
Abstract
Lacking compliance with liquid intake restrictions is one of the major problems in patients on hemodialysis and causes an increased mortality. In 120 patients on hemodialysis with an average interdialytic weight gain (IWG) exceeding 1.5 kg on at least 2 days during the 4 weeks preceding the intervention, the effect of telemetric body weight measurement (TBWM) on IWG, ultrafiltration rate, and blood pressure was evaluated over a period of 3 months. Patients of the telemetric group (TG) were supplied with automatic scales, which transferred the weight via telemetry on a daily basis. In the case of IWG of more than 0.75 kg/24 h, a telephonic contact was made as required, and in the case of an IWG of more than 1.5 kg, telephonic contacting was obligatory along with the advice of a liquid intake restriction to 0.5 L/day until the next dialysis. The patients of the control group (CG) received standard treatment without telemetric monitoring. We examined specific data of the second interdialytic interval (IDI2) and the average within 1 week. The average difference of IWG between TG and CG was not significant before the start of the study but 0.2 kg (p=0.027) (IDI2)/0.27kg (p=0.001) (WP) at the end of the study, respectively. The average difference in the ultrafiltration rate within 1 week was 19.0 mL/h (p=0.282) (IDI2)/8.2 mL/h (p=0.409) before the start of the study but 28.4 mL/h (p=0.122) (IDI2)/30.9 mL/h (p=0.004) at the end of the study, respectively. Thus, TBWM is a feasible method for optimizing the IWG and reducing the ultrafiltration rate.
Introduction
Patients with end-stage renal failure on hemodialysis frequently suffer from a compelling sensation of thirst. Therefore the desired liquid intake due to the reduced patient's urine production is often exceeded. More than 74% of patients in hemodialysis have difficulties with their liquid intake restriction. 1,2 Elevated liquid intake correlates with an increased interdialytic weight gain (IWG) in the form of hypervolemia. 2 The increased weight gain can be seen as an indicator for nonadherence to the liquid intake restrictions. 3 Poor liquid intake compliance has a negative effect on the long-term survival in patients on hemodialysis. 4 There is a correlation between an increased IWG and an increased mortality, which was shown in large studies. 5,6 It was also shown that there is a 35% increased death risk due to weight gain. Furthermore, increased IWG results in the need for higher ultrafiltration rates (UFRs).
Patients having UFRs over 12.37 mL/h/kg of body weight have an increased mortality. 7 The long-term prognosis related to acute myocardial infarction and coronary heart disease is also impaired by high UFRs. 8 The noncompliance with liquid intake restrictions is a considerable risk factor for acute hospitalization due to hypervolemia (for example, pulmonary edema, hypertensive crisis, and myocardial infarction). 9
It is also a risk for cardiac long-term damage (diastolic and systolic heart failure, left ventricular hypertrophy) 10 –13 and dialysis-associated events such as a mortality-increasing hypotension, 14 –16 muscle cramps, 17,18 and ischemic complications because of the required high filtration rates. Furthermore, 60–90% of dialysis patients suffer from hypertension, in particular, systolic hypertension, 14 which is often not adequately controlled with antihypertensive medication. In this situation, a consequent reduction of the daily liquid intake is recommended 19 to achieve an appropriate blood pressure decrease. 20
End-organ damage caused by recurrent hypervolemia and high blood pressure undulation under hemodialysis increases the already elevated morbidity and mortality. 15,21 The current approaches to assist liquid intake compliance are not able to solve the issues observed in the daily routine of nephrology practice. 22,23 The application of telemetric transmission of self-measured body weight via modern telecommunication technology and information technology between physician and patient is a new indication. We hypothesize that telemetric body weight measurement (TBWM) can improve compliance and thus reduce morbidity and mortality in patients under hemodialyses.
