
Abstract
Introduction
Pre-anesthesia evaluation (PAE) is performed prior to elective surgical procedures, with the objectives of discovering disease, assessing medical readiness, and formulating patient-specific plans, any of which may affect perioperative care. 1 PAE includes interview, review of laboratory and medical records, and directed physical examination. Inadequate PAE is associated with delays, cancellations, 2 –5 and preventable adverse events. 6,7 PAE clinics lower healthcare costs through targeted testing and increased operating room efficiency because inadequate preoperative workup is reported to cause 10–20% of day of surgery cancellations. 8 –10 Criteria select patients who may safely have day of surgery PAE. 1,11 –13
Not all patients whose care could benefit keep their PAE appointments. Seidel et al. 14 reported patients living >60 miles away were less likely to keep PAE appointments than those living <30 miles away. Patients scheduled for PAE spend additional time and incur additional costs not covered by health insurance. These may be significant for patients in a practice that serves a wide geographic area and could contribute to patients deciding to not keep PAE appointments.
Loma Linda University Medical Center is an academic medical center that draws patients from across several hundred miles of San Bernardino and Riverside Counties, California. Surgeons see patients in clinics 35–75 miles distant from Loma Linda, although these patients may be scheduled for procedures at Loma Linda University Medical Center. Typically patient presurgical and PAE visits are scheduled on separate days because travel time from surgical clinics to Loma Linda makes same-day scheduling impractical. Patients who need in-person PAE often make round trips of considerable distance, incurring time off from work, increased childcare demands, and other patient-specific costs or inconveniences. Application of telemedicine could reduce these barriers.
Telemedicine facilitates the exchange of medical information to improve patients' health status 15 and may include two-way video communication, controllable examination cameras, and electronic stethoscopes. A pilot study in remote areas of Canada using telemedicine prior to anesthesia in 10 patients found high levels of satisfaction among patients and providers. 16 A retrospective study of telemedicine PAE in 43 inmates prior to dentoalveolar surgery showed no cancellations or anesthetic complications. 17 Patient acceptance was reported to be high in a pilot trial of telemedicine PAE in 41 patients, with no cancellations from incomplete PAE. 18
A departmental quality review identified missing or incomplete documentation, testing, or consultation related to incomplete PAE as our most common cause of preventable day of surgery delays, with few cancellations. For many patients, preferred providers outside our system must perform testing. Missing results of these tests contribute to day of surgery delays. The impact that changing from in-person to telemedicine PAE has on this preventable delay is unclear. We hypothesized that telemedicine PAE would be associated with better documentation compared with our current in-person PAE, with fewer resultant day of surgery delays. This randomized trial was designed to compare telemedicine with in-person PAE in single-specialty adult surgical patients.
Subjects and Methods
This study was approved by Loma Linda University's Institutional Review Board. Adult patients scheduled for head and neck surgery with the ability to read, write, and speak English were considered for inclusion. Patients provided written informed consent for participation. Patients who met current criteria underwent telephone consultation with a member of the PAE clinic staff and were not included in the analysis. Remaining patients were randomly assigned at the time consent was obtained to in-person or telemedicine PAE on the basis of a computerized random sequence generator (Fig. 1). A nearby single-specialty otolaryngology clinic was used to facilitate comparison and allow for rapid intervention if needed for equipment malfunction while testing this potential practice change. This office is approximately 3 miles distant from the PAE clinic at Loma Linda University Medical Center. Computer networking is inside the Medical Center network firewall in these clinics to allow the highest degree of data security.
