534] – 3.4717×[(age <45 years)×(BMI ≥35 kg/m2) – 0.0204186] – 1.9794×[(age ≥45 years)×(BMI <23 kg/m2) – 0.0757717] – 2.4426×[(age ≥45 years)×(BMI ≥23 kg/m2)×(BMI <25 kg/m2) – 0.1004247] – 2.8488×[(age ≥45 years)×(BMI ≥25 kg/m2)×(BMI <30 kg/m2) – 0.2102784] – 3.3179×(age ≥45 years)×(BMI ≥30 kg/m2)×(BMI <35 kg/m2) – 0.0670142] – 3.5857×[(age ≥45 years)×(BMI ≥35 kg/m2) – 0.0174318], μ (for women)=10.5474 – 0.2865×(for hypertension − 0.1639604) – 0.4309×(for nonwhite − 0.1885892) – 0.293×(for immigrant − 0.2364449)+0.2042×(for education − 0.6859416) – 0.5432×[(age <45 years)×(BMI ≥23 kg/m2)×(BMI <25 kg/m2) – 0.0718019] – 0.8453×[(age <45 years)×(BMI ≥25 kg/m2)×(BMI <30 kg/m2) – 0.0933620] – 1.4104×[(age <45 years)×(BMI ≥30 kg/m2)×(BMI <35 kg/m2) – 0.0366780] – 2.0483×[(age <45 years)×(BMI ≥35 kg/m2) – 0.0209614] – 1.1328×(0−0.0380835) – 0.0711×[(age ≥45 years)×(age <65 years)×(BMI <23 kg/m2) – 0.1105067] – 0.7011×[(age ≥45 years)×(age <65 years)×(BMI ≥23 kg/m2)×(BMI <25 kg/m2) – 0.0636299] – 1.4167×[(age ≥45 years)×(age <65 years)×(BMI ≥25 kg/m2)×(BMI <30 kg/m2) – 0.1083856] – 2.215×[(age ≥45 years)×(age <65 years)×(BMI ≥30 years)×(BMI <35 kg/m2) – 0.0387616] – 2.2695×[(age ≥45 years)×(age <65 years)×(BMI ≥35 kg/m2) – 0.0177015] – 1.726×(0−0.0164429) – 1.0823×[(age ≥65 years)×(BMI <23 kg/m2) –0.0493039] – 1.1419×[(age ≥65 years)×(BMI ≥23 kg/m2)×(BMI <25 kg/m2) – 0.0280374] – 1.5999×[(age ≥65 years)×(BMI ≥25 kg/m2)×(BMI <30 kg/m2) – 0.0538456] – 1.9254×[(age ≥65 years)×(BMI ≥30 kg/m2)×(BMI <35 kg/m2) – 0.0176045] – 2.1959×[(age ≥65 years)×(BMI ≥35 kg/m2) – 0.0049091] – 1.8284×(0−0.0139008).

Equation about the risk model.
In the formula, every risk factor concerning μ must be replaced by “1” if the condition is fulfilled or “0” otherwise. For example, if the user smokes, the variable smoker must be replaced with 1; if the user is 46 years old, the variable age <45 years counts as 0, and age ≥45 years is considered 1. Altogether, there are nine risk factors: age, sex, BMI, hypertension, heart disease, ethnic group, smoker, secondary education, and immigration.
Our innovation in Diab_Alert is that the equation in Figure 1 is used to generate a graph that stands for the risk over the years, whereas other tools do not offer the users this kind of representation. The DPoRT gives the result as a numerical probability, but it is not available at other Web sites because it was originally designed as a predictive algorithm, not as a (software) tool for the population. In fact, all you can find about the DPoRT in the Internet, in terms of usage with a computer, is a macro for Microsoft® (Redmond, WA) Word. This does not constitute a specific application for calculating the risk of diabetes, not to mention its incompatibility with mobile devices.
The Findrisc questionnaire
The Findrisc questionnaire is also used in the Diab_Alert application to show the users a message with their global risk. It includes eight questions whose answers add points to the total risk score. The Findrisc questionnaire is available in several Web sites because of the simplicity of the questionnaire, but does not do calculations over time. These Web sites simply show a low/high-risk result.
This and the previous method give similar results, although, according to their authors, the Findrisc may overestimate the risk, whereas the DPoRT tends to underestimate it. The risk factors that appear in the Findrisc are the following: • Age. If it is greater than 65 years, we add 4 points; if it is between 55 and 64 years, we add 3 points; and if it is between 45 and 54 years, we add 2 points. • BMI. If it is greater than 30 kg/m2, 3 points must be added. If it is between 25 and 30 kg/m2, 1 point is added. • Waist circumference. If it is between 94 and 102 cm for men or 80 and 88 cm for women, we add 3 points; if it is over 102 cm for men or 88 cm for women, we add 4 points. • Frequent exercise. If the user is sedentary, we add 2 points. • Intake of vegetables and fruits. If the user does not eat them daily 1 point is added. • Hypertension. We add 2 points if the user is on medication for high blood pressure. • High glucose. If the user has been found sometimes to have high glucose values, we add 5 points. • Diabetic relatives. If any of their parents, siblings, or children is or was diabetic, we add 5 points; if any of their grandparents, aunts, uncles, or cousins is or was diabetic, 3 points is added.
