
Abstract
Concussion awareness and management in sports have gained a great deal of attention in light of research illustrating the potentially devastating consequences of repeated traumatic brain injuries. In order to address this public health crisis, numerous states have passed legislation that mandates medical clearance before being eligible to return to play of concussed athletes by a qualified healthcare provider. As the number of qualified healthcare providers with expertise in the diagnosis and management of concussions remains very small, patient safety and the ability to fulfill these legislative return-to-play requirements present unique problems to rural communities without easy access to subspecialty care. Telemedicine is a possible means by which to address the needs of the rural student-athlete.
Introduction
Concussion is a highly prevalent and under-recognized disorder that affects 1.7–3.8 million individuals in the United States every year. 1 These estimates are felt to be grossly underestimated, however, as many concussed individuals with mild or rapidly improved symptoms are never identified and may never seek medical attention. Concussion is a significant public health concern that transcends age and gender, can occur in any sport, and has potentially devastating consequences if unrecognized and untreated.
Although most concussions are short-lasting and self-limited, the effects of repetitive and untreated concussions may result in long-lasting, progressive sequelae, including profound cognitive, psychiatric, and neurologic symptoms which can be seen in chronic traumatic encephalopathy (CTE). CTE is associated with various neurometabolic and structural brain abnormalities supported by autopsy studies revealing the presence of pathologic changes in repetitively concussed brains, including the presence of tau immunoreactive neurofibrillary tangles, neuropil neuritis, and β-amyloid plaques. 2 Additionally, magnetic resonance spectroscopy studies have made associations between acute concussive head injuries and significant disruptions of the normal metabolic activity of the brain, including decreases in the N-acetylaspartate–creatine and N-acetylaspartate–choline ratios, that can persist for weeks beyond the full resolution of clinical symptoms. 3,4
As the potential sequelae of concussion become more widely recognized, a great deal of attention has been focused on concussion awareness and the need for preventative strategies to help minimize risk to the athlete. Specifically, professional sports organizations such as the National Football League and the National Hockey League have made new rules and also been more strictly enforcing existing rules in an effort to address preventable concussions and allow for the proper triage and treatment of concussed athletes. Many states have also addressed the problem through legislation aimed at protecting student-athletes at the amateur and collegiate levels.
Arizona Senate Bill 1521, signed into law by Governor Jan Brewer on April 18, 2011, mandates concussion education for all players, parents, and coaches engaged in interscholastic sports, removal from competition any player suspected of having a concussion, and formal clearance of concussed athletes for return to play by a healthcare provider trained in the management and evaluation of concussion.
Although this legislation represents a uniformly positive change in the culture of athletics and the awareness of concussion, it presents a unique problem for nearly one-third of the population of Arizona living in rural communities who frequently lack access to the specialized medical care available in larger metropolitan cities such as Phoenix or Tucson. 5 Telemedicine networks currently exist in Arizona and have been invaluable in providing rapid, accurate, and effective care for rural citizens suffering from acute stroke. To date, there are no reports of telemedicine technology being used to help in the evaluation and management of concussed athletes.
Case Report
We report the case of a 15-year-old boy who presented for telemedical consultation with a complaint of postconcussive symptoms 19 days after sustaining a head injury while playing soccer. Eyewitness accounts revealed that his head struck the shin of an opposing player who was in the process of kicking the ball, after which he experienced a brief loss of consciousness under 1 min in duration. Although he was able to exit the playing field without assistance, within minutes he experienced an abrupt alteration in mental status with no response to voice and a lack of spontaneous speech production. He was immediately transported by ambulance to the local emergency department of an 89-bed regional healthcare facility that serves nearly 90,000 local residents and seasonal visitors but lacks direct neurological support. Upon arrival and triage assessment, the emergency department physician on duty reported that the patient appeared to resist examination of his pupils by forcibly closing his eyes and only exhibited motor response to deep pain stimulation. His Glasgow Coma Score was reported as 8. The patient's mental status began to normalize within 30 min of arrival to the emergency department and had completely returned to baseline within 4 h. The patient has only a partial recollection of these events and was found to have approximately 30 min of both retrograde and anterograde amnesia. He was observed in the hospital for 24 h prior to discharge home, and a non-contrast head computed tomography scan obtained at the time of his emergency department admission was determined to be normal. The patient reported that after the event, his only persistent symptoms were bifrontal headache with photophobia, phonophobia, and worsening of pain with activity as well as intermittent difficulties with concentration. He did not complain of balance difficulties, nor did he complain of depressive symptoms or anxiety; however, his father observed that the patient seemed to be sleeping more than usual.
As the patient considered his initial symptoms to be significantly improved over the ensuing 2 weeks, he had begun to return to physical activity and training with his soccer team. Although light running and jogging did not precipitate symptoms, he did report that more aggressive running and jumping consistently resulted in an exacerbation of his headache.