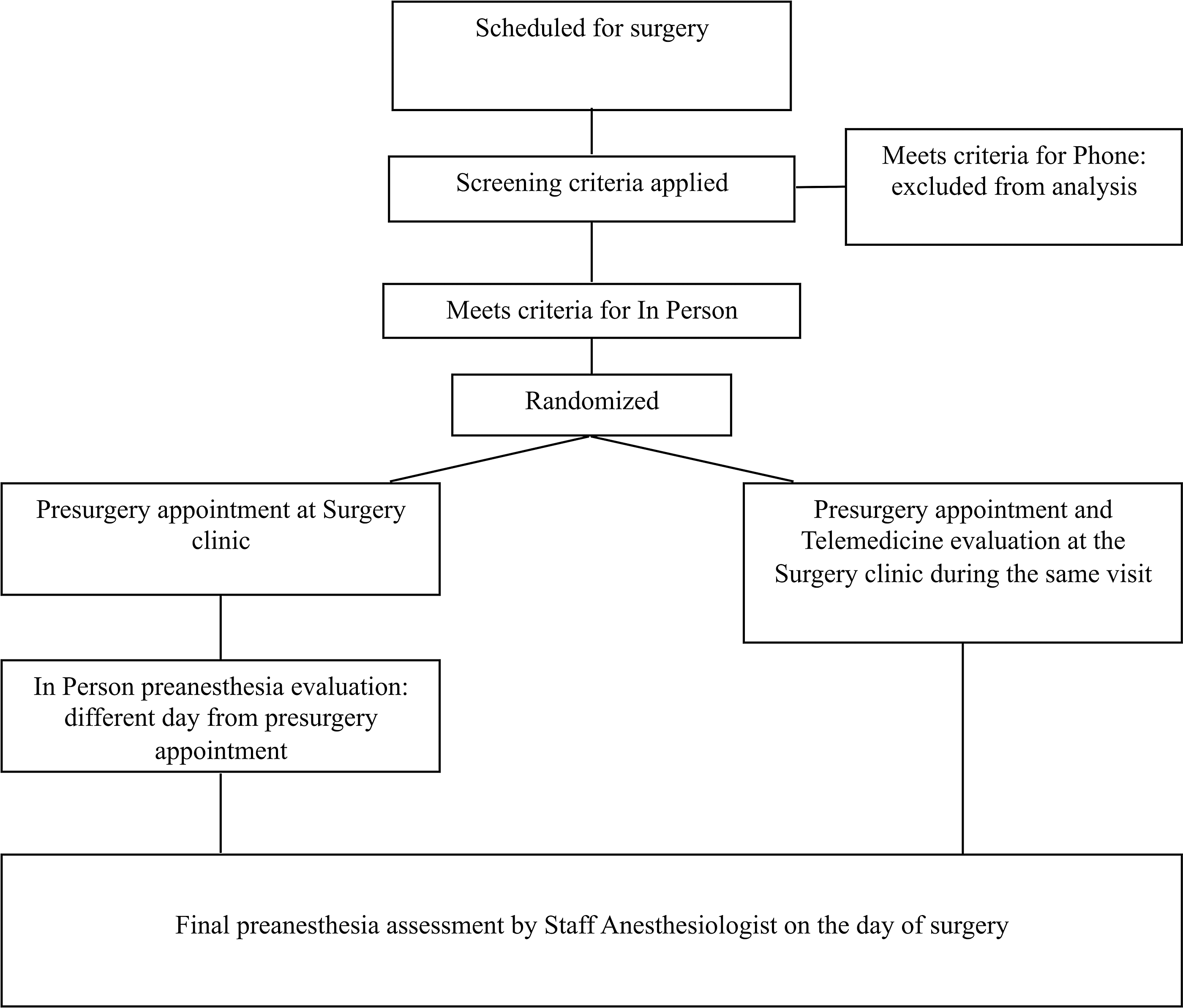
Steps involved in pre-anesthesia evaluation for patients in the two study groups.
The screening PAE is performed by nurse practitioners under standardized procedures or by anesthesiology residents in their first or second year of training, with documentation in the electronic anesthesia record. The PAE format followed consisted of standardized preoperative medical history evaluation along with testing and medical consultation for patient-specific factors, based on published testing recommendations. 1,12,19 Test results available at the time of PAE were reviewed. A screening physical examination was performed including cardiopulmonary examinations and an adapted American Society of Anesthesiologists 11-point airway examination, 20 which assigned 1 point for each abnormal finding. The airway examination was considered predictive of difficulty if the patient was found to have two or more abnormal findings 21 or if the resident or nurse practitioner entered a comment indicating expected difficult airway management. Patients who were medically optimized proceeded with surgery as scheduled. Patients who were not optimized underwent further evaluation prior to surgery with any necessary follow-up scheduled with the PAE clinic. A comment was entered for any anticipated surgical delays. Patients randomized to in-person PAE had their appointment scheduled on a separate day from the presurgical visit, per our current scheduling practice as discussed. Patients randomized to telemedicine underwent PAE immediately following presurgical evaluation while still in the surgical clinic.
