
Abstract
Introduction
Endobronchial ultrasound-guided (EBUS) transbronchial fine needle aspiration (TBFNA) has emerged as the procedure of choice for establishing diagnosis as well as staging of locally advanced malignant lung neoplasms and in the assessment of mediastinal lesions. 1,2 Rapid on-site evaluation (ROSE) with cell block preparations is effective in optimization of EBUS-TBFNA specimen procurement and processing. 3,4 Micames et al. 5 demonstrated in a large meta-analysis that ROSE increased sensitivity of EBUS-TBFNA from 80% to 88% without compromising the procedure length. On-site assessment not only enables a highly accurate preliminary diagnosis of malignancy for samples obtained under endoscopic ultrasound guidance but also contributes to enhanced diagnostic yield of samples for ancillary studies such as immunohistochemical analysis, bacterial cell cultures, flow cytometry, and gene rearrangement studies for unsuspected cases of lymphoma. 6
EBUS-TBFNA procedures are time consuming and adversely affect time management for cytopathologists. 7,8 Distances of EBUS suites from the pathology laboratory can make timely assessment by an on-site cytopathologist difficult. Even though collaboration of a bronchoscopist and the ROSE cytopathologist is essential for optimizing the yield and efficiency of EBUS-TBFNA, the staffing, time, and cost constraints have precluded the availability of ROSE in every institution.
Dynamic telepathology systems focus on transmission of live images that are viewed electronically in real time at a remote site, in contrast to static telepathology systems that are based on capturing of images in a digital format and then transmitting them to distant observers. 9 Advancements in telepathology technology have made it feasible to use dynamic telepathology for cytologic specimens. However, most studies using dynamic telecytopathology have been retrospective. 10,11 Only a few studies have focused on the application of dynamic telecytopathology for initial real-time on-site diagnosis in aspiration cytology. 12 –16
In this study we present our experience with use of dynamic telecytopathology for preliminary on-site evaluation and diagnosis of EBUS-TBFNA and compare it with conventional microscopic ROSE by a cytopathologist.
Materials and Methods
The study involved EBUS-TBFNA performed by a pulmonologist (R.L.) at a remote EBUS suite located on the third floor of the north wing of the hospital and evaluation of slides by the cytopathologist located in a cytopathology laboratory on the sixth floor of the south wing (a block away from the EBUS suite) of the hospital. The on-site cytotechnologist prepared cytology smears that included Diff-Quik (Mercedes Medical, Sarasota, FL)–stained slides and alcohol-fixed smears that were later stained with the Papanicolaou method in the laboratory. Each EBUS-TBNA pass involved endoscopic visualization of the lesion (adjacent to the tracheobronchial tree) with high-frequency ultrasound imaging and obtaining cytological samples from the lesion. The total number of Diff-Quik–stained slides prepared on site ranged from two to four slides per pass. Additional material was collected for cell block as needed. On average, three passes (range, two to eight) were performed per procedure. Each pass was evaluated separately irrespective of use of the telecytopathology system or conventional on-site method for immediate assessment. Additional passes were performed only if the prior pass did not yield adequate material for preliminary diagnosis. In contrast to the conventional on-site method, which required the cytopathologist to be physically present at the EBUS suite to evaluate the slides prepared on-site, telecytopathology assessment could be performed from the cytopathologist's office or any computer accessible through the hospital's ethernet network. The time spent for review of each pass during telecytopathology or conventional microscopic preliminary interpretation was recorded. This study received institutional review board exemption.
Case Selection
Telecytopathology was introduced in our remote endoscopy suite on November 2009. We evaluated all consecutive cases of EBUS-TBFNA that underwent telecytopathology on-site assessment from November 2010 to September 2011. We also reviewed the same number of consecutive cases of EBUS-TBFNA that had conventional microscopic on-site evaluation prior to introduction of telecytopathology at our remote EBUS suite.