According to the total score, less than 7 points means the risk is low. If the score is between 7 and 11, it is slight. Either 12 or 13 points indicates a moderate risk, whereas a score over 14 denotes a high risk. When the result exceeds 20 points the risk is considered very high.
Architecture
As explained before, our aim was to make a widely compatible Web-based application. For that reason, we considered HTML plus PHP quite a suitable and efficient solution. Also, it is optional that the user browser supports JavaScript because it improves some visual behavior. As seen in Figure 2, the client Web browser launches requests to the server, which processes the proper PHP file and generates HTML code that is sent back to the client. This happens every time users interact with the Web page, especially when they send the answers to the questionnaire and receive the results. This way, no additional software needs to be installed, regardless of whether the subjects use a computer or a mobile device.

Architecture.
Web Page Design
The application is intended to be simple, widely compatible, and user-friendly (available at
Mobile version: Home page, Questionnaire, and Results.
The Web site is organized into these sections: Home, Questionnaire, Results, Statistics, and Administration. The Home page displays a short description of the Web application as well as of diabetes, its types, and common symptoms (Fig. 4).
Home page.
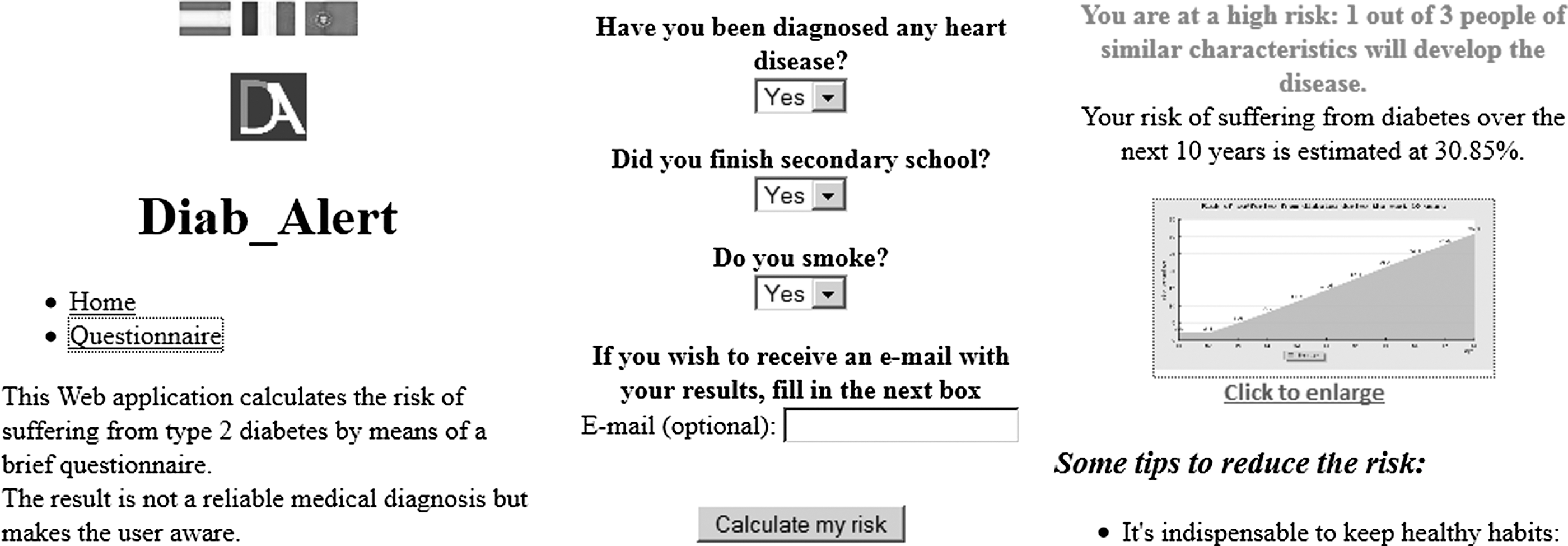
The questionnaire presents 15 questions that allow the calculation of the risk (Fig. 5). Besides, the user may fill an additional field in order to receive the results via e-mail. When the user completes the test and presses Calculate, all the answers are sent to the Results page.

Questionnaire.
In that moment, the PHP server evaluates the answers to the questionnaire and shows a message with the overall risk according to the total score—without specifying any time. Also, a graph appears (Fig. 6) that represents the probability of developing the disease in the next 10 years using the equation that appears in Figure 1. At the bottom of the Results page, some tips to reduce risk are shown; for example, if the BMI is over 25 kg/m2, 14 a message appears and suggests losing weight (Fig. 7).