Telemedicine equipment was installed at the surgical and pre-anesthesia clinics for this trial. Equipment at the otolaryngology clinic included high-definition pan-tilt-zoom videoconference end point capable of real-time two-way video and audio communications, on a mobile wireless cart. This telemedicine cart included a general examination camera and an electronic stethoscope. To perform the examination, staff at the PAE clinic used videoconferencing software based on the session initiation protocol, which allows mobility. This software was coupled with a high-quality headset to ensure audibility of the heart and lung sounds, which require lower frequencies than standard headsets are capable of reproducing. Data transmission was within the institutional firewall and was AES-128 encrypted (certified by the U.S. Department of Defense). The electronic stethoscope was used for cardiopulmonary examination, whereas a handheld general examination camera was used to complete the adapted American Society of Anesthesiologists 11-point airway examination. Staff at the surgical clinic received training in the use of the telemedicine equipment and electronic stethoscope, along with patient positioning needed for the airway examination to facilitate completion of the PAE.
Staff anesthesiologists were blinded to group assignment and evaluated all patients on the day of surgery, reviewing the medical history and diagnostic data and performing cardiopulmonary and airway examinations. All anesthesia and airway management choices were at the discretion of the staff anesthesiologist assigned to care for the patient. Patients whose anesthetic did not include tracheal intubation were excluded from analysis of airway difficulty prediction. Difficult airway was considered present if a Cormack–Lehane 22 laryngoscopic view >2 was documented. 20,23 Staff anesthesiologists noted delays, cancellations, and perioperative complications. Satisfaction scores using a 5-point Likert scale were obtained from patients regarding PAE experiences, pre-anesthesia staff regarding performance of PAE, and staff anesthesiologists regarding PAE completeness.
The primary outcome measure was inadequate PAE measured as preventable day of surgery delay related to missing documentation, testing, or consultation or physical examination findings that should have been identified during PAE. Secondary measures included prediction of difficult airway, concordance of PAE with day of surgery physical examination findings, and satisfaction scores. A 50% reduction in preventable delays was estimated for sample size calculation, based on our belief that missing documentation could be obtained from the surgeon's office staff during telemedicine PAE. A sample size of 62 patients each for in-person and telemedicine would allow detection of a 50% change in the prior year overall delay plus cancellation rate with power set at 0.80 and p=0.05. Statistical analysis was performed using computerized software (JMP version 8.0.2; SAS Institute, Cary, NC) with p<0.05 considered significant. Normally distributed continuous data were compared using Student's t test, whereas non-normally distributed continuous data were compared using the Wilcoxon test. Ordinal and nominal data were compared using chi-squared analysis.
Results
Between January and September 2010, 200 patients enrolled in the study. Of those, 40 met criteria for telephone screening (20%), leaving 160 to be randomized. Surgery was cancelled after randomization for patient refusal, surgeon availability, or insurance issues for 5 patients who were excluded from analysis (Fig. 2). Intergroup comparisons of the 155 patients analyzed are summarized in Table 1. Seventy-three percent of all patients were ≤65 years of age.
