
Abstract
Introduction
Expert systems have been widely used in medical and healthcare practice for various purposes. 1 The first large-scale medical expert system, MYCIN, was developed in 1975. It was an interactive computer program that used the clinical decision criteria of experts to help physicians who request advice regarding selection of appropriate antimicrobial therapy for hospital patients with bacterial infections. 2,3 The medical expert system CASNET/Glaucoma was developed in the early 1980s. It drew on the clinical expertise of a network of glaucoma specialists and was eventually able to help with even complex cases. 4 A system called PUFF, also developed in the early 1980s, interpreted lung function test data and became a working tool in the pulmonary physiology lab of a large hospital. 5
The rapid progress of information and communication technologies has significantly influenced healthcare practice. In particular, “telehomecare,” or the more modern term “home telehealth,” has been defined as the use of information and communication technologies to enable effective delivery and management of health services at a patient's residence. 6 Home telehealth allows patients the dignity of remaining in their own homes for as long as possible and by providing care that is equal to or superior than approaches that rely solely on health providers coming into the home for scheduled visits. 7 In a typical home telehealth scenario, the patient subscribes with a home healthcare service provider. The patient then regularly measures vital signs at home and transmits the data to the service provider, which monitors the patient's status and provides healthcare services accordingly.
In telehealthcare, the use of expert systems to generate automated alerts to patients and clinicians and instructions to patients based on telemonitoring data could increase self-care and improve clinical management. 8 Ulieru and Grabelkovsky 9 presented a Web-based expert system for glaucoma that can convey diagnosis alerts or emergencies to registered users, doctors, or patients, thereby allowing them to take immediate actions. Medina et al. 10 presented an expert system that is able to suggest diagnoses, interventions, and outcomes based on the valuation for the patient and vital signs. Seto et al. 8 developed a rule-based expert system for telemonitoring of heart failure. This mobile phone-based system generated alerts and instructions based on the patient's weight, blood pressure, heart rate, and symptoms.
In addition to vital sign data, important concerns in telehealthcare include the compliance with the measurement prescription, accuracy of vital sign measurements, and the functioning of vital sign meters and home gateways. However, few expert system applications are found in the telehealthcare domain to address these issues. Christensen et al. 11 developed an Internet-based expert system for the control of oral anticoagulation therapy. Weekly measurement and dosing at an international normalized ratio at home using the expert system were shown to be superior to conventional computer-assisted monitoring and treatment in an anticoagulation clinic.
This article presents an expert system application for one of the largest commercialized telehealthcare practices in Taiwan by Min-Sheng General Hospital (Taoyuan). Since 2009, Min-Sheng General Hospital has offered a telehealthcare service, “Smart Care,” for patients just discharged from the hospital, patients with chronic diseases, and elderly patients who visit the hospital frequently. Under the concept of creating a “Houspital” (house+hospital), Smart Care strives to achieve the goal of “Patients in their own houses receive the same continuous care as they would in a hospital.”
Figure 1 shows the telehealthcare service platform of Smart Care. Patients discharged from the hospital can join the service on the recommendation of their doctors. Patients regularly measure vital signs at home according to the measurement prescription issued by their doctors. They then upload the measurement data and report their health status through a home gateway or the Web interface using a home computer or smartphone. The patients can also phone the call center for health education and counseling, dispensed by the interactive voice response system.
