
Abstract
Introduction
Remote monitoring is a promising approach to improve the treatment of patients with heart failure. 1,2 Some heart failure patients are recipients of cardiac implantable electronic devices, such as implantable cardioverter-defibrillators (ICDs) or cardiac resynchronization therapy defibrillators (CRT-Ds). These devices are capable of automatic or semi-automatic data transfer from their diagnostic memory to physician-accessible Web sites, allowing for remote device and patient monitoring. 3 –7 One such option, the Biotronik (Berlin, Germany) Home Monitoring® (HM) system, transfers relevant data automatically on a daily basis. The HM system has been shown to shorten substantially the time from the onset of relevant medical and technical events to physician evaluation 6,8 and to allow longer in-office follow-up intervals without compromising patient safety. 6 It also facilitates the early detection of arrhythmias, including atrial fibrillation, 6,9,10 and enables a remote analysis of intracardiac electrograms recorded by the implanted devices. 11
Studies investigating the implementation of HM into clinical routines 6,9,12,13 showed that HM can be efficiently used to change in-clinic workflow and to reduce long-term treatment costs. 12,14 High-volume clinical or hospital facilities typically dedicate specialized teams to remote follow-up. 12 It has been suggested recently that such institutions could provide monitoring services for several smaller clinical sites. 13 Another possibility is to outsource the daily analysis of HM data to a competent telemedical service provider. The provider would interpret HM data according to clearly defined procedures and conduct telephone interviews with the patient if the data suggest the need for this. This method would add information about symptoms to the automatically transmitted HM information. Although a key strength of HM is the reliable daily data flow resulting from its fully automatic operation, a service provider may extend the range of information available and might be better posed than the attending physician for applying a rigorous telephone interview strategy that delivers reproducible results.
The performance and clinical acceptance of centralized telemedical service centers for actively contacting ICD and CRT-D patients have not been studied systematically. The aim of the present study was therefore to evaluate the three-party cooperation among (1) the patient whose implanted device automatically sends HM messages to the HM Service Center (HMSC), (2) a telemedical service center (TmSC) engaged to verify and filter HM findings, and (3) the study site that handles the HM data forwarded by the TmSC. The acceptance of the TmSC by the patient and the clinician and the frequency and category of HM findings reaching the sites per patient-month were the primary objectives of this study.
Subjects and Methods
The Early Detection of Cardiovascular Events in Device Patients with Heart Failure (detecT-Pilot) Study was a prospective, multicenter, non-randomized, observational study involving 10 German sites and 1 TmSC (Vitaphone GmbH, Mannheim, Germany). Ethics committee approval was granted before the study's start, and all patients gave their written consent. To be enrolled, patients had to be in New York Heart Association functional class II or III, have a left ventricular ejection fraction of 40% or less, and have an indication for the implantation of a dual-chamber ICD or CRT-D. Patients were excluded if they had permanent atrial fibrillation, acute coronary syndrome, planned cardiovascular surgery, uncontrollable blood pressure, untreated severe valvular disease, or restrictive, infiltrative, or hypertrophic cardiomyopathy.
According to the individual indications, either a dual-chamber ICD or a CRT-D from the Lumax® family (Biotronik) with integrated HM capability was implanted. Device programming was left to the responsibility of the physician. Initial HM alert criteria were prespecified, but physicians were allowed to modify these settings according to the clinical need. The schedule and scope of follow-ups adhered to the institutional standards. All patients remained in the study until the last included patient had completed 6 months of follow-up.
Remote Monitoring and TMSC Role
The HM technology has been described previously. 4,5,12,15 In brief, a short-range radio transmitter (402–405 MHz, Medical Implant Communication Service band) embedded in the implanted device emits once per day at a programmed transmission time or after certain events, a message containing relevant diagnostic data. The data are received by a patient device containing a Medical Implant Communication Service receiver and a GMS mobile phone. After the received data are encrypted and compressed, the patient device forwards them automatically and without any patient involvement, in the form of one or several short message service texts to the HMSC. The HMSC displays the incoming data as trends on a secure Web site and sends e-mail, fax, or short message service notifications (“HM alerts”) whenever the data meet certain user-defined criteria. In a typical setting, only the patient's physician has access to the HM Web site and receives HM alerts (Fig. 1A).