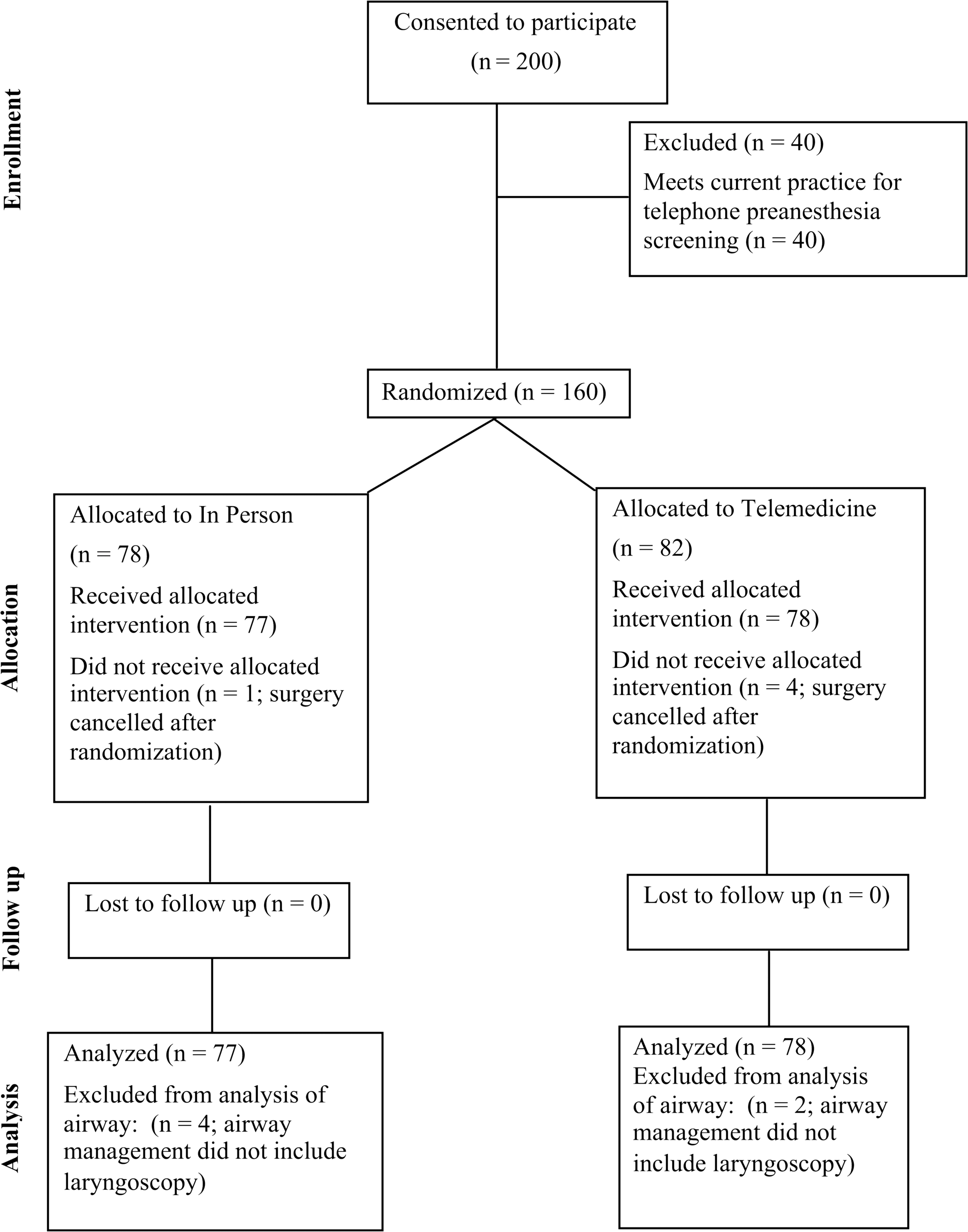
CONSORT diagram.
Intergroup Comparisons
Telemedicine had more men than in-person. Other differences between telemedicine and in-person were not statistically significant.
Intergroup comparisons are by chi-squared analysis.
ASA, American Society of Anesthesiologists; F, female; M, male.
Incomplete PAE caused day of surgery delay in 1 telemedicine patient: PAE identified that results of an echocardiogram were missing but were expected by surgery. Delay occurred because these results were not available on the morning of surgery. Testing was needed or pending at the time of evaluation for 59% of in-person and 34% of telemedicine patients. Overall, PAE and medical optimization were adequate, as no other patients were delayed or had the procedure cancelled on the day of surgery.