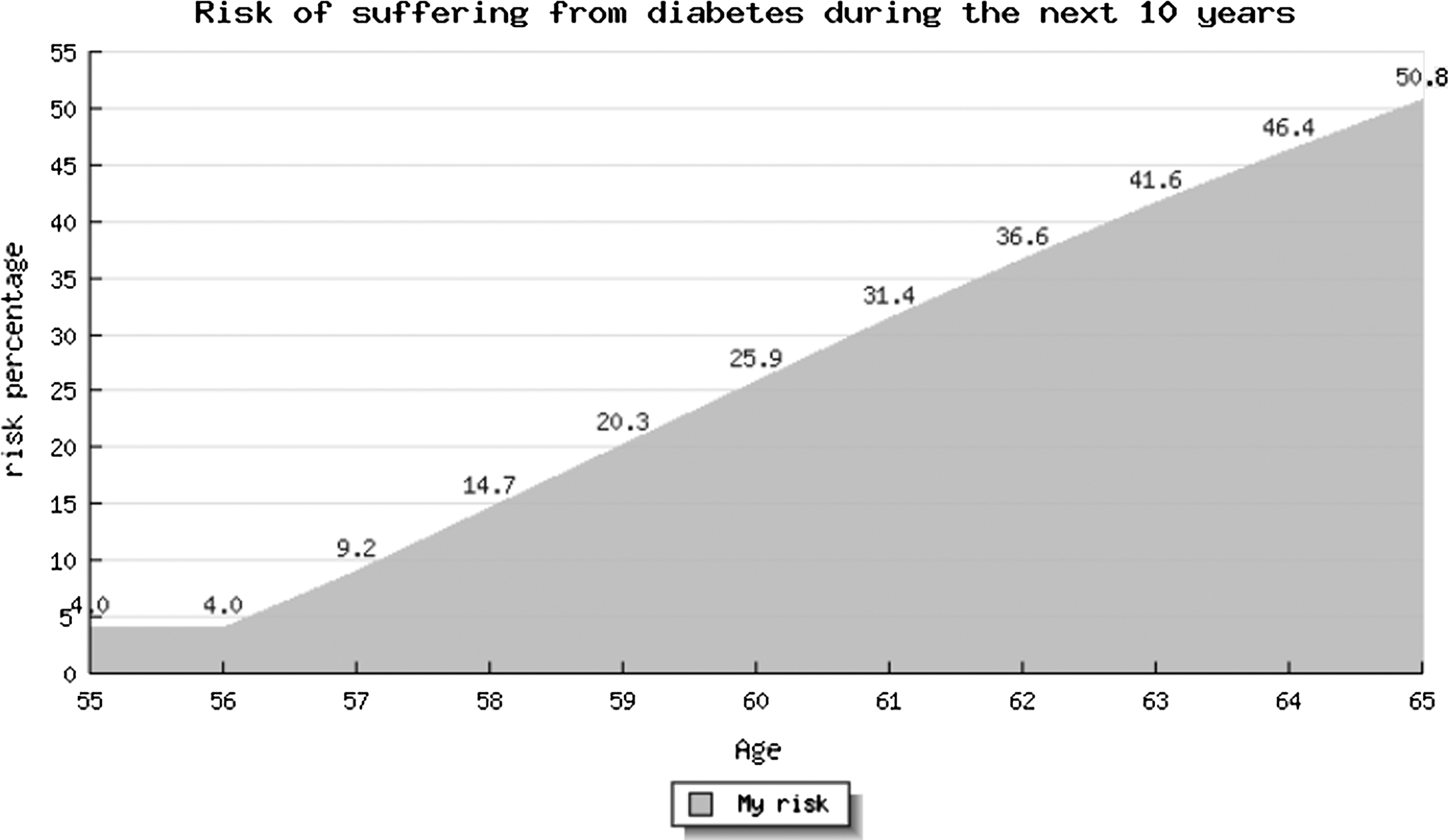
Results.