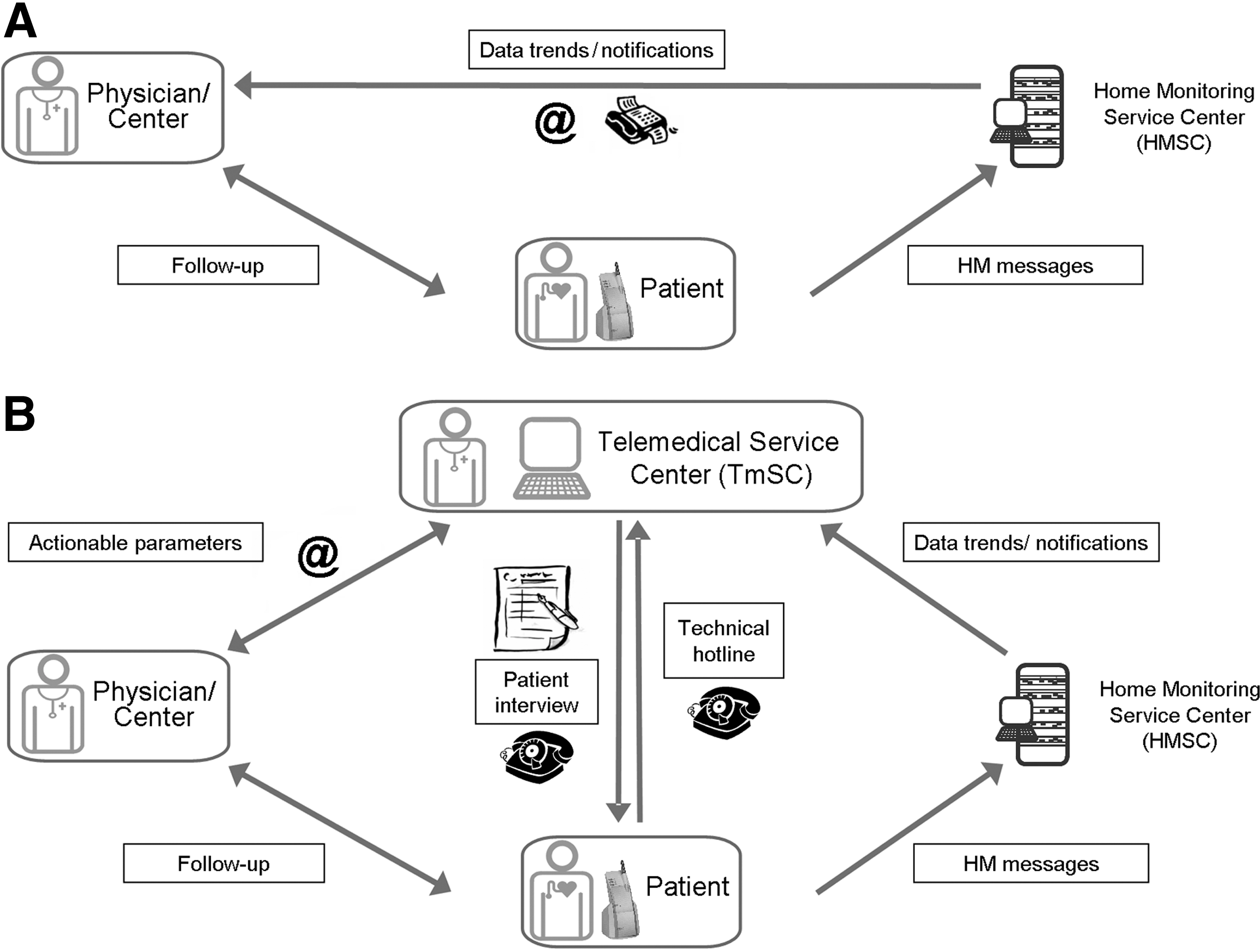
In the present study, HM data flow differed from that in the routine practice. Instead of the patient's physician, the TmSC received alerts from the HMSC and had access to the online HM data trends (Fig. 1B). After appropriate initial training on HM and study procedures, the medical professional staff at the TmSC analyzed alerts and data trends. The staff was familiar with the clinical and medical history of study patients, including medication. A supporting cardiologist was part of the staff.
The TmSC contacted the patients by telephone at the beginning of the study (welcome call) and again if the automatic transmission of HM data was interrupted. In response to certain HM findings, the TmSC staff conducted a short structured patient interview comprising four questions related to the patient's general well-being, dyspnea, ankle swellings (each covering the last 3 days), and drug compliance. If two or more of these items were unfavorable, the status was defined “possibly worsening.” The forwarding of potentially relevant information to clinical sites was managed according to an array of actionable parameters (APs) predefined by the study protocol (Table 1).