Preliminary results from this study have been presented previously in abstract form. 24 –28
Patients and Methods
Patients and Study Design
After consent of the local ethics committee at the Georg-August-University Göttingen (Göttingen, Germany) and education and written consent of the patients, 120 patients with end-stage renal failure requiring hemodialysis (>6 months, three times a week) and who experienced an average weight gain of at least 1.5 kg during the 2-day interval between the second and third dialysis in the course of the week (second interdialytic interval [IDI2]) within the last 4 weeks before inclusion in the study were randomized in two groups in this monocentric (Center of Nephrology Göttingen), prospective, open body weight telemetry study (Table 1).
Patient Population After Randomization in the Telemetric Body Weight Measurement Group and in the Control Group
Data are number of patients or mean±standard deviation values as indicated.
BMI, body mass index; D, two dialysis sessions a week; F, femaleM, male; MI, methodological noncompliance.
Both groups received standard care including body weight measurement directly before and after dialysis treatment in the dialysis center (EDI-63™; Waegetechnik Kohn Ltd., Siegen, Germany) (scales accurate to 0.1 kg). The telemetry group (TG) was additionally supplied with telemetric weight monitoring. Patients were instructed to weigh their body weight under possibly equal terms daily before and after dialysis and once daily on days without dialysis at a time corresponding to the start of the dialysis. The observation period was 3 months for each patient.
The dialyses were carried out with a Nikkiso DBB 05 hemodialysis machine (Nikkiso Medical Ltd., Tokyo, Japan) in combination with a kidney low-flux dialyzer (FX 8; Fresenius Medical Care AG & Co. KGaA, Bad Homburg, Germany). Blood pressure measurements were carried out with a Stabil-O-Graph™ (IEM Ltd., Stolberg, Germany).
TBWM
Patients of the TG were supplied with TC 100 Mobil™ (IEM Ltd.) scales. The scales offer an accuracy of measurement of 0.1 kg. The mean deviation is ±0.2 kg with a standard deviation of 0.06 kg. The scales are equipped with a Bluetooth® (Bluetooth SIG, Kirkland, WA) interface for data transmission to Bluetooth-compatible mobile phones, which were handed to the patients. Once a patient carried out a successful measurement with the TC 100 Mobil scale, data transmission was initiated automatically (Fig. 1).