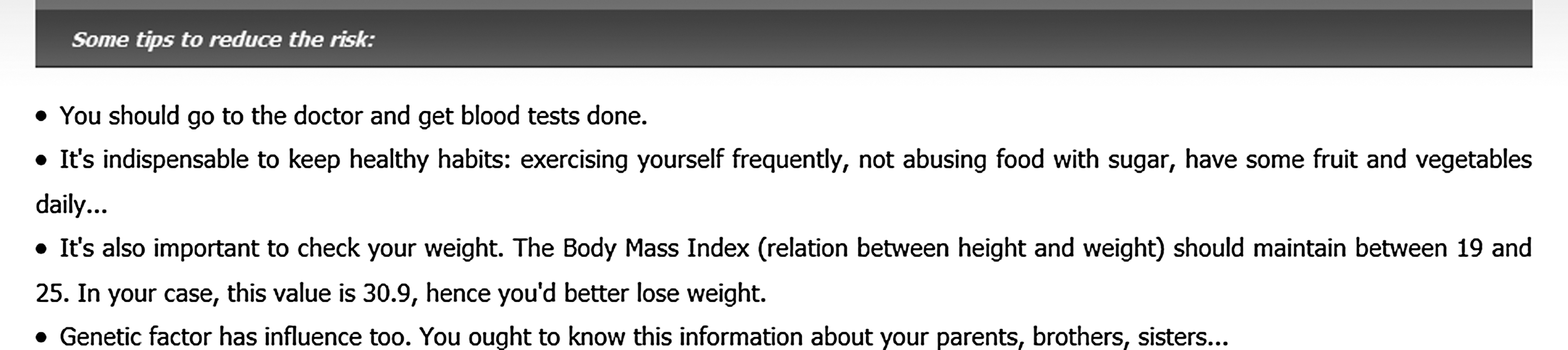
Some tips to reduce the risk.
Moreover, all the answers of the questionnaire as well as the results, the language, and the kind of device used are saved into a database for statistical analysis. This is where the Statistics and Administration parts become significant. These two sections require logging with a username and a password and are not accessible to common users. Through the Administration page, the administrator can view the entire database and delete particular data if necessary (Fig. 8).
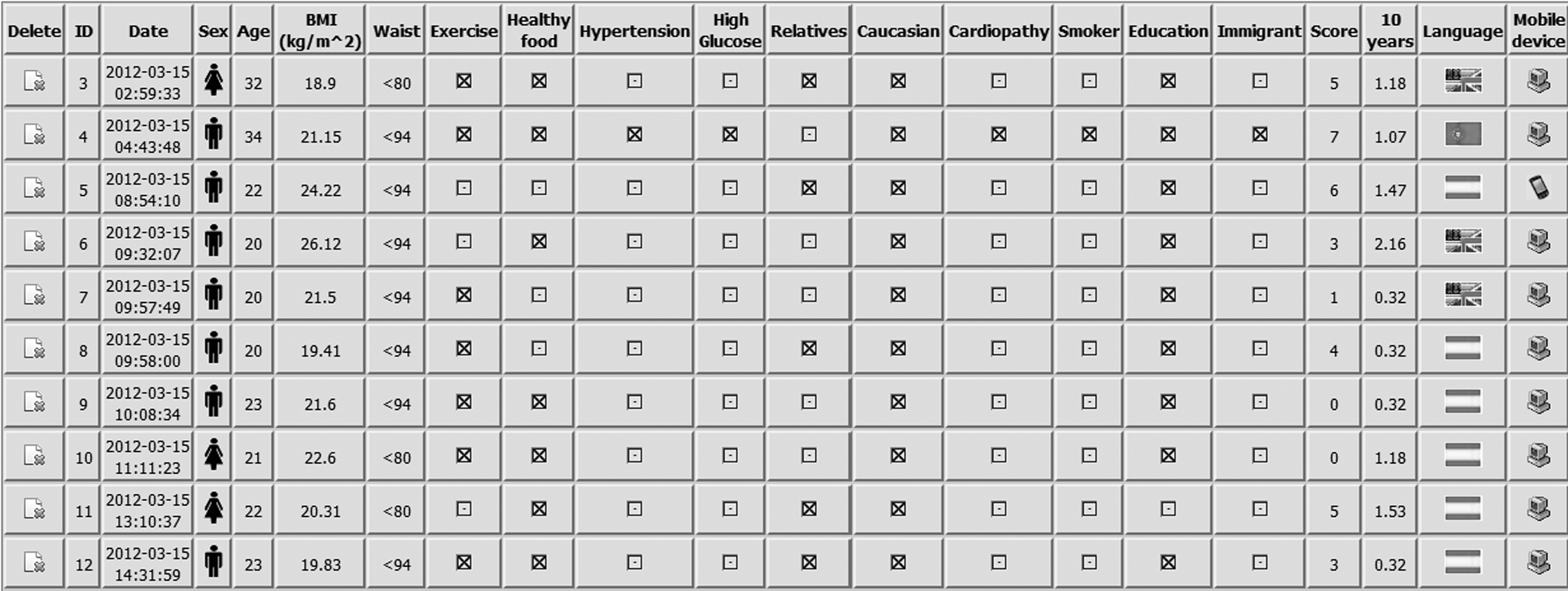
Some data stored for the administrator. BMI, body mass index.
In Statistics, the administrator can check how many users have done the questionnaire in terms of every risk factor, language, and sort of device used. In addition, there are many graphs available. The administrator is offered the choice to view specific information such as the total number of users or the risk in the next 10 years as a function of age, BMI, hypertension, etc. (Fig. 9).