Management of Actionable Parameters at the Telemedical Service Center
A standardized questionnaire focusing on heart failure symptoms was used. The attending physician was informed if it showed that the patient's status was “possibly worsening.”
In patients with a known history of atrial fibrillation (AF).
In patients without a history of AF.
Instruct the patient to solve the problem through appropriate handling of the patient device, or ascertain that the underlying cause is the patient's absence from home. In the case of continuing significant problems, inform the physician.
Assessed by the physician on duty at the telemedical service center.
bpm, beats/min; CRT-D, cardiac resynchronization therapy defibrillator; DR-ICD, dual-chamber implantable cardioverter-defibrillator; ERI, elective replacement indicator; HM, home monitoring; IEGM, intracardiac electrogram; LV, left ventricular; RA, right atrial; RV, right ventricular; VF, ventricular fibrillation; VP, ventricular pacing; VR, ventricular rate; VT1, slow ventricular tachycardia; VT2, fast ventricular tachycardia; WHF, worsening of heart failure.
The first AP category involved a pilot algorithm for early detection of acute worsening of heart failure (WHF). Constructed for study purposes only, this algorithm combined the mean heart rate and the patient activity time assessed by the device's accelerometer sensor, to produce one value every day using the formula a×(mean heart rate) – b×(activity duration). If the slope of the linear regression of these values for the last 7 days was above a predefined threshold value, the algorithm generated this specific AP. Upon receiving it, the TmSC conducted the structured patient interview and informed the patient's physician of the “possibly worsening” status of the patient. Although aimed at evaluating the patient's acceptance of the interviews conducted by the TmSC, this AP was not expected to show particular diagnostic value for the clinical management of the patient. As for all other AP categories, the reaction to the pilot WHF algorithm was left to the physician.
The second AP category was related to atrial fibrillation (Table 1). Depending on the history and current burden of atrial fibrillation, the TmSC either interviewed the patient or forwarded the HM finding immediately to the study site.
The third AP category was HM data transmission failure during ≥3 consecutive days. The TmSC instructed the patient on how to solve this problem or ascertained that the underlying reason was the patient's absence from home (e.g., holidays or hospital stay). The patient's physician was informed only in the case of continuing transmission problems.
Alerts belonging to the fourth AP category (essential HM alerts, including technical issues and ventricular arrhythmia/therapy) were immediately forwarded by the TmSC. If the cardiologist on duty at the TmSC found that an arrhythmia was misclassified by the implanted device (based on the intracardiac electrogram), the study site was contacted directly. Also, alerts of the fifth AP category (pacing percentages) were forwarded immediately. Like in routine clinical practice, the patient's physician could disable HM alerts deemed less important, for instance, the alert to high ventricular pacing occurrence in an ICD patient who had developed permanent atrioventricular block. For technical reasons, the pilot WHF algorithm could not be disabled. The physician, however, could instruct the TmSC to suspend this algorithm in a patient after five or more false alarms.
Feedback from Study Sites and Patients
The physicians were asked to rate the clinical relevance of each AP received from the TmSC as high, medium, low, or none and to indicate if the AP led to a clinical action. A string of the same APs in a patient could be reported in a single case report form. By definition, additional or rescheduled face-to-face follow-up, hospitalization, or reprogramming of the implanted device was considered as an action, but not a telephone contact alone. At the end of the study, TmSC acceptance by patients and physicians was measured using purpose-designed questionnaires.
Statistical Methods
The data are presented using descriptive statistics. For continuous data, the mean values and standard deviation are provided. For categorical data, the absolute and relative frequencies are calculated. The rates of individual APs or groups of APs were calculated as the total number of the respective events in all patients divided by the cumulative study duration for all patients. Only the rate of all APs was calculated from the patient-individual rates, to express it as mean±SD and allow a statistical comparison between the ICD and CRT-D groups. No study hypothesis has been defined. The sample size of 55 patients was chosen to ensure that the TmSC would receive approximately 150–300 alerts per month from the HMSC, which was considered a sufficient number to work efficiently.
Results
Patients
Fifty-five patients, 46 of them male (84%), with a mean age of 65±11 years, were enrolled through March 2010. All patients had symptomatic heart failure and were in New York Heart Association class II (n=16 [29%]) or III (n=39 [71%]). Thirty-five patients (64%) received CRT-D devices. Forty-seven patients (86%) had an indication for primary prevention of sudden cardiac death. Eight patients (15%) had a known history of atrial fibrillation. Major cardiovascular medications at baseline were beta-blockers (in 85% of all patients), diuretics (83%), angiotensin converting enzyme inhibitors (72%), and digitalis (29%).