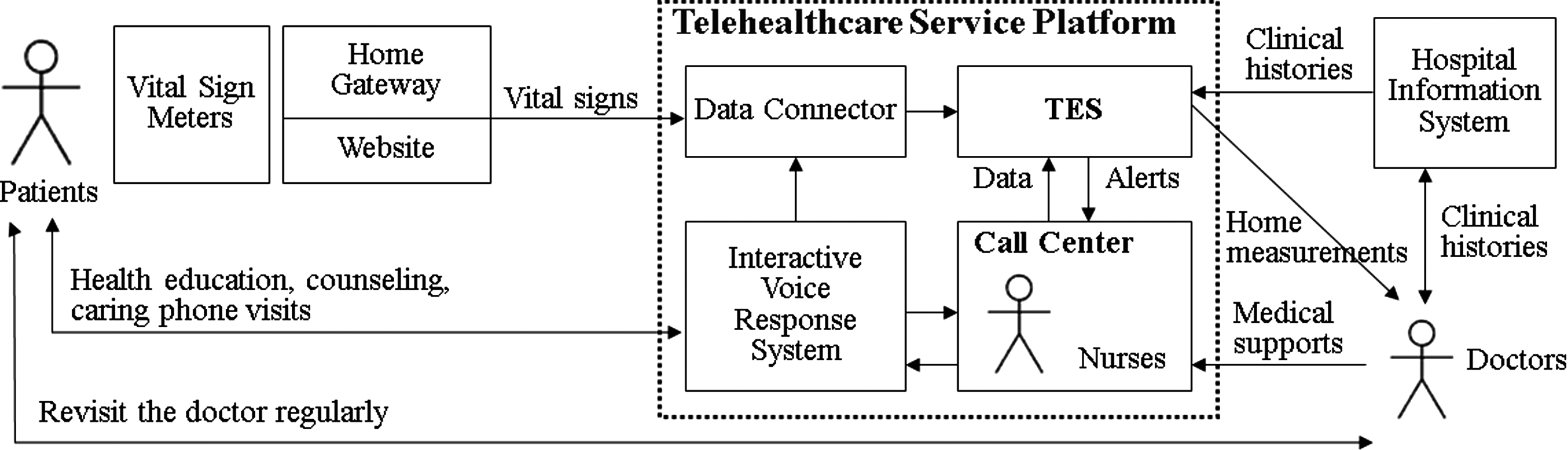
The telehealthcare service platform of Smart Care. TES, Telehealthcare Expert System.
The main function of Telehealthcare Expert System (TES), developed in this research, is to detect and classify events based on the measurement data transmitted to the database at the call center, including abnormality of vital signs, violation of vital sign measurement prescriptions, and malfunction of hardware devices (home gateway and vital sign meter). These last two capabilities are critical in the telehealthcare domain because the call center otherwise might not know that it lacks the current health situation of the patient. When an abnormal event is detected, TES assigns an urgent degree and alerts the call center, whose staff can immediately phone the patients for counseling or to urge them to return to the hospital for further tests. The staff members inform the doctors when they cannot handle the situation. Doctors provide consulting to the call center. In the mean time, the doctors can refer to the long-term monitoring data and events in the database of the call center, as well as the clinical history in the hospital information system in the outpatient and inpatient service.
In “Smart Care” telehealthcare service, TES plays a key role in the whole infrastructure: 1. It is highly integrated with telehealthcare processes. The expert system must be highly integrated with the telehealthcare information platform and processes to operate smoothly, minimize the time expended by call center personnel, and ensure data integrity and accuracy. 2. It helps accumulate knowledge about telehealthcare, improve its accuracy, and reduce human effort. The expert system is expected to integrate with the knowledge base and carry out self-improvement by updating models and mechanisms to accumulate knowledge from doctors, medical experts, nursing experts, and clinical experience. It is also expected to improve accuracy and reduce human effort, cost, and mistakes. 3. It is customized for each individual patient to provide personalized care and improve care quality. The expert system is expected to have mechanisms that adapt to each patient's health condition.
This article is organized as follows. First the events detected by TES are described, followed by how TES provides the personalized care. Then the experiment on the usability of TES's user interface for nurses is outlined, followed by the results of the 2-year practice. Finally, conclusions are drawn from the results, and implications are discussed.
Materials and Methods
Events Detected by TES
Figure 2 depicts the information flow of TES. As do most expert systems, TES contains a knowledge base that is populated by doctors and medical experts through the “developer interface” and by databases of vital signs, prescriptions, and service records. The rules in TES's knowledge base were framed by doctors and medical experts involved in this project according to their experience in telehealthcare. Some rules were created according to international guidelines (e.g., American Heart Association guidelines for hypertension). Forty-two default rules created for TES were examined and approved by a professional committee in the hospital before being stored in TES's knowledge base. Interference engines interpret logic rules from knowledge base and reference the measurement data from databases. If the TES detect an abnormal event, it will output alert messages with urgent degrees to nurses via the “user interface.”

The information flow of the Telehealthcare Expert System.
The abilities of the TES to detect abnormality of vital signs, violation of vital sign measurement prescriptions, and malfunction of hardware devices are described below.