Six patients had alternate airway management and were not included in analysis of airway difficulty prediction: monitored anesthesia care, 3 from the in-person group; mask anesthesia, 1 from the in-person group; laryngeal mask airway, 1 from the telemedicine group; and existing tracheostomy, 1 from the telemedicine group. Airway management difficulty was predicted and found equally. Tracheal intubation was successful in 149 patients (Table 1). In 8 of 25 patients with airway difficulty, an experienced provider needed more than two attempts or more than one type of laryngoscope to successfully intubate the trachea. Although screening airway examinations performed in-person more often identified airway management difficulty (4 of 10) compared with telemedicine (3 of 15), the intergroup difference was not significant (p=0.54). The PAE airway examination had low positive predictive value.
PAE staff reported high satisfaction with the ability to obtain history, discuss anticipated problems, and provide instructions for all patients during PAE regardless of group. As seen by the PAE clinician, the telemedicine cameras provided excellent views to allow completion of the airway examination. Day of surgery heart and lung examinations documented by the staff anesthesiologist were highly concordant (>98%) with findings documented in PAE, although PAE staff reported better satisfaction with the ability to hear heart and lung sounds during in-person compared with telemedicine PAE. Patient satisfaction questionnaires were returned by 78.1% of patients. Analysis revealed high satisfaction scores regardless of group (Table 2). Satisfaction with preoperative instructions was higher among in-person patients. Half of respondents reported living at least 25 miles away from the clinic, whereas 26% reported living more than 50 miles away from the clinic.
Patient Questionnaire Responses
Patients indicated satisfaction with pre-anesthesia consultation in both groups, as seen in average scores±standard deviation (on a 5-point Likert scale, where 1=strongly disagree to 5=strongly agree). Time between presurgical visit and pre-anesthesia evaluation and distance between home and clinic was self-reported.
Analysis was by t test except for number responding and distance between home and clinic, which was by chi-squared analysis.
Discussion
Similar to prior reports, we found only one delay in telemedicine PAE and none for in-person PAE. Overall, we found less frequent delay than in other adult patients seen in our PAE clinic during 2010. This supports the potential for telemedicine PAE to provide information needed for safe anesthesia care while decreasing patient travel. It is possible that participation in the study introduced a modifying effect on the practice of the nurse practitioner at the surgical clinic. Having one nurse practitioner perform the presurgical visits eliminated the potential for interindividual variability from staff at the surgeons' office. The nurse practitioner may have consulted our PAE testing and consultation guidelines more diligently for patients enrolled in the trial, which may explain the approximately 40% fewer telemedicine patients who had results missing at the time of PAE. Alternatively, the nurse practitioner may have been subtly influenced by requests for added testing or documentation made during telemedicine visits as a quality check of documentation for patients sent for in-person visits. Either behavior could have contributed to our finding only one day of surgery delay related to incomplete testing or documentation. Regardless, our results suggest changing to telemedicine PAE would not introduce more delays when institutional PAE testing and consultation guidelines are followed. As we found, previous studies report high levels of patient satisfaction, with no evidence of a negative impact on surgery delay or cancellation. 16 –18 However, prior studies did not randomize comparison with in-person consultation, nor did they report cardiopulmonary and airway examination findings.
Airway examination is an important component of PAE risk assessment with significant planning implications. When prediction of possible difficult airway anatomy is communicated, day of surgery delay may decrease as precautionary preparation can be made before the patient arrives to the operating room. We found airway management difficulty in 25 (16.7%) of our patients who underwent laryngoscopy, similar to the higher prevalence of airway difficulty reported in head and neck compared with general surgery patients. 24 Telemedicine and in-person airway examinations were equivalent, although in-person had greater calculated sensitivity. The sensitivities found are similar to those reported in a meta-analysis of bedside screening tests. 21 Sensitivity of the screening airway examination may reflect the experience level of nurse practitioners and residents performing these examinations, and not the telemedicine equipment, as the examination camera provided good views of airway anatomy. As we did not collect reasons for alternate airway management, we are not able to determine if the staff anesthesiologist found airway abnormalities that prompted avoidance of tracheal intubation in the 6 patients with alternate airway management. If so, and if these 6 patients then had airway management difficulty, sensitivity would have changed to 36% for in-person and 29% for telemedicine, based on recorded PAE airway examinations in these patients. The predictive value of the airway examination performed during telemedicine PAE may be improved if it is performed by staff anesthesiologists, which could be the focus of future research. The low sensitivity of screening airway examinations in both groups suggests final evaluation by staff anesthesiologists remains an important safety measure.