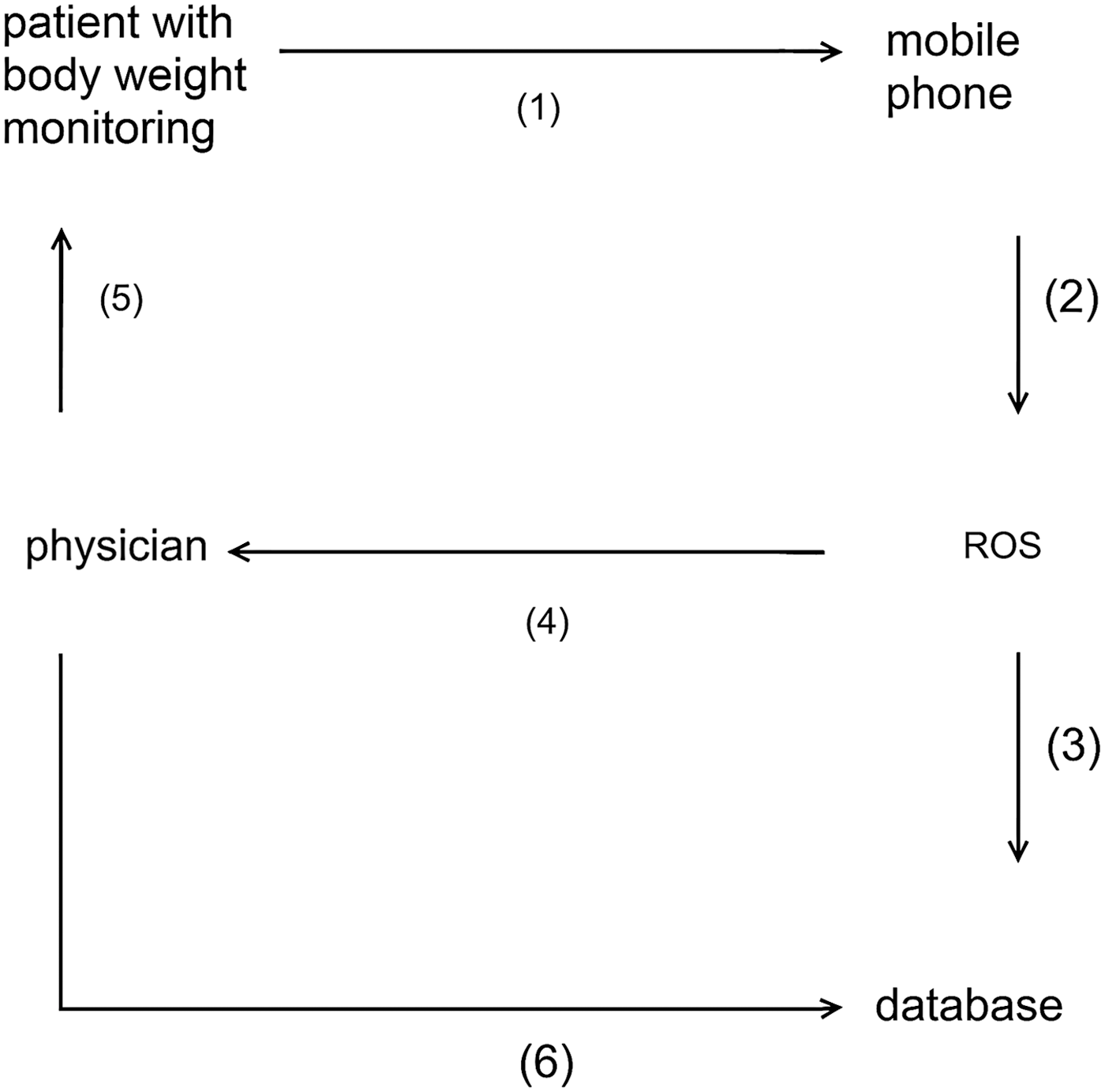
Concept of data management. (1) The patient's weight is sent from the scale via Bluetooth to a mobile phone, (2) which sends the encrypted blood pressure data via short message service to the remote operating system (ROS). (3) The ROS decrypts the data and transfers them to the central data bank. (4) If the weight is beyond the alarm limit, an alarm is generated, which is sent as e-mail from the ROS to the physician, (5) who can, in the case of an alarm, contact the patient and ask about liquid intake compliance and the state of his or her health. Moreover, further procedures can be discussed. (6) At any time the physician is able to access all data in the database via a Web interface.
Alarm Algorithms
In the case of a weight gain of more than 0.75 kg between two measurements, an alarm report was sent to the physician by e-mail. The weight gain was then discussed at the next dialysis appointment or on the telephone. An alarm report was generated once a day at most. If measurement was missed for more than 3 days, a warning of underusage was sent to the physician. Furthermore, a monthly report and a weekly report of the patient's weight parameters were generated. The status reports were handed to the patients during dialysis, and the results were discussed. If a weight gain exceeded 1.5 kg between two measurements, an intervention via phone was mandatory. For a weight gain between 0.75 kg and 1.5 kg, an individual decision on intervening was made depending on the patient's profile and the other interdialytic weight changes.
Study End Points
Primary study end points were the IWG during the IDI2 per week and the average ultrafiltration. Secondary end points were blood pressure characteristics during dialysis.
In order to monitor the course of a patient's weight gain between the dialyses, the weight change between the second and third dialysis in the course of the week, subsequently termed IDI2, was analyzed separately. Furthermore, the unfiltered data obtained between any two dialyses were analyzed as well. For the IDI2 the last four dialyses were used; for the unfiltered data the last 12 dialyses were used. Four datasets measured in the IDI2 and 12 unfiltered data sets correspond to measurement over 4 weeks, respectively. This makes it easier to compare with data obtained in the 4-week period preceding the study.