Follow-Up and HM Transmission Success
The enrolled patients were followed up for a mean of 402±200 days. The cumulative follow-up was 727 patient-months. Five patients died, resulting in an annual mortality rate of 8.3%. Three patients dropped out because of acute myocardial infarction (n=1) or residence change (n=2). No patient withdrew consent. Study data collected until patient death or dropout were included in the analysis.
HM messages were received on 82.5% of all days after HM initialization. One frequent reason for transmission gaps was that during their absence from home (e.g., holidays or hospital stay), patients typically did not take the patient device along with them.
Management of APS at the TMSC
No relevant violations of the protocol-defined procedures by the TmSC were recorded. Several additional telephone calls were conducted by the TmSC to clarify situations not provided for by the study protocol. On the other hand, some patients actively contacted the TmSC to report on issues such as an upcoming absence from home.
The most frequent AP type in this study was the pilot WHF algorithm. This AP was issued 2,037 times (53% of all APs), necessitating 489 phone calls by the TmSC (48% of all phone calls). In 20 instances, the patient interviews indicated symptomatic worsening, and the sites were informed accordingly (Table 1). Atrial fibrillation alerts were the second most frequent AP category, with 799 alerts (21% of all alerts) necessitating 299 patient calls (29% of all calls). The study site was informed in 25 instances. Furthermore, all “pacing percentage” alerts (629 occurrences [16% of all alerts]) were forwarded to study sites (accounting for 88% of all forwarded APs), except for a few alerts issued after the physician had asked to inactivate it.
All essential HM alerts were forwarded to study sites, accounting for 3% of all APs. HM transmission gaps accounted for 6% of APs and were all managed by the TmSC with the exception of 1 patient who was managed by the study site.
The normalized numbers of APs handled at the TmSC per patient-month were as follows: 2.80 (pilot WHF algorithm), 1.10 (atrial fibrillation), 0.87 (pacing percentage), 0.34 (transmission gaps), and 0.17 (essential HM alerts). The normalized numbers of patient calls per patient-month were as follows: 0.67 (pilot WHF algorithm), 0.41 (atrial fibrillation), and 0.32 (transmission gaps).
Feedback from Study Sites
The mean number of APs forwarded to study sites was 1.04±1.55 per patient-month. There was no significant difference between ICDs and CRT-Ds (1.11±1.72 versus 1.00±1.47 APs, respectively; p=0.81). As presented in Table 2, the numbers of “sent” and “judged” APs differed from each other, especially for the pacing percentage category for which the physicians frequently used a single case report form to judge jointly on successive events in the same patient. Of the total of 122 judgments for individual or clustered APs, 35 were classified as having high or medium relevance. Clinical action was initiated in 46 APs related to tachyarrhythmia detection (15 ventricular arrhythmia, 5 recurrent atrial fibrillation, and 2 new-onset atrial fibrillation), inadequate percentage of ventricular pacing (16 in CRT-Ds, 2 in ICDs), pilot WHF algorithm (n=4), and lead impedance out of range (n=2).
Feedback from Study Sites and Actions Taken
Possible actions included change in in-clinic follow-up schedule, hospitalization, or reprogramming of the implanted device. Telephone contact alone was not counted as action.
In patients with known history of atrial fibrillation (AF).
In patients without history of AF.
bpm, beats/min; CRT-D, cardiac resynchronization therapy defibrillator; DR-ICD, dual-chamber implantable cardioverter-defibrillator; HM, home monitoring; LV, left ventricular; RA, right atrial; RV, right ventricular; VF, ventricular fibrillation; VP, ventricular pacing; VR, ventricular rate; VT1, slow ventricular tachycardia; VT2, fast ventricular tachycardia; WHF, worsening of heart failure.
TMSC Acceptance by Patients and Physicians
At the end of the study, 48 patients completed a TmSC-related questionnaire. In total, 64% of patients had the impression of an overall better care owing to the TmSC, and 73% had a feeling of increased security (Fig. 2). Of 55 enrolled patients, 54 were contacted by the TmSC at least once (Fig. 3); the number of contacts ranged up to one in every second day in a patient with recurrent atrial fibrillation episodes. No correlation was found between the number of contacts and the acceptance of the TmSC by patients (data not shown).

Forty-eight patients and 17 physicians from 10 sites filled out purpose-designed questionnaires at the end of the study. HM, home monitoring; TmSC, telemedical service center.