The telecytopathology system consisted of an Olympus (Olympus America, Center Valley, PA) CX41 microscope and a digital camera with NetCam software (Olympus) (Fig. 1). A 2.11-megapixel cooled digital color camera (Olympus DP20) was used for image acquisition with the microscope (Olympus CX41) and a Dell (Round Rock, TX) desktop computer with a direct ethernet connection. NetCam software used a transmission control protocol/Internet protocol (IP) to transmit live images over the Internet via an assigned static IP address (Figs. 2 and 3). The computer and the image server required log-in, and the IP address was known to the faculty or the operators of the microscope. The original size of the acquired image was 1600×1200 pixels, with the NetCam-transmitted image having a resolution of 1600×1200 pixels.
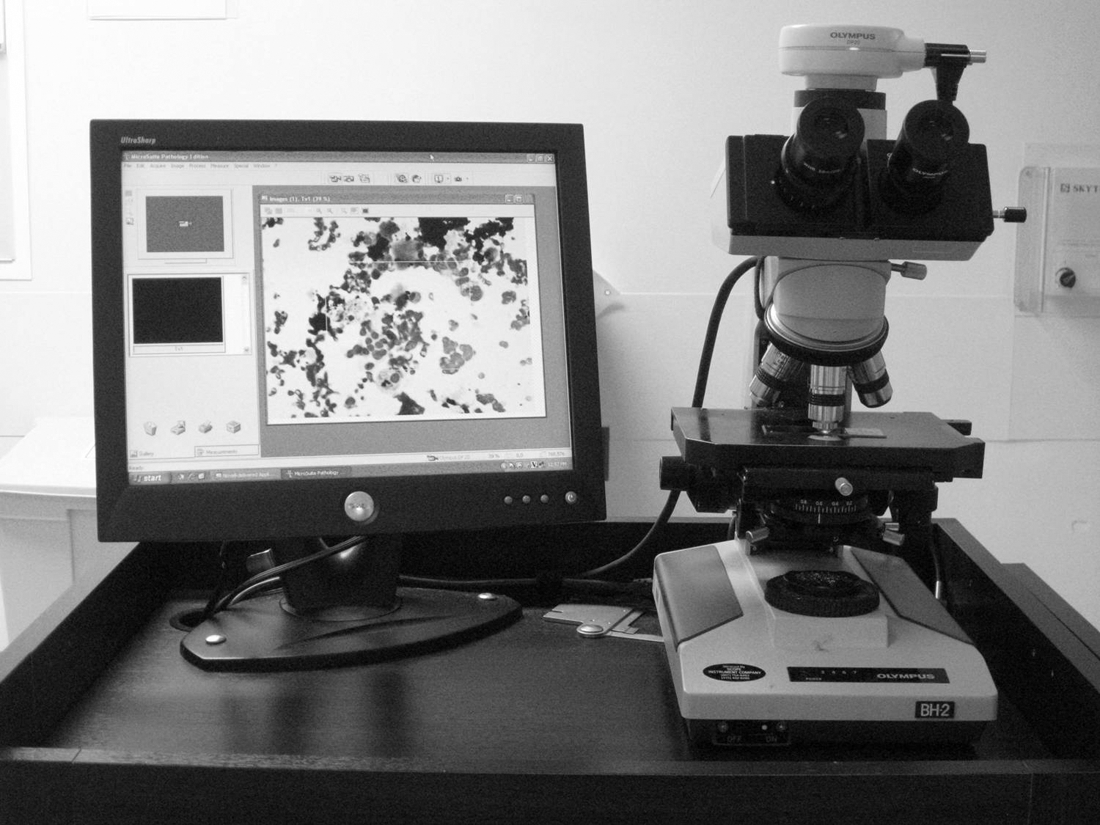
The telecytopathology digital system comprises an Olympus camera and a monitor with microscope.

Small cell carcinoma involving the subcarinal lymph node in an endobronchial ultrasound-guided transbronchial fine needle aspiration specimen viewed remotely on a computer screen using the telecytopathology digital system (Diff-Quik stain).