Abnormality of vital signs
Vital signs reflect the interaction of many physiological systems and are used as an outcome measure to assess efficacy of intervention in telehealthcare applications. TES accepts several types of vital signs that are frequently used in the telehealthcare domain, such as systolic blood pressure, diastolic blood pressure, mean arterial pressure, heart rate, blood glucose, and body temperature. These vital signs can be measured at home using commonly available equipment and uploaded via automatic home gateways. TES also accepts vital signs that are measured in the hospital and long-term care, such as respiration rate, respiration volume, and oxyhemoglobin saturation by pulse oximetry. Other health status indicators, such as pain, swollen, and wound liquid, apply to patients recovering from surgery. These indicators were mostly input by nurses interactively during the phone conversation with the patients, although the patients can also choose to input from a Web site or smartphone app.
Table 1 shows a few sample rules, including rules for single events (e.g., “blood pressure is extremely high”) and rules for long-term events (e.g., “mean arterial pressure is higher than the average of the most recent 30 days”).
Sample Logic Rules for Abnormal Vital Signs
BG, blood glucose (in mg/dL); BT, body temperature; DBP, diastolic blood pressure (in mm Hg); HR, heart rate (in beats/min); LQ, wound liquid; MAP, mean arterial pressure; PN, pain; SBP, systolic blood pressure (in mm Hg); SW, swollen.
The urgent degree indicates the severity of the event. There are 9 degrees, with 1 being the lowest and 9 the highest. The group data field classifies patients according to overall health status and helps identify the logic rules that might apply to a given patient. The number of occurrences determines the threshold for sending a predefined alert message to the call center.
These event rules, urgent degrees, number of occurrences before sending an alert, and the alert messages are decided by the doctor experts according to their experience and knowledge in telehealthcare.
Violation of vital sign measurement prescriptions
Compliance describes the degree to which a patient correctly follows medical advice. The compliance of patients to vital sign measurement prescriptions is crucial to the success of telehealthcare practice. TES detects violations of five types of vital sign measurement prescriptions (Table 2): • Obtain one measurement every n h • Obtain n measurements in a day • Obtain one measurement every n days • Obtain measurements at “specific times” of day • Obtain measurements on “specific days” of the week
Types of Logic Rules for the Violation of Measurement Prescriptions
The measurement prescriptions given to a patient by his or her doctor are also input into the knowledge base by selecting among the five types of logic rules and filling in the required parameters. Table 3 gives a few sample rules. The call center is alerted if a patient has fewer measurements than required by the prescription. If a patient has more vital sign measurements than required by the prescription, it may indicate that the patient is anxious, and the call center is therefore alerted.
Sample Logic Rules for the Violation of Measurement Prescriptions
Malfunction of devices
Reliability has been an important issue in home telehealthcare applications, especially with the increasing variety of telehealthcare devices. Many home gateways report to a central server at regular intervals (e.g., every hour). TES generates an alert of gateway failure (device failure, power failure, Internet connection failure, transmission problem, or data cache problem) if a report is not received by 6 h after the prescribed time. Some home gateways have self-diagnosis functions and send the error codes to the central server when a malfunction occurs. TES also interprets these error codes and generates corresponding alerts to the call center.
TES also detects malfunction of the vital sign meter from the data received. Typical data are shown in Table 4. The data usually consist of 12 items: meter ID, meter brand, meter model, firmware version, measurement time, vital sign type, vital sign value, vital sign unit, special notes, sync flag, sync time, and checksum. Three types of malfunctions can be detected from the measurement data: error in the meter clock, data value out of range, and data value zero or null. The accuracy of the vital sign meter is not measurable by TES.
Typical Vital Sign Data Sent by a Vital Sign Meter
BG, blood glucose; bpm, beats per minute; DBP, diastolic blood pressure; HR, heart rate; SBP, systolic blood pressure.
The correct meter clock time is important in telehealthcare applications for recording health status of the patient. An error in the meter clock may occur when the meter battery has exhausted, the user changes the battery without correctly resetting the date and time, or the time circuits in the meter have malfunctioned.
Every datum provided by a vital sign meter would normally be nonzero and adhere to a specified range. Table 5 shows examples of such ranges. An out-of-range datum may be caused by meter malfunction or the patient being in critical condition.
Typical Examples of Result Ranges for a Vital Sign Meter
BG, blood glucose; BP, blood pressure; bpm, beats per minute; HR, heart rate.