Statistical Analysis
All of the statistical analyses were performed using SPSS software (SPSS for Windows version 11.5.1; SPSS Inc, Chicago, IL). The data were analyzed using t tests for independent samples. Homogeneity of variances was checked using Levene's test. The normal distribution assumption was analyzed via the Shapiro–Wilk test as well as the Kolmogorov–Smirnov test, using the correction of the significances by Lilliefors.
Results
Interdialytic Weight Gain
During the study the IWG (IDI2) was reduced from 2.22±0.84 kg to 2.11±0.84 kg in the TG (p=0.474), whereas in the control group (CG) a small rise from 2.29±1.08 kg to 2.33±1.08 kg (p=0.839) was observed. The unfiltered data show a reduction of the weight gain from 2.41±1.01 kg to 2.31±0.94 kg in the TG (p=0.575) and a weight gain from 2.53±1.32 kg to 2.58±1.25 kg in the CG (p=0.831) (Figs. 2 and 3). The mean difference in weight gain between the groups was 0.07 kg (p=0.198) for the IDI2 at the beginning of the study and 0.22 kg (p=0.027) at the end of the study. The mean difference in weight gain for the unfiltered weekly data was 0.12 kg (p=0.072) at the beginning of the study and 0.27 kg (p<0.001) at the end of the study.