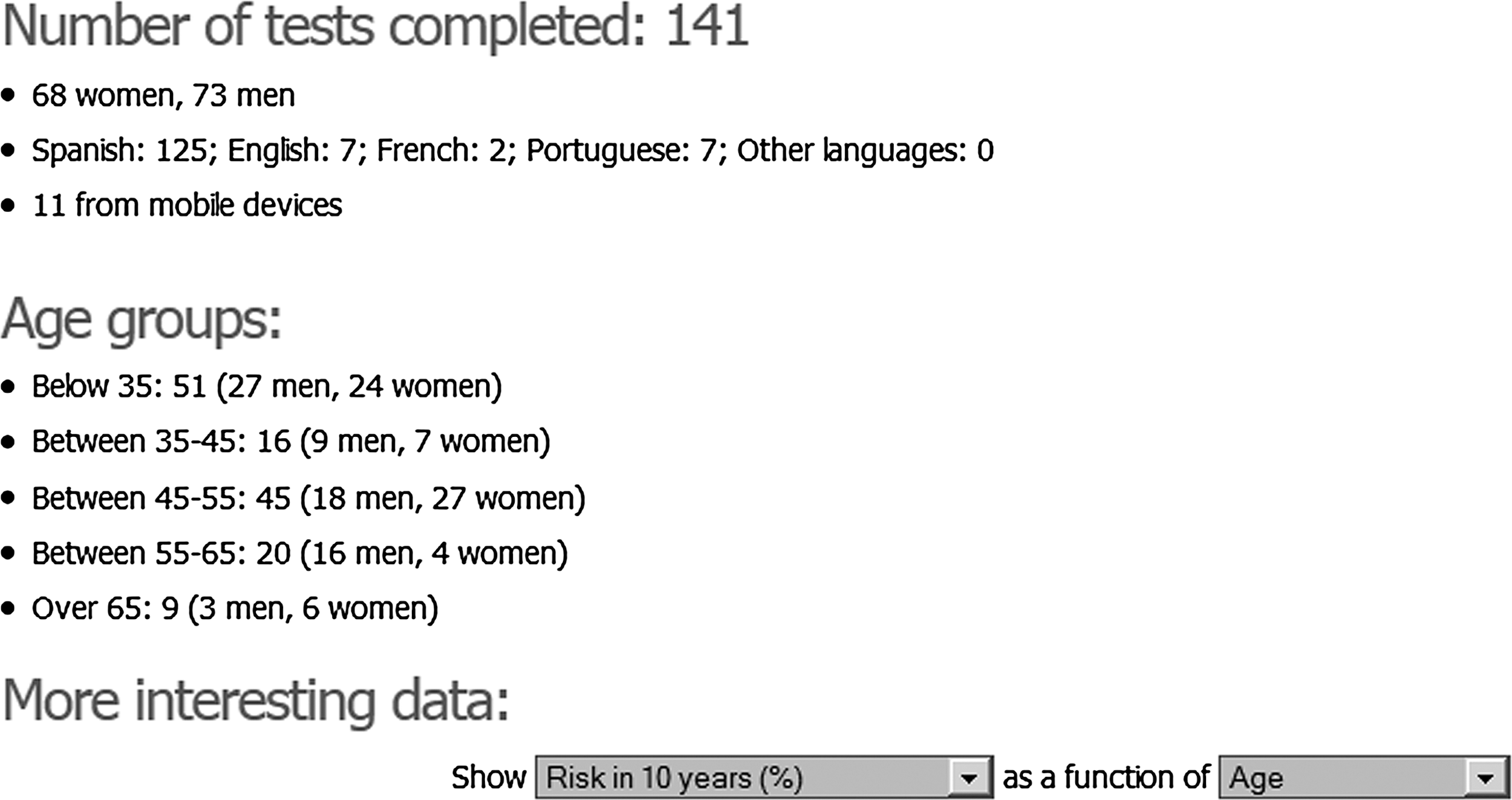
Statistics accessible by the administrator.
Results
Performance Evaluation
Response time has been measured in the browser Mozilla Firefox with the tool Firebug. Download time obviously depends on the broadband limit agreed to with providers. In this case, the measures have been made with a maximum (available) download rate of 6 megabits per second. According to repeated measurements, in both the standard and mobile versions, the Home and Questionnaire pages loaded completely in between 700 to 800 ms. Then, when the questionnaire is complete, the results are shown to the user in between 900 and 1,200 ms, which means the server takes between 200 to 500 ms to process the risk factors, create the graphic representation, and store the statistics in a database. It is worth pointing out that a random, intentional delay has been introduced in the calculation process to avoid massive attempts to send e-mail, so the result is quite satisfying.