Figure 3 illustrates how the subranges of a vital sign datum may indicate various abnormalities, using blood glucose measurement values as an example. Each problematic subrange would be covered by one or more logic rules. Table 6 shows several sample rules for malfunction of devices, including gateway failure (Rules 1 and 2), error in the meter clock (Rule 3), data value out of range (Rules 4 and 6), and data value zero or null (Rule 7).
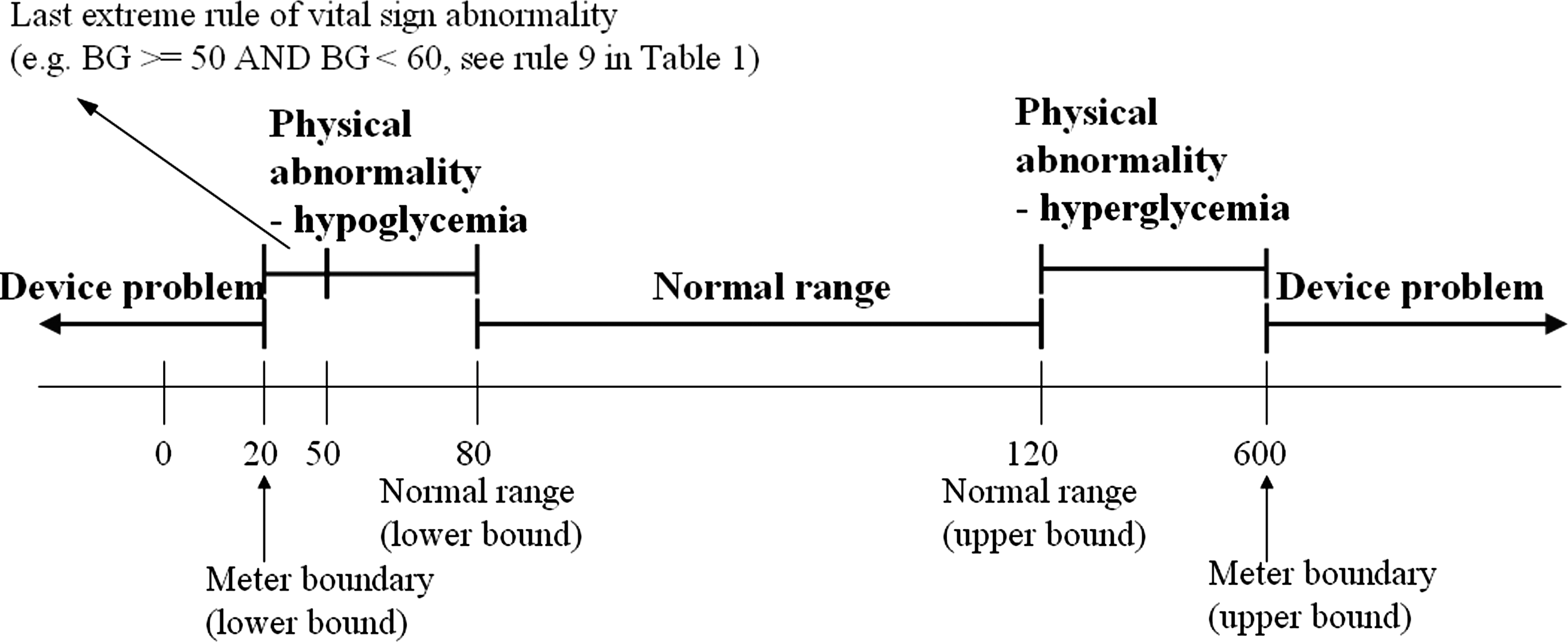
Sample subranges for blood glucose (BG) vital sign.
Sample Logic Rules for Malfunction of Devices
BG, blood glucose; GW, home gateway; HRS, hours.
In a typical home telehealth scenario, patients' measurements are taken by patients themselves or their caregivers. In this study, efforts are made to ensure the fidelity of the home measurements. Before discharge from the hospital, patients and caregivers receive a short training session on how to correctly make the measurement. Patients and caregivers are requested to bring their measurement devices when they revisit the hospital for calibration and retraining.
This communication is not a systematic comparison of home measurements and hospital measurements. However, the doctors read both home measurements and hospital measurements and interacted with the patients when they revisited the hospital. Erroneous measurement can also be detected by TES. For example, in blood glucose measurement, improper operation of measurement may cause an abnormally low value of a vital sign datum (Rule 5).
Personalized Care
Customization is especially important in the telehealthcare practice. TES allows customization of event rules for each individual patient to provide the personalized care.