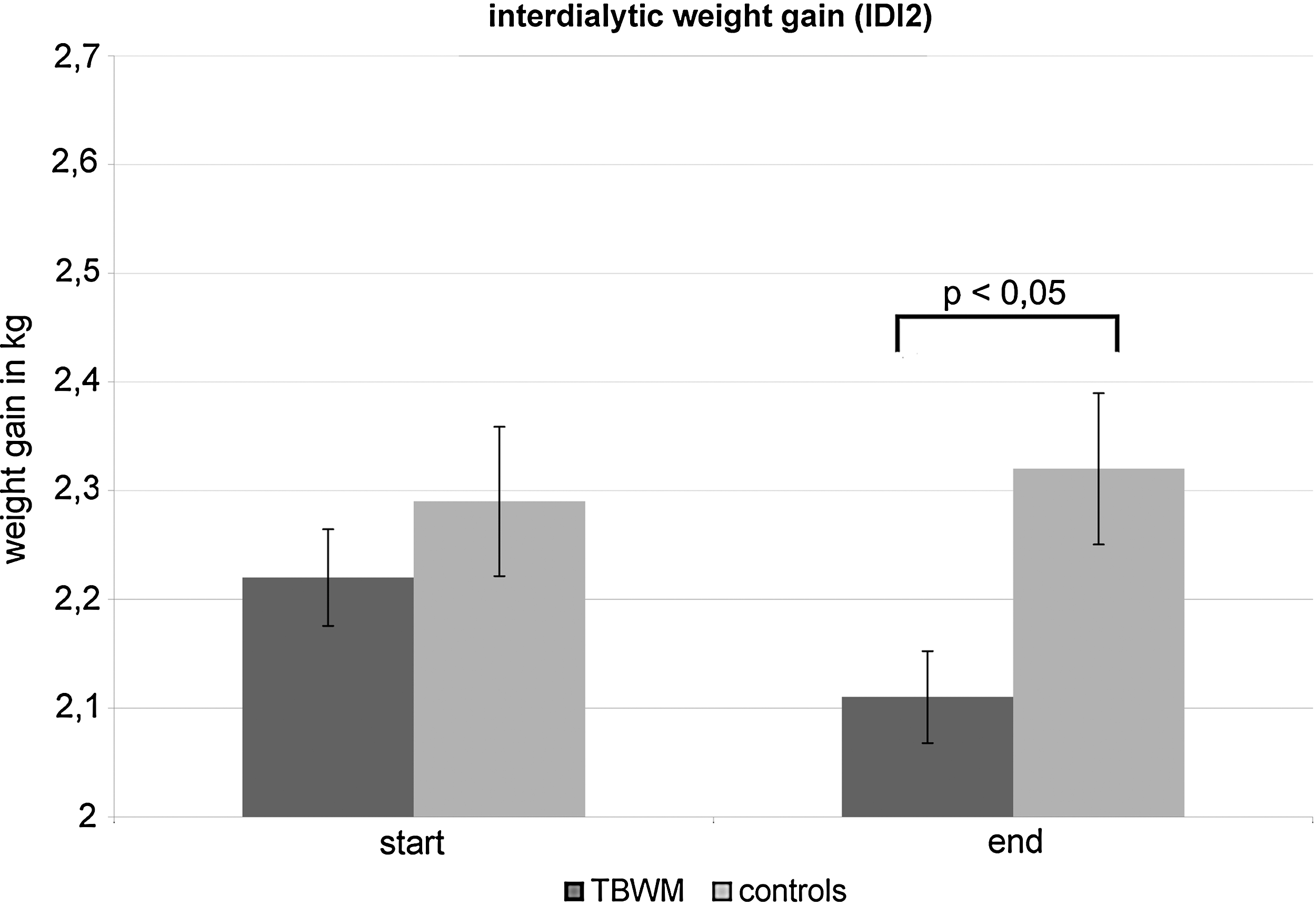
Interdialytic weight gain at the end point (only the second interdialytic interval [IDI2]). TBWM, telemetric body weight measurement.
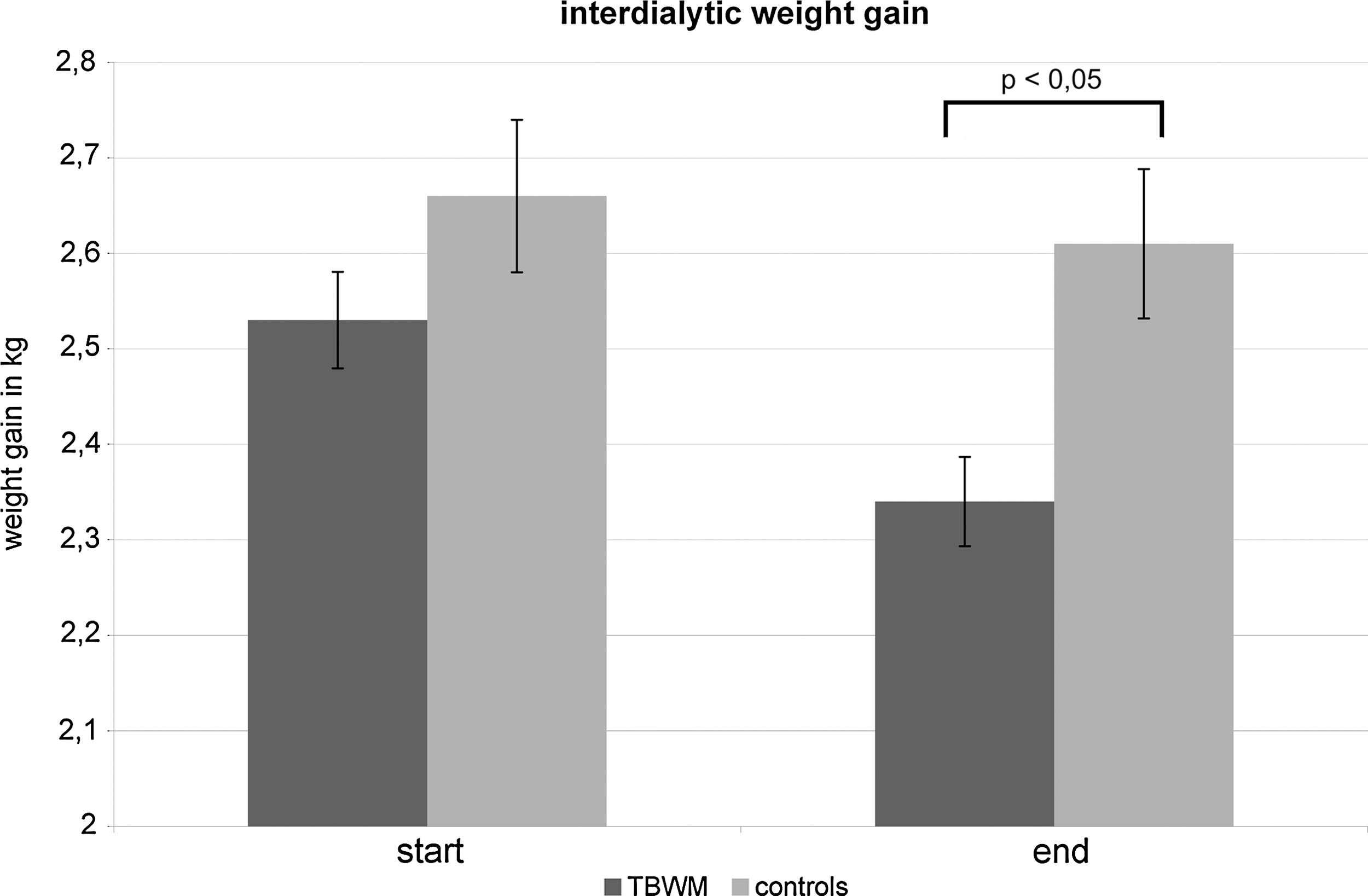
Interdialytic weight gain at the end point (unfiltered). TBWM, telemetric body weight measurement.
Ultrafiltration
At the end of the IDI2 the UFR was reduced from 604.6±148.3 mL/h to 593.7±156.5 mL/h in the TG (p=0.696) and from 623.6±185.8 mL/h to 622.07±196.1 mL/h in the CG (p=0.965). Over the whole week the average UFR was reduced from 631.1±170.6 mL/h to 621.6±169.7 mL/h in the TG (p=0.760) and was increased from 639.2±195.5 mL/h to 652.5±198.6 mL/h in the CG (p=0.712). The mean difference between the TG and CG values for the IDI2 was 19.0 mL/h (p=0.282) before the start of the study and 28.4 mL/h (p=0.122) at the end of the study. The mean weekly difference was 8.2 mL/h (p=0.409) prior to the study's start and 30.9 mL/h (p=0.004) at the end of the study (Fig. 4).

Ultrafiltration at the end point (unfiltered). TBWM, telemetric body weight measurement.
Mean Time Duration on Dialysis
At baseline the mean time on dialysis was 4.56±0.79 h in the TG and 4.58±0.99 h in the CG (p=0.74). At the end of the study the average time on dialysis was 4.47±0.75 h in the TG and 4.62±0.87 h in the CG (p=0.001) (Fig. 5).

Mean time duration on dialysis. TBWM, telemetric body weight measurement.
Blood Pressure
In the TG there was, compared with the CG, a significant higher diastolic blood pressure and a lower systolic blood pressure by trend. At the end of the study this difference was present at the start and the end of a dialysis session (Table 2).
Blood Pressure
Data are mean±standard deviation values.
p<0.05.
CG, control group; IDI2, second interdialytic interval; TG, telemetry group.
Telemetric Body Weight Data
During the study a reduction of the average daily weight gain from 831±323 g/day in the first week to 707±339 g/day in the last week of the study (p=0.098) in a persistent manner (Fig. 6) could be observed in the TG. The median weight gain was reduced from 814 g/day to 727 g/day.