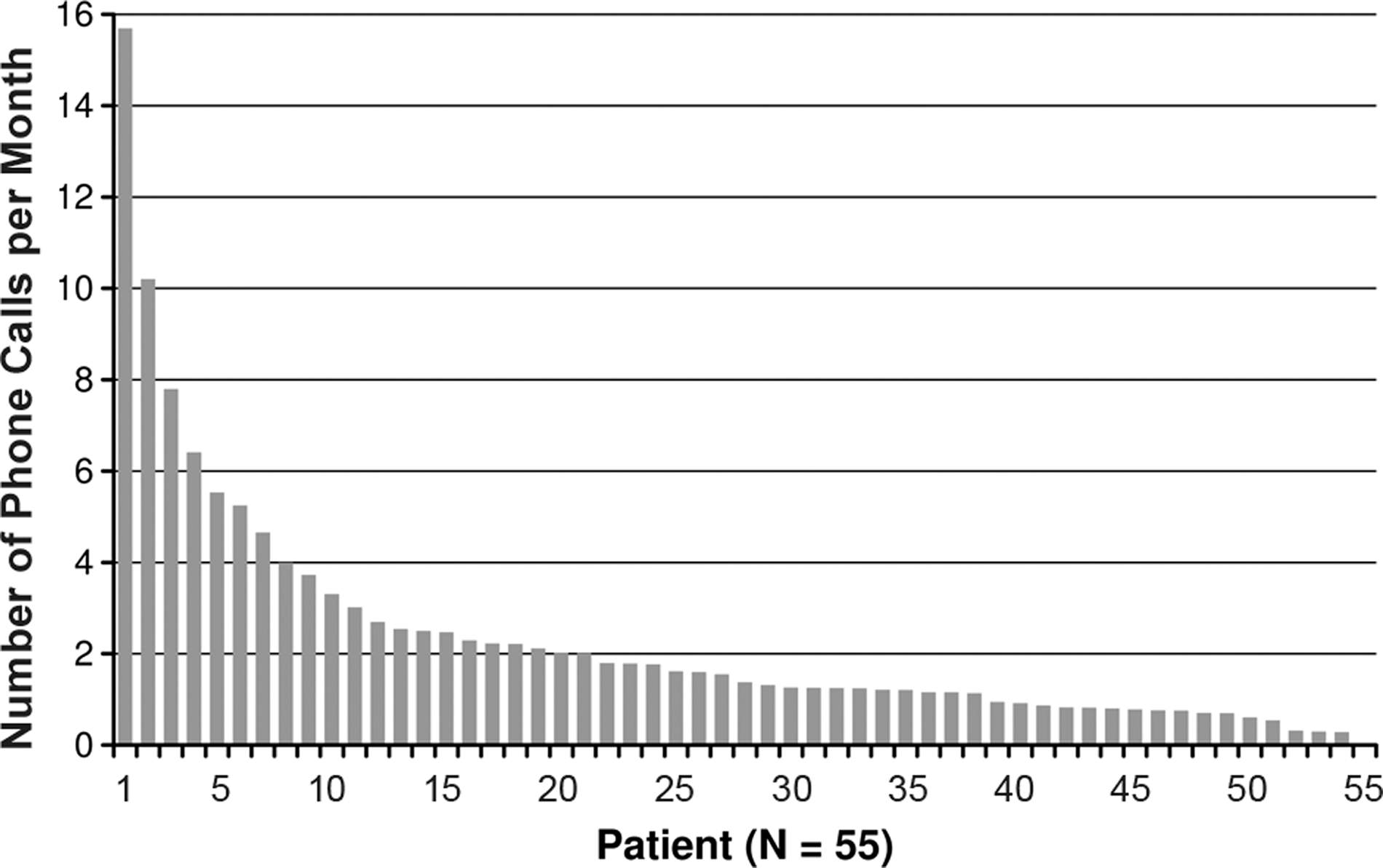
Distribution of the number of telephone contacts between the telemedical service center and study patients. Each bar represents 1 patient.
Among 17 physicians from 10 sites, 65% had the impression that the TmSC contributed to an overall better patient care (Fig. 2). The majority of physicians appreciated the improved feeling of security for the patient (82%), a faster reaction to HM messages (71%), and a more time-efficient use of HM (71%). Furthermore, nearly half of physicians felt they were able to improve treatment efficacy and their relationship to the patient owing to the timely receipt of relevant information from the TmSC, compared with potentially infrequent HM data analysis by their own in a busy clinical routine. Conversely, about 20% of physicians did not experience a benefit from the cooperation with the TmSC.