Methods and Results
Via real-time audiovisual link through a Global Media, i8500 Mobile Telemedicine cart with EasyShareVC videoconferencing software, a direct connection was made to the community's regional healthcare center allowing for a subspecialty concussion evaluation (Fig. 1). History was obtained from both the patient and his father who was at the bedside. His medical history was significant only for two concussions (one 4 years prior and the most recent 19 days prior to telemedical evaluation). His only reported medication was acetaminophen taken as needed for headache. Social history was unremarkable with no history of tobacco, alcohol, or illicit drug use. On examination, the patient was well developed, pleasant, cooperative, and in no acute distress. General neurologic examination including cranial nerve examination, sensory examination, muscle stretch reflexes, coordination, and gait were normal. Headache Impact Test (HIT-6™ [Quality Metric, Inc.]) score was 46, Generalized Anxiety Disorder 7-item score was 4, and Patient Health Questionnaire (PHQ-9 scale) score was 11. The Sport Concussion Assessment Tool 2 was then used to assess the patient for other signs of cognitive and balance dysfunction. The patient's performance on tests of orientation and immediate memory were normal; however, he appeared to have mild to moderate difficulty with concentration. Additionally, although he endorsed no subjective balance difficulties, he exhibited moderately impaired balance on single-leg stance. His Sport Concussion Assessment Tool 2 total score was 82/100.

The remote examiner is pictured obtaining the history and preparing to examine the patient via real-time audiovisual link with the emergency department.
His previous non-contrast head computed tomography scan was readily available for review via a remote Picture Archiving and Communication System, as were the results of his after-injury computerized cognitive testing using the Axon Sports Computerized Concussion Assessment Tool (Fig. 2). Pertinent clinical notes from his previous emergency department visit were faxed to the remote examiner for review.
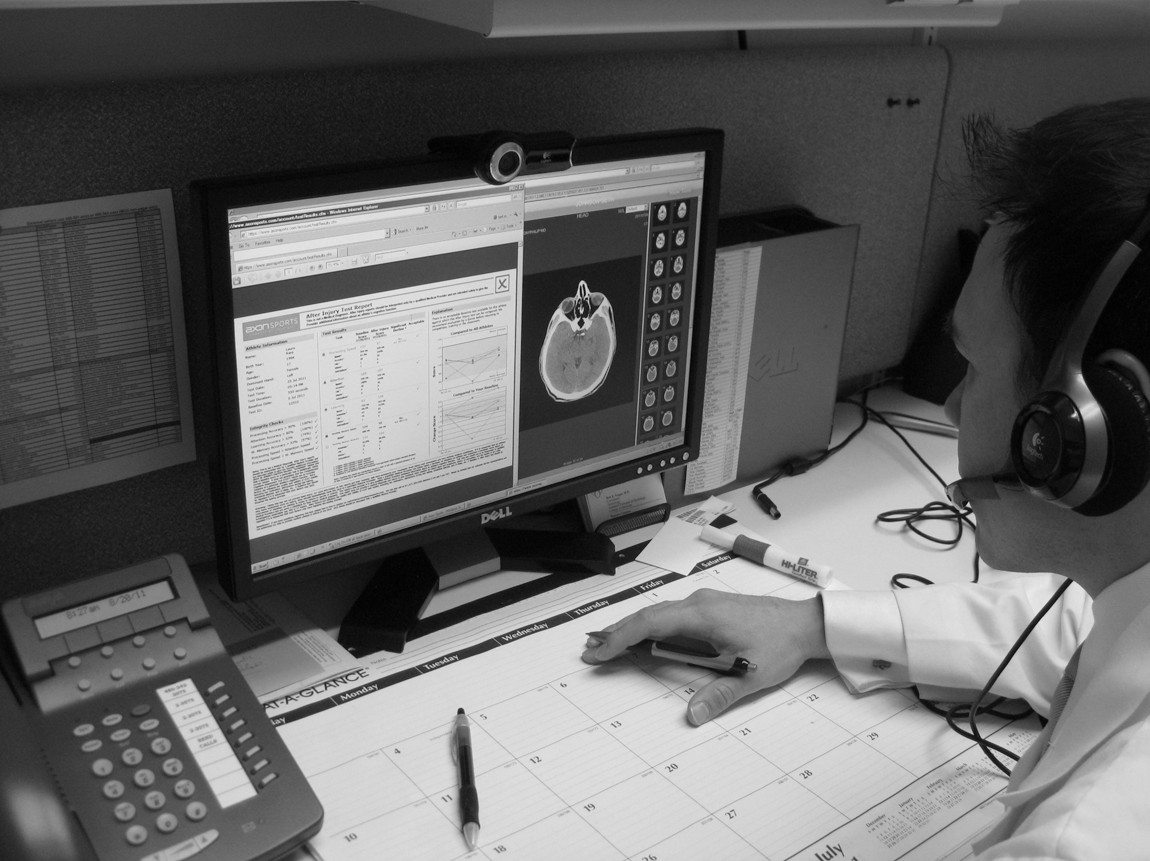
With remote access to the emergency department's Picture Archiving and Communications System and online evaluation of a patient's Computerized Concussion Assessment Tool, the examiner is better equipped to make complex clinical decisions.