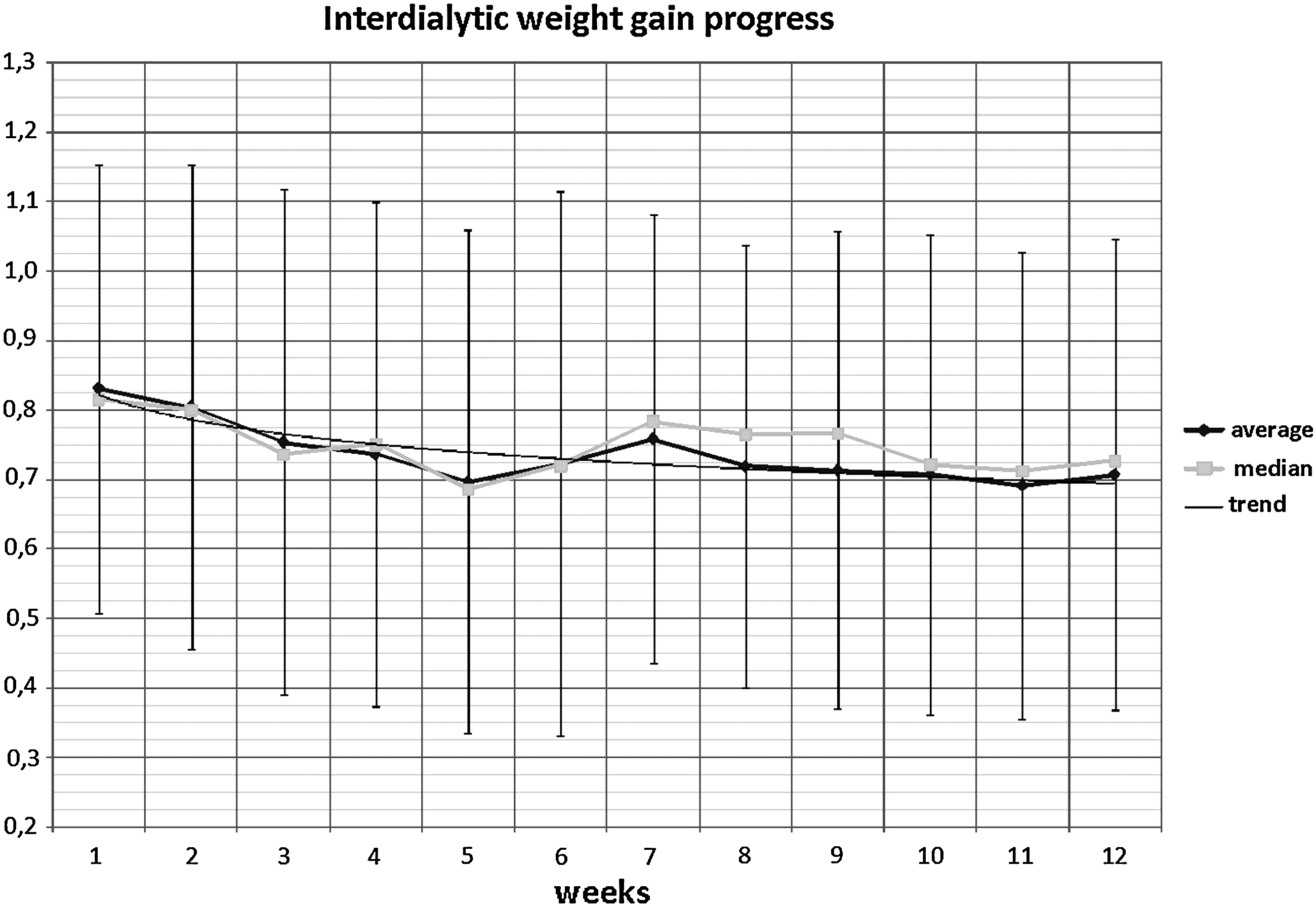
Interdialytic weight gain progression seen in telemetrically transmitted data.
Discussion
The current study demonstrated that a reduction of the IWG can be achieved by telemetric monitoring of the body weight. This is important especially with regard to the correlation of a high IWG and an increased mortality. 5,6
At the end of the study TG patients were dialyzed with a significantly lower UFR compared with CG patients.
To summarize, initially there was no significant difference in both groups regarding all analyzed parameters. The intergroup statistics did not show any significant change over the study period, but parameters directly dependent on fluid intake such as IWG, ultrafiltration, and duration of dialysis were persistently modified in the opposite direction within both groups over the whole investigation time, resulting in significant differences at the end of the study between the two groups. This is consistent with the normal course of patients on hemodialysis, which means that these patients sustain a reduction of diuresis because of their kidney disease. Without effectively restricting fluid intake these changes are connected with a slow but ongoing increase of IWG.