Discussion
In patients with heart failure and implanted CRT-Ds or ICDs, the combination of a fully automatic remote monitoring system and a TmSC providing alert filtering and patient calls was investigated. The acceptance of TmSC among patients and physicians was good. Two-thirds of both groups concluded that the studied concept led to better patient care. The TmSC maintained a high level of protocol compliance throughout the study period. The average number of alerts forwarded to the clinics per patient-month was 1.04. This figure is well within the range of 0.14–2.10 reported from different studies of the same remote monitoring system 3,12,15 –18 and is primarily influenced by study procedures, population characteristics, and device types. 15
The volume of data provided by the investigated remote monitoring system (Biotronik HM) is growing because of the fact that more patients receive HM-equipped devices. In addition, newer-generation devices transmit more data than older ones. Continuous improvements of the HMSC Internet platform help with data management. The user can limit the number of alerts online, by tailoring the alert criteria to the individual patient's conditions. Furthermore, a traffic light system guides the user through the information, which is summarized for a focused review. Nevertheless, resources are required for continuous remote patient monitoring, which may be especially challenging in clinics without dedicated personnel. Vogtmann et al. 13 evaluated the feasibility and safety of centralized HM surveillance by a dedicated clinical monitor center, where HM data from patients of nine satellite clinics were screened and filtered. The authors found that centralized HM was feasible and safe and may enable continuous surveillance for smaller sites that have limited workforce. 13 Although our concept differs from the one investigated by Vogtmann et al., 13 both studies indicate feasibility of external support in handling HM data.
The HM system shows an excellent compliance, with data successfully transmitted on 80–90% of all days, 12,13,15,18 likely because of the ability of the system to operate without the patient's cooperation. We have now shown that it is possible to complement the automatically captured HM data with patient feedback, if needed. No patient compliance issues arose because the patients did not need to initiate the telephone contacts. It is important that no patient withdrew from the study.
Significant effort is currently being made to develop predictors for heart failure decompensation. Attempts have so far not been successful, 19 –21 but new promising parameters for improved algorithms are under investigation, including hemodynamic parameters 22,23 or minute ventilation abnormality. 24 Our concept might allow identification of critical patients among those with parameter deviations, whereas reliable and fully automatic predictors have not yet been found. Because of the clearly defined tasks of the TmSC and the structured interview it used, the TmSC-based concept should deliver reproducible results. With daily transmissions and its fully automatic operation, HM appears to be the ideal platform to develop predictive algorithms for heart failure decompensation. 25 However, once the data indicate a critical deviation from expected values, a telephone contact to the patient may be helpful for the diagnosis. It can be conducted by the attending physician. But, our study suggests that this contact, be it for data transmission problems, atrial fibrillation, or other parameters indicating deterioration of the patient's status, can also be provided for by a third party, if exact procedures are defined.
Study Limitations
As there was no control group, the patients' appreciation of the TmSC may have been biased by their overall opinion about the device therapy and HM. Second, as no alternative predictive algorithm was available, we constructed the pilot WHF algorithm merely for the purpose of the present study. As expected, the algorithm had no power to make predictions about the patient's status, generating a large number of alerts. The frequent alerts and interviews may have reduced the patients' appreciation of the TmSC because of general lack of correlation between the received calls from the TmSC and their own symptoms.
Conclusions
An external service provider operating according to a strict, predefined procedure can support the management of patients with cardiac implantable electronic devices under remote monitoring surveillance. Accepted by the majority of physicians and patients, this concept may be helpful in gaining symptomatic information on top of automatic HM data and in supporting smaller clinics in the follow-up of their device patients.
Footnotes
Acknowledgments
The study was supported by Biotronik SE & Co KG, Berlin, Germany. The authors acknowledge the contribution of Jochen Proff for input on study design, Sabrina Streller to study management, Jürgen Schrader, PhD, to data analysis and manuscript review, and Dejan Danilovc, PhD, to medical writing assistance.
Disclosure Statement
S.-S.S. has received speaker's fees from Medtronic, St. Jude Medical, Boston Scientific, and Biotronik. H.N. has received a study grant from Biotronik. A.N. is an employee of Biotronik, Germany. M.A. is an employee of Vitaphone, Germany. A.M., A.G., C.P., T.K., W.S., C.v.B., M.H., S.S., and T.L. have no competing financial interests.