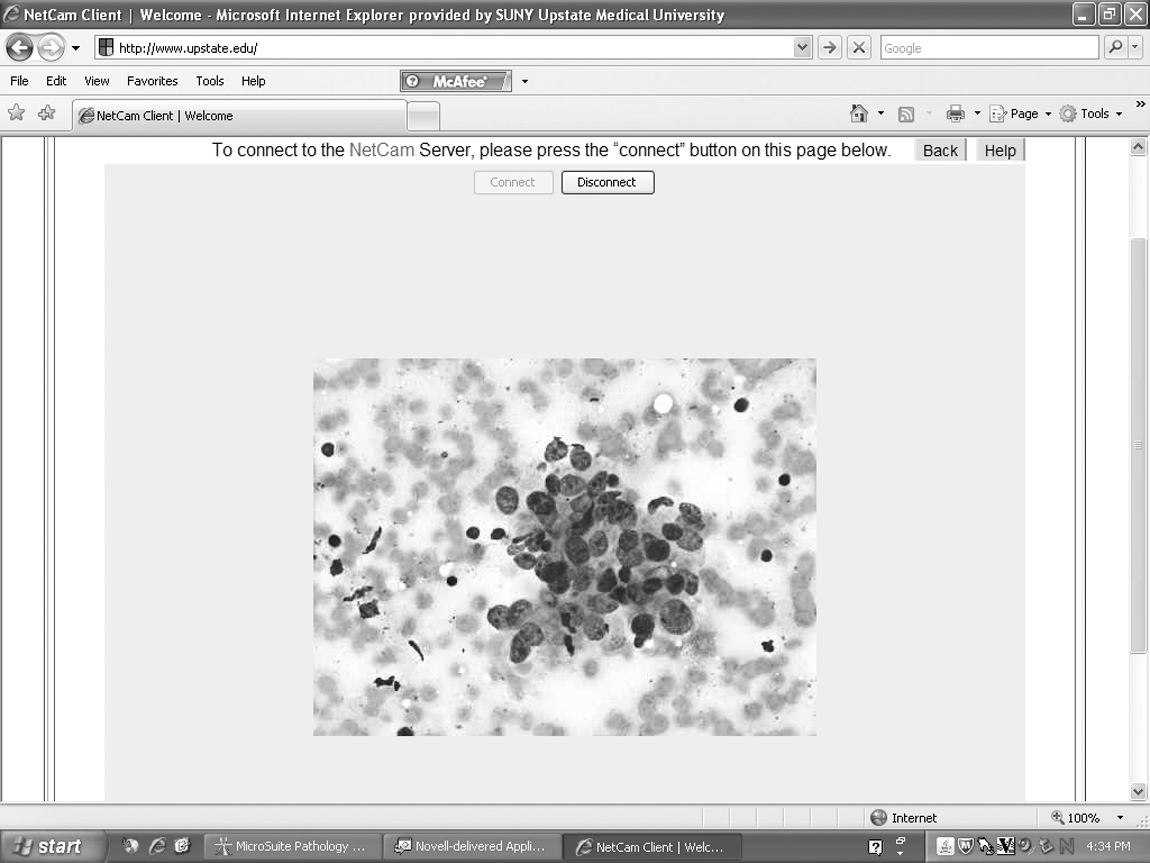
Metastatic non–small cell carcinoma viewed remotely on the computer screen using the telecytopathology digital system (Diff-Quik stain).
Different cytotechnologists with 12–20 years of experience and well conversant with the telecytopathology system operated the microscope at the remote site. The cytopathologists (K.K.K. and A.K.), with experience in aspiration cytology of EBUS-TBFNA, could not control the microscope or camera and interacted with the cytotechnologist via the Vocera (San Jose, CA) voice communication system, which enabled hands-free, voice-controlled wireless voice communication using the wearable Vocera B3000. The preliminary diagnosis was communicated to the bronchoscopist (R.L.). The images were transmitted continuously without any lag time as the cytotechnologist moved the slide on the stage and the pathologist could view on the desktop screen what the cytotechnologist was seeing at the microscope. The Olympus microscope had objectives from ×4 to ×40. Low-power objectives of ×10 and ×4 were used to assess overall cellularity of the smears and to identify areas that may require review under a higher-power ×40 objective for better cytologic details.