The failing statistical significance within the TG in spite of the obvious trend may be explained by a naturally occurring large individual variance of IWG in patients on hemodialysis. For example, IWG is of less clinical relevance for a patient weighing 90 kg than for one weighing 60 kg. Furthermore, even the same patient may exhibit a large variance in IWG between 1 and 5 kg. Using TBWM, a lower UFR and a significant reduction of mean time duration on dialysis are achieved because an increased uptake of liquid intake can be avoided. The above-mentioned consideration is relevant in the context of a high UFR leading to increased mortality 7,8 and playing an important role in pathophysiology of hypotensive crises during dialyses. 16 Furthermore, high UFR accounts for a poorly adjustable blood pressure because of a reactive release of aldosterone. 29
Hemodynamics during dialysis were not the primary focus of this study considering that blood pressure during hemodialysis provides only small prognostic value for these patients and depends on many different factors such as calcium and sodium concentration, left ventricular function, and antihypertensive medication. Thus, using TBWM a significantly higher diastolic and by trend a lower systolic blood pressure are achieved. Low diastolic blood pressure rates result in increased mortality in dialysis patients 30,31 so that an increase in this parameter might reflect a positive effect. 20,32 The decrease of the systolic blood pressure is desirable in the context of hypertension and cardiovascular diseases, 33,34 resulting in decreased mortality. 35 Moreover, a decrease of the pulse pressure during dialysis was achieved in the experimental group. A direct association between a high pulse pressure and a higher cardiovascular risk was found in multiple studies. 36 –38 Furthermore, it has a better correlation to end-organ damage and cardiovascular diseases than brachial blood pressure office readings. 39 –42 A direct relation between mortality rate and pulse pressure has been reported: an increase in pulse pressure of 10 mm Hg is associated with a 12% increase in mortality. 43 In summary, all blood pressure results based on blood pressure measurement during dialysis have to be judged with caution.
We believe that combination of TBWM with 24-h pulse wave analysis (PWA) via upper arm cuff of a special ABPM device, e.g., PWA monitor Mobil-O-Graph (IEM Ltd., Stolberg, Germany), 44 allows direct recording of the influence of a reduced IWG gain on augmentation index, cardiac output, and notably the 24-h blood pressure characteristics. 45 In particular, the effects of a reduced IWG on blood pressure should be examined via 24-h or 48-h blood pressure measurement in order to obtain a more exact evaluation of blood pressure characteristics 46 and to interpret possible differences in the survival rate. 47
Combined with regular medical and custodial care, TBWM is a feasible method to optimize the IWG and to reducte UFR at dialysis. Interventions by phone and instruction during dialyses can be planned easily. The individual weight-dependent liquid intake adjustment considers varying external parameters such as temperature and air humidity and physical exercise, as well as special metabolism situations (e.g., diarrhea).
Moreover, by reduction of the weight variability using the telemetry technique, a significant influence on blood pressure characteristics is achieved. To evaluate possible positive effects on undesirable events like blood pressure crises, vascular events, hospitalization rates, and mortality rate, a larger organized study with the cooperation of several locations during a longer time of evaluation appears advisable.
Footnotes
Acknowledgments
The study was supported by Roche Pharma Deutschland GmbH.
Disclosure Statement
H.H. has received honoraria from Daiichi-Sankyo, Sanofi-Aventis, Amgen, Roche, Recordati, Takeda, Astra-Zeneca, Berlin-Chemie, and Novartis. J.M. has received honoraria from Daiichi-Sankyo, Novartis, and Berlin Chemie. E.G.S. has received honoraria from Daiichi-Sankyo, Sanofi-Aventis, Amgen, Roche, Böhringer Ingelheim, Takeda, Berlin-Chemie, Astra-Zeneca, and Novartis. C.L.N., F.W., C.B., S.S.-W., E.M.R., V.S., G.C.H., S.M., and L.Z. declare no competing financial interests exist.