Other Web tools
The Diabetes Risk Test from the American Diabetes Association 13 took between 2,000 and 4,000 ms to load fully. This greater variation may be caused by the fact that the test does not appear in a dedicated window, but rather is surrounded by pictures and advertisements. Moreover, the final result is not a graphic prediction over time, but a simple low/high-risk message, which asserts worse performance efficiency than Diab_Alert. This tool lacks a mobile version, so no mobile comparison is feasible. With regard to the Australian Type 2 Diabetes Risk Assessment Tool, 11 the test loads completely in 6–11 s. The result is calculated with JavaScript, without redirecting to a different page, so some browsers may not be fully compatible. It also lacks a mobile version, and the result is a low/high-risk message like the previous tool, so the performance of Diab_Alert results is satisfactory.
Finally, as explained in the Introduction, the performance of other techniques such as the enhanced diabetes prediction model 12 cannot be compared because it has not been implemented as a Web tool. It is instead a questionnaire that can be completed on paper.
User Evaluation
So far (April 26, 2012), the questionnaire has been completed by 141 people, of which 73 are men and 68 are women. Most of the users (n=125) have used the Spanish language, whereas 7 chose Portuguese, 7 chose English, and 2 chose French. Moreover, 11 of them used a mobile device. The number of individuals who have completed the test is too small to draw significant conclusions, but it is useful to begin discussing and analyzing statistics.
Another limitation is the lack of data related to the impact on users' behavior. This is due to several facts: the intention to build a very specific tool (with no sections for collecting opinions), the anonymity of the users when it comes to completing the questionnaire, and the fact that our planning did not include monitoring of individuals over the years because this is not a medical study. To do such an evaluation, we would have to follow the evolution of disease in every user for 10 years.
Some statistics of interest, such as risk as a function of age or BMI, can be viewed in Figures 10 and 11. The number of individuals who completed the questionnaire is too small to draw conclusions, although results are not as advanced as expected. It is remarkable that risk is higher in people older than 45 years old, especially in men. Also, BMI has a notable influence: people with a BMI greater than 30 kg/m2 are at a much higher risk than those with a proper BMI below 25 kg/m2. Other factors like hypertension, lifestyle, and family history have an influence too, although to a lesser extent. Unfortunately, some of them could not be included in the equation shown in Figure 1 because of the lack of population data by the developers of DPoRT. 9
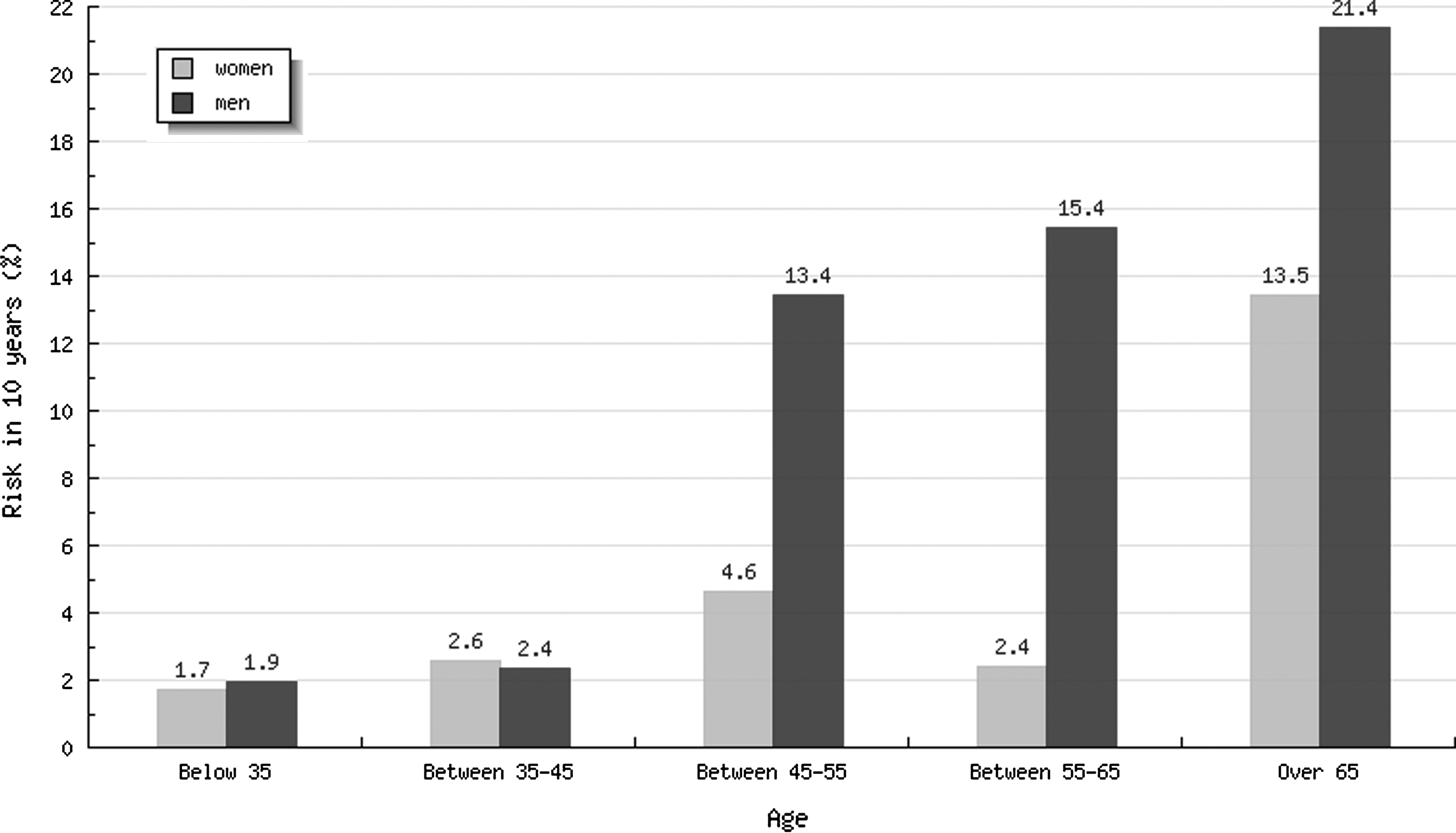
Risk and age.