Diagnostic cytology categories that were used for preliminary on-site evaluation and final cytologic diagnosis were as follows: 1. Benign: cases yielding benign lymphoid elements with or without granulomas. 2. Suspicious or atypical: cases with cytologic features suspicious for malignancy or cases with atypical cytologic features where malignant neoplasm could not be excluded. 3. Malignant: cases with obvious cytologic features of malignancy. 4. Unsatisfactory: cases that contained predominantly blood or rare poorly preserved cells or crushed fragments of tissue or lacked site-specific tissue (e.g., no lymphocytes identified in a specimen designated lymph node).
The initial and final cytologic interpretations for the majority of the telecytopathology cases were performed by two cytopathologists (K.K.K. and A.K.). Although the conventional cases were diagnosed by three other faculty cytopathologists in addition to K.K.K, the initial and final interpretations on these cases were also rendered by the same cytopathologist in accordance with the practice at our institution.
Statistical Analysis
Accuracy was defined by agreement between the preliminary and final interpretations in the two groups. Suspicious or atypical category cases were considered concordant if the final diagnostic category was the same or malignant. All case slides on discrepant cases that did not meet the criterion for concordance as stated above were reviewed to assess the cause of discrepancy. The association between the three preliminary diagnostic categories (benign, suspicious/atypical, and malignant) and the two diagnostic methods (telecytopathology and conventional) was analyzed using Pearson's chi-squared statistic. Because the suspicious/atypical cells have expected counts of less than 5, an exact p value was obtained via Monte Carlo simulation. 17 The proportions of concordance between preliminary and final diagnoses for telecytopathology and conventional methods were compared using relative risk, and a corresponding 95% confidence interval was constructed based on large sample theories. The mean, standard deviation, and range for the time spent for review of each pass with conventional and telecytopathology preliminary interpretation were computed, and statistical significance of the mean between two groups was determined using t test. All computations were performed using SAS/STAT proc freq software (version 9.2) of the SAS system for Windows (SAS Institute, Cary, NC).
Results
There were 100 consecutive EBUS-TBFNA cases evaluated by telecytopathology from November 2009 to July 2011 and 100 consecutive cases with conventional on-site evaluation from April 2008 to October 2009. The time spent for review of each pass ranged from 2 to 4 min in both telecytopathology and conventional microscopic preliminary interpretation.
Table 1 compares the preliminary diagnosis rendered via telecytopathology and conventional on-site microscopy. There was no statistically significant difference (exact p value=0.54) in proportion of cases (telecytopathology versus conventional microscopy) in the benign, atypical/suspicious, malignant, and unsatisfactory categories.
Preliminary Diagnostic Categories Used for On-Site Evaluation by Telecytopathology and the Conventional Method
Pearson's chi-square statistic for the association between rows and columns is 0.99 with a Monte Carlo simulation–based exact p value equal to 0.54, which was calculated based on the exact inference of the contingency table shown.
Table 2 shows the follow-up final cytologic diagnosis on all EBUS with the preliminary diagnosis rendered via telecytopathology. All cases with initial telecytopathology diagnosis of malignant (24 cases) and benign (58 cases) corresponded with a final cytologic diagnosis of malignant and benign, respectively. Twelve of the 14 cases with an initial telecytology diagnosis of atypical or suspicious corresponded with a final cytologic diagnosis of malignant (12 cases) and benign (2 cases). Of the 4 cases with an initial telecytopathology diagnosis of unsatisfactory, in 2 cases there was correspondence with an unsatisfactory diagnosis on final cytology, and 2 cases were reclassified as malignant. In summary, the final cytologic diagnosis in the telecytopathology group was 60% benign, 38% malignant, and 2% unsatisfactory.