Telemedicine patients had no difficulty communicating with the PAE clinic staff and reported high overall satisfaction. PAE clinic staff reported high satisfaction with PAE performed via telemedicine. Although satisfaction with heart and lung examinations using the telemedicine electronic stethoscope was lower than for in-person evaluation, this did not appear to be a significant limitation, as physical examination findings were documented as highly concordant with the day of surgery examination.
We use criteria to select patients who are younger and healthier for telephone PAE, with over 50% of our scheduled patients screened by telephone. In the present study, 20% of enrolled patients met criteria for telephone PAE screening, implying the study group was less healthy than our overall practice. The current in-person evaluation requires at least one additional trip to Loma Linda for patients who live at a distance. The benefits of telemedicine PAE to patients and family can include fewer appointments, less travel time, and less time off work. Yen et al. 25 reported 48% of 46,000 patients screened by telephone would need to take a day off from work to keep PAE appointments prior to surgery, with <10% willing to make an extra trip. This group averaged 40 (median, 25) miles between home and the surgery center. As half of our patients reported living over 25 miles away from the clinic and over three-quarters of our study group were of working age (under 65 years old), elimination of in-person PAE and associated time off from work could provide significant benefit to many of our patients. The potential lost income and lost productivity are accompanied by potential costs related to travel and childcare. These added costs may be significantly increased for patients living in rural areas who travel several hours for each appointment.
Generalization of our findings is subject to several limitations. We relied on self-reported travel distance to the clinic, did not measure time off from work, and did not measure associated costs related to travel or childcare, so we can only infer potential economic benefits of telemedicine PAE. However, when the distance between surgical and PAE clinics is large, PAE and presurgical visits are scheduled on different days; thus patients who work likely lose at least half a day of work. Other systems may have different processes that would have to be evaluated compared with ours. We studied patients from a single specialty clinic, which limits comparison between groups of surgical patients. We found very few abnormalities on heart and lung examination, none of which was discordant, limiting our ability to assess the adequacy of heart and lung examination by telemedicine. Although we did not discover abnormal findings by telemedicine stethoscope examination, patients in other specialty clinics may have a higher prevalence of preexisting cardiovascular disease, suggesting further research is needed to determine if similar concordance of physical examination findings would be obtained. Cancellation and delays may be greater than we found in patients scheduled for surgery from other surgical specialty clinics. Although satisfaction reported by telemedicine patients was high, consistent with previous reports, 16 –18 the lower response rate from in-person patients may confound analysis of intergroup satisfaction differences.
Telemedicine PAE can provide high patient satisfaction with potential patient time and cost saving benefits compared with in-person PAE. These were not associated with an increase in day of surgery delays compared with in-person PAE for adult patients undergoing head and neck surgery in our system. Based on these findings, a prospective trial enrolling patients from multiple surgical specialties is warranted.
Footnotes
Acknowledgments
The authors thank Dr. W. William Hughes, Dean, Loma Linda University School of Pharmacy, for loan of the telemedicine equipment used at the otolaryngology clinic for this trial. This study was supported by the Department of Anesthesiology and the Department of Otolaryngology/Head and Neck Surgery, Loma Linda University School of Medicine
Disclosure Statement
R.L.A. II, B.G., J.L.R., J.N., B.W., T.-A.D., and G.S. report no conflicts of interest. R.P. provides consultation to and has previously served on Boards of the American Medical Association and serves on the board of NORCAL Mutual Insurance. D.S.R. discloses that as cofounder/developer of a telemedicine system used to evaluate stroke patients at rural hospitals, he has received royalties from REACH Health, Inc., for financial activities outside the submitted work. No resources or other support were received from REACH for any aspect of this study. J.F. is Principal in Med-RT, LLC. In this role he has provided services and consultation to hospitals, including Loma Linda University Medical Center.