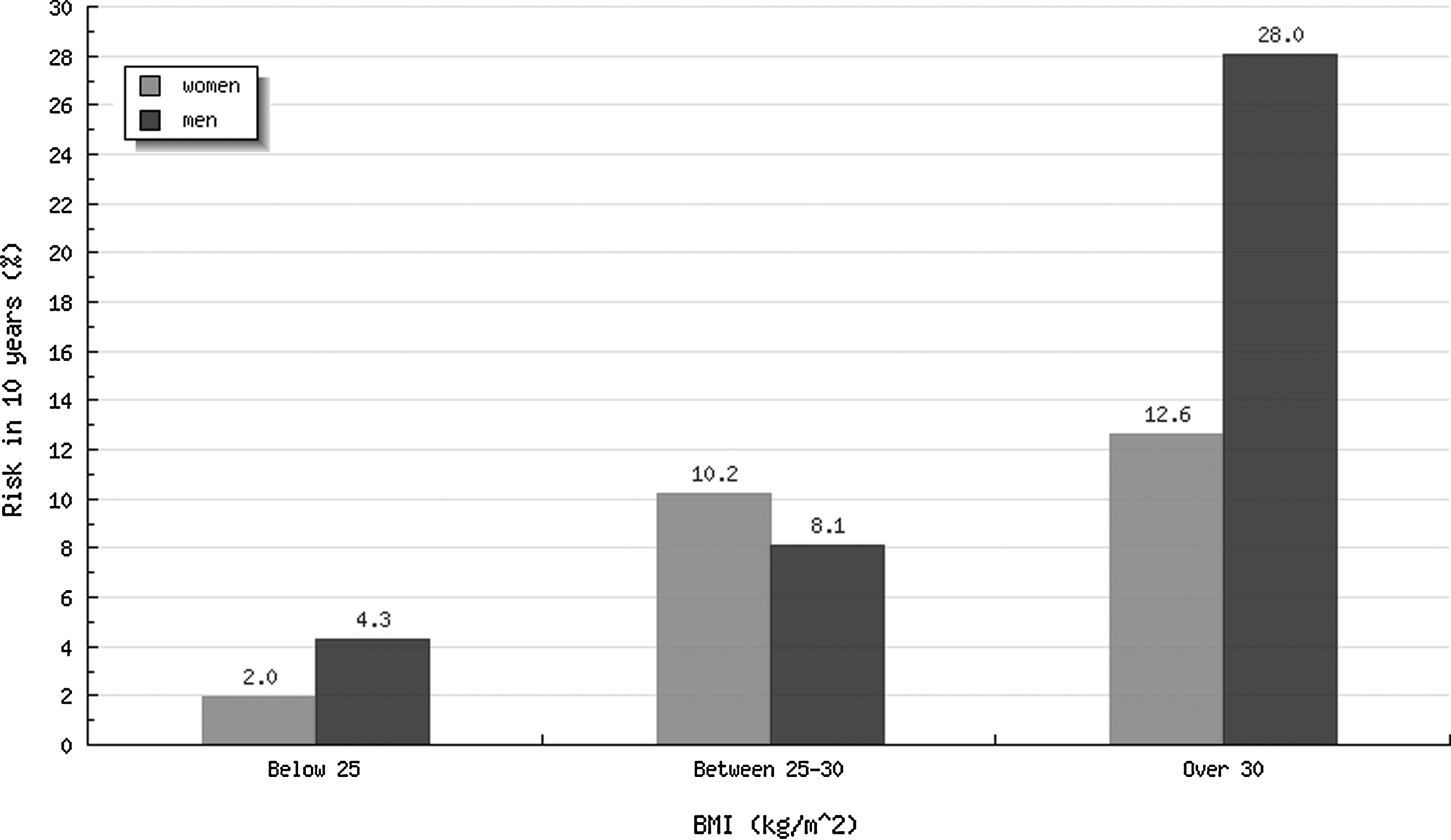
Risk and body mass index (BMI).