Preliminary On-Site Telecytopathology and Final Cytologic Diagnoses
Table 3 shows the follow-up final cytologic diagnosis on all EBUS-TBFNAs with preliminary diagnosis rendered via conventional on-site microscopy. All cases with an initial conventional on-site diagnosis of malignant (31 cases) corresponded with a final cytologic diagnosis of malignant. Of the 10 cases with an initial cytologic diagnosis of atypical/suspicious, final cytologic diagnoses were as follows: atypical or suspicious (1 case) and malignant (9 cases). Of the 57 benign cases with an initial cytologic diagnosis of benign, in 51 cases there was correspondence with a benign diagnosis on final cytology, and 6 cases were reclassified as malignant. In summary, the final cytologic diagnosis in this group was 52% benign, 46% malignant, and 2% unsatisfactory.
Preliminary Conventional On-Site and Final Cytologic Diagnoses
The accuracy rate of preliminary telecytopathology and conventional on-site microscopy diagnosis was 96% (96/100) and 93% (93/100), respectively (Table 4). The relative risk is 1.03 with a 95% confidence interval of (0.97, 1.10), which is within the commonly selected equivalence bound (0.8, 1.25). Thus we are confident from a statistical point of view that the concordance rates are comparable between the two evaluation methods.
Summary of Concordance Pairs for Telecytopathology and the Conventional Group
These calculations were generated from the data in Tables 2 and 3 . Cases were considered concordant if the final diagnostic category was the same as the preliminary one or if the final diagnostic category was malignant when the preliminary diagnostic category was atypical/suspicious. The relative risk regarding the concordance rates between the method groups is 1.03 with a 95% confidence interval of (0.8, 1.25).
Analyses of causes of discrepancy in the preliminary and final interpretations in telecytopathology cases and on-site conventional microscopy cases are given under the review column in Tables 5 and 6, respectively. The causes of discrepancy in small cell carcinoma were attributable to the difficulty in the distinction of crushed fragments of tumor cells in the background of polymorphous lymphocytes from reactive lymphoid elements. Papanicolaou-stained slides highlighted the salt and pepper chromatin pattern that aided in diagnosis of small cell carcinoma. Cell block material when available allowed immunostaining for chromogranin and synaptophysin to confirm the neuroendocrine nature of the tumor cells.
Discrepancies Between Preliminary Telecytopathology and Final Cytologic Diagnoses
Discrepancies Between Preliminary Conventional On-Site and Final Cytologic Diagnoses
Cell block material captured tissue fragments of tumor cells with architectural details that aided in the diagnosis of cases of adenocarcinoma and squamous cell carcinoma that were initially assessed with conventional microscopy. Obscuring acute inflammation precluded recognition of tumor cells on Diff-Quik stain in a case of poorly differentiated large cell carcinoma. Immunostains performed on cell block material facilitated recognition of tumor fragments with large pleomorphic tumor cells. In the case of metastatic renal cell carcinoma, a few scant vacuolated tumor cells were initially misinterpreted as histiocytes during telecytopathology assessment. A case of lymphoma was interpreted as reactive lymphocytes at the time of initial assessment with the conventional microscopic method; however, flow cytometry performed on additional material collected in RPMI solution at the time of on-site evaluation revealed a monoclonal population of lymphocytes consistent with B cell lymphoma.
Reactive bronchial epithelium was interpreted as atypical or suspicious in 2 cases and 1 case during initial assessment with telecytopathology and conventional microscopy, respectively.
The average time spent for review of each pass with telecytopathology and conventional microscopy for preliminary interpretation was 2.89±0.85 min (range, 2–4 min) and 2.80±0.76 min (range, 2–4 min), respectively, and was not statistically significant (p>0.05).