Based upon the presence and severity of postconcussive symptoms reported by the patient and observed by his father, information gathered from the physical examination, and performance on the Computerized Concussion Assessment Tool, the patient was advised to refrain from physical activity pending additional workup and face-to-face consultation with a concussion specialist.
Discussion
Telemedicine is a validated and effective means of remotely assessing patients with neurological emergencies and is widely regarded as an effective tool in providing subspecialty care to individuals in rural locations. In particular, telemedicine has been shown to be of great benefit in the management and evaluation of stroke 6,7 and has also proven to be an effective tool in the triage, decision-making, and disposition of patients with traumatic brain injuries. 8,9 Telemedicine is a solution to eliminate the major disparity between urban and rural trauma care and can cover the entire spectrum of care from the site of injury (prehospital care) to the site where the patient is first assessed (rural emergency departments) to the tertiary hospital or dedicated trauma center (definitive care). 10
This case represents the first real-time telemedical assessment, triage, and management of a concussed athlete based on a review of existing literature and also represents the first use of the term “teleconcussion.”
As of May 2012, 38 states have passed legislation aimed at addressing concussion in youth sports including measures to improve the identification and management of concussed athletes. Arizona Senate Bill 1521 specifically mandates the education of student-athletes, parents, coaches, and athletic trainers in concussion awareness and further requires that concussed athletes be cleared for return to play by a healthcare professional trained in the evaluation and management of concussion. As the number of providers with specialized training in the subspecialty of concussion remains relatively small, rural communities are at a distinct disadvantage in obtaining appropriate concussion evaluation in a timely manner. As with many other telemedical applications, teleconcussion helps to bridge this gap in access to specialty care.
With further validation studies, teleconcussion has the potential for numerous practical applications beyond non-emergency, outpatient evaluation of concussed rural athletes. The telemedicine platform is ideal for providing rapid access to a concussion specialist to facilitate sideline assessments and return-to-play decisions at the professional and amateur levels, especially taking into account recent guidelines imposed by the National Football League to seek the opinions of independent neurologists in the assessment of concussed football players.
Outside of athletics, traumatic brain injuries have been reputed to be the signature injury of Operations Iraqi Freedom and Enduring Freedom. 11 Currently, the U.S. Army is pursuing technological solutions for early detection and treatment of traumatic brain injury in order to help address and prevent lasting impacts on military troops and have facilitated a partnership between the U.S. Army Telemedicine and Advanced Technology Research Center and the American Telemedicine Association to conduct a symposium on the topic. 12
Telemedicine technology for teleconcussion assessment should emphasize portability without sacrificing connectivity and security. Traditional telemedicine carts with access through remote desktop or laptop interfaces can adequately serve the technology needs for teleconcussion assessment, but will place unnecessary location restrictions on the examination environment. Mobile tablets and smartphones are prime examples of technology that would allow for remote examinations in a variety of settings. Key requirements for these mobile devices would be encrypted communication to ensure patient privacy, access to Wi-Fi and 3G/4G cellular networks, and videoconferencing software that promotes interoperability between disparate mobile platforms (i.e., Android and iOS).
In the case presented, teleconcussion was useful in identifying a concussed athlete who had begun to resume physical activity ahead of commonly accepted return-to-play guidelines and was helpful in triaging the patient as being symptomatic and in need of a formal face-to-face evaluation and additional workup in order to construct a plan of care and eventual return to play. The development and introduction of teleconcussion to address mild traumatic brain injury in civilian populations have arisen from a preexisting stable foundation of literature describing evidence to support telemedicine applications in the management of moderate and severe traumatic brain injury in the fields of neurosurgery, trauma, neurocritical care, and military medicine. The use of teleconcussion to make formal return-to-play decisions, however, is not validated and should be the focus of further research.
Footnotes
Acknowledgments
We wish to acknowledge the participation and cooperation of Dr. Philip Johnson of the Emergency Medicine Department, Summit Regional Healthcare Medical Center, Show Low, AZ, an affiliate hospital of the Mayo Clinic Telemedicine Network.
Disclosure Statement
No competing financial interests exist.