Discussion and Conclusions
The incidence of type 2 diabetes is growing in all populations worldwide. It is a major risk factor for death and numerous nonfatal complications that will form a hefty burden to the patients, their families, and the healthcare system. 14 Type 2 diabetes is also associated with increased risk of cardiovascular disease and premature mortality and is the leading cause of blindness, kidney failure, and nontraumatic amputations resulting from microvascular complications. 1
Numerous recent intervention studies have borne out that type 2 diabetes can be efficiently prevented by lifestyle variation in high-risk individuals. This is one of the most astonishing things about this disease. At present, the major task for public health administrations is to identify individuals who would take advantage of exhaustive lifestyle counseling. To lower the risk of diabetes, people must follow similar guidelines for warding off heart disease: eating a healthy diet, exercising daily, maintaining a healthy weight, and talking to the doctor about being screened for prediabetes. In fact, people with prediabetes can be helped to prevent the progression to type 2 diabetes by lifestyle changes and medication. There are risk factors that boost the risk but cannot be controlled: ethnicity, family history of diabetes, and age over 45 years. Nonetheless, there are other factors that can be controlled: being overweight, defined as a BMI over 25 kg/m2; sedentary lifestyle; abnormal cholesterol and blood fats, such as HDL cholesterol lower than 35 mg/dL or triglyceride level over 250 mg/dL; high blood pressure greater than 140/90 mm Hg in adults; and also smoking.
Even though the population is progressively more aware of the peril of diabetes and its complications, more education is needed in community and clinical settings. 14 Many people are living with diabetes or prediabetes but are unaware of their condition. This fact makes diabetes risk communication an important application area. 8
Web platforms are an efficient solution in the field of e-health, as neither their display nor their maintenance is very costly. Diab_Alert has been designed with the primary target of the creation of a widely compatible tool that predicts the risk of type 2 diabetes that raises the public awareness of this disease. It is available in four languages (English, Spanish, Portuguese, and French) and is ready to add new ones if necessary. Even though it includes both a standard version for computers and a simpler version for mobile devices, which makes it different from other tools, more adaptations may be developed in the future, so as to span the vast variety of mobile devices with different display resolutions.
Other outstanding feature of this Web application is the graph shown when the questionnaire has been completed successfully, as well as the option to send the results by e-mail, whereas other related tools do not present this sort of depiction—they only display the total score or a global risk, without specifying a numerical probability or a time interval.
Besides, this platform has been designed exclusively for predicting the risk of type 2 diabetes, whereas on other platforms this is not their main objective because they are usually health Web sites embracing numerous diseases. Diab_Alert dedicates the whole screen, whereas other tools open a small pop-up window in a corner, which may make it harder to display or understand the results for inexperienced users. In addition, there is no advertising on the page so viewers do not have unnecessary distractions.
Even though the application is complete and fully operative, several improvements can be carried out: • Translation. There are four languages available: English, Spanish, French, and Portuguese, but more languages should be included to provide greater accessibility. • Adaptation to mobile phones. Although Diab_Alert includes a simple style for mobile devices, more versions can be developed in order to adapt the design to the ample diversity of mobile devices with different display resolutions. • Delivery of multimedia messaging system. Users can receive the results by e-mail, but a system to send the results to a mobile phone using multimedia messaging system would be interesting too. • Social networking wervices. The results given by the tool Diab_Alert could be published in the users' profiles in trendy platforms like Twitter or Facebook. This would spread the application quickly and concern more people about the prevention and consequences of diabetes.
As for statistics, it has been mentioned that the sample is too small to draw significant conclusions. Nonetheless, 67 users who have completed the test are less than 45 years old and are at low risk, comparing both the DPoRT and Findrisc results. The rest of them (74 users) are older than 45 years, and their risk rises notably. As seen in Figures 10 and 11, risk increases with age and BMI, and it is slightly higher in men than in women. Although some factors such as family history or age are inevitable, others can be changed with enough willpower (weight, nutrition, physical activity, etc.). It is the users' duty to have blood tests done if they are at a very high risk.
Footnotes
Acknowledgments
This research has been partially supported by the Spanish Social Security Administration Body under project 85/2010, by the Instituto de Telecomunicações, Next Generation Networks and Applications Group, Portugal, and by national funding from the Fundação para a Ciência e a Tecnologia through the PEst-OE/EEI/LA0008/2011 project.
Disclosure Statement
No competing financial interests exist.