Discussion
Increasing numbers of studies in the recent cytology literature have demonstrated the usefulness of dynamic and static telecytopathology systems to review cytology smears remotely over an Internet connection. 10 –16,18 –23 Dynamic systems appear to be more accurate compared with static systems. 8,9,24
In the current study we performed ROSE of EBUS-TBFNA specimens, exclusively, via a dynamic live and remotely operated telecytopathology system and compared it with on-site evaluation by a pathologist using conventional microscopy. We demonstrated comparable and high diagnostic accuracy in both groups. Kern et al. 16 compared rapid evaluation using telecytology of transbronchial and computed tomography–guided lung fine needle aspiration specimens with a group of similar specimens that did not receive on-site assessment. They concluded that rapid evaluation using telecytology improves the diagnostic yield of guided fine needle aspiration biopsies by decreasing the percentage of non-representative specimens. Our study reaffirms the use of telecytopathology as a valid substitute for ROSE via EBUS-TBFNA.
Discrepancies between on-site preliminary diagnosis and final diagnosis were identified using both telecytopathology and conventional microscopy assessment methods and can be categorized as interpretative difficulties, paucity of material, and lack of availability of additional material on Papanicolaou-stained slides and cell block material. Similar discrepancies were noted in a prior study on aspirates from various body sites by Alsharif et al. 12 Interpretative difficulties and importance of collection of additional material for ancillary studies for diagnosis of transbronchial aspirates using conventional microscopy have been well described. 25 The importance of additional Papanicolaou-stained slides for review of cytologic features and collection of material for ancillary studies (e.g., flow cytometry or cell block material for immunostains that facilitated final diagnosis in all discrepant cases) cannot be overemphasized.
The success of telecytopathology depends on the experience of the on-site operator (e.g., an experienced cytotechnologist or senior resident with an interest in cytopathology or a cytopathology fellow) who can effectively operate the slides on the on-site microscope, transmit real-time images, and project significant findings while being in audio contact with the attending cytopathologist. 12 Also, the pathologist must be well familiarized with the use of telecytopathology for interpretation of real-time images. In our study, both the pathologist and the on-site operator were familiarized with the use of the telecytopathology system. The pathologist did not perceive any difficulty in interpretation of the real-time online images due to their high quality and resolution. Our study shows that an experienced surrogate (cytotechnologist, senior resident, or cytology fellow) can manage field selection for telecytopathology by being in audio contact with the cytopathologist who will render the final report.
The difference in the average time spent for review of each pass in both telecytopathology and conventional microscopic preliminary interpretation was not statistically significant. However, in contrast to conventional microscopic initial evaluation, where the pathologist is required to be physically present in the EBUS suite, telecytopathology preliminary interpretation allowed the cytopathologist to use dead time between passes (which ranged from 5 to 20 min) to perform other routine office work, including sign out of routine cases. Telecytopathology also offered the opportunity to discuss the difficult cases with colleagues who can view the real-time images from any computer within the hospital network system.
Under current practice, staff cytopathologists alone are able to bill (Current Procedural Terminology code 88172 or 88177) for passes performed during telecytopathology services as long as they participate in preliminary evaluation of these passes and assess the need for additional passes to obtain material for cytologic diagnosis and ancillary studies. 26 The results of these preliminary evaluations have to be communicated to the physicians performing the procedure. Staff cytopathologists are legally responsible for all cases in which they provide diagnostic services, including telecytopathology.
In summary, we demonstrate that on-site telecytopathology preliminary evaluation for EUS-TBFNA appears to be highly accurate and comparable with conventional microscopic preliminary interpretation. Interpretative difficulties, scant material, and lack of Papanicolaou-stained slides and cell block material at the time of on-site evaluation represent common limitations of both conventional microscopy and telecytopathology preliminary evaluation of EUS-TBFNA that may contribute to diagnostic difficulties in a few cases. Our study supports use of telecytopathology as a valid substitute in ROSE of EBUS-TBFNA. The low cost of the telecytopathology equipment (approximately $6,000, excluding the microscope) makes it a cost-effective alternative in situations where distance and time constraints may preclude cytopathologists from rendering preliminary on-site evaluations at distant and multiple locations.
Footnotes
Acknowledgments
We would like to thank Ms. Cindy Steele, cytopathology laboratory supervisor, for help with retrieval of data for this study.
Disclosure Statement
No competing financial interests exist.