TES has distinct “default rules” for the common group, disease groups, and specific groups, for a total of 42 default event rules of these three groups. Each patient is assigned a set of default rules when he or she joins the service. After the patient is examined and evaluated by his or her doctor, the doctor may customize the rules' vital sign boundaries, urgent degrees, and alert messages. A warning message will be displayed by TES to confirm with the doctor if a new customized boundary overlaps with those of existing rules. The doctor can update these rules at any patient visit.
All events detected by TES are assigned an urgent degree and an alert message, and both of these are displayed to the nurse at the call center. TES will also retrieve any relevant events from the service history database and display them.
A call center that provides Smart Care telehealthcare service will respond to TES alerts by taking the actions listed below.
Abnormality of vital sign or violation of measurement prescriptions
• Advise the patient or a family member to address the situation by obtaining health education and counseling by either phone or short message service.
• Arrange a visit with the doctor (if the patient's health status is not critical) or the emergency medical service (if it is critical).
• Continuously monitor similar events for that patient and adjust the treatment plan as conditions change.
Malfunction of devices
• Ascertain whether the patient can care for him- or herself in the event of a device failure.
• Inform the patient as to what constitutes failure or malfunction of a telehealthcare device and explain what steps to take if a device stops working properly.
• Designate a representative to assist the patient to get the device fixed or replaced if it should malfunction.
• Continuously monitor the ability of the patient to participate in telehealthcare activities and adjust the treatment plan as conditions change.
Experiment to Determine Effect of TES on Nurses
In order to know the time saved in the call center with the help of TES, an experiment was conducted involving senior nurses in the call center.
This experiment identified any difference in the time required to judge events manually versus with the help of TES. The time for judging the event of abnormality of vital signs was calculated from when a vital sign measurement is received. The time for judging the event of violation of measurement prescription was calculated from looking up the measurement prescription of the patient. The time for judging the event of malfunction of hardware devices was based on a vital sign measurement being received and the nurse looking up the report records or error codes for telehealthcare devices.
In the first round, two groups of nurses judged three types of events without TES. They judged the events by manual reference of the vital sign measurements uploaded from the patient, the patient's history data (including service records), measurement prescriptions from the telehealthcare information platform and the Hospital Information System, and the report records or error codes from telehealthcare devices. In the second round, the same two groups of nurses judged three types of events using TES without manually referencing any other records. In each round, each nurse judged 30 events: 10 each of vital sign abnormality, violation of measurement prescription, and malfunction of device. This experiment took place when TES was first installed in October 2009, to prevent the effect of familiarization of nurses' judging events.
Results
In the 2 years of clinical practice of Smart Care telehealthcare service from August 2009 to September 2011, 19,182 patients were served. Patients were assigned an average of 34.6 rules for abnormality of vital signs, for a total of 663,304 rule assignments. There were 23,455 measurement prescriptions given by doctors. In total, 158,122 vital sign measurements were received by TES, of which 37.5% were of blood pressure, 18.0% were of heart rate, 4.9% were of blood glucose, 9.1% were of body temperature, and 30.5% were of health status (pain, swollen, and wound liquid).
TES detected 41,755 events in this period, of which 22.9% concerned abnormality of vital signs, 75.2% concerned violation of measurement prescription, and 1.9% concerned device malfunction. Most of the events were violations of measurement prescription. This indicates that compliance of measurement could be improved substantially. After the call center phoned the patients involved, 74.8% of them improved in compliance of measurement. On average for a given day, 1,274 patients participated in this telehealthcare. The average day saw 14.4 events of vital sign abnormality, 47.3 events of violation of measurement prescription, and 1.2 events of device malfunction.
As shown in Table 7, urgent degree 5 accounted for a higher percentage (37.5%) than did any other event indicating vital sign abnormality urgent degree. Table 8 shows that urgent degree 1 accounted for a higher percentage (41.7%) than did any other event indicating violation of measurement prescription urgent degree. In the events involving violation of measurement prescription, 99.2% of events indicated that the number of measurements was lower than required by the prescription, and 0.8% of events indicated that the number of measurements was higher than required by the prescription.
Urgent Degrees of Events Involving Vital Sign Abnormality
Urgent Degrees of Events Involving Violation of Measurement
For the experiment involving two groups of senior nurses in the call center, Table 9 shows the results. On average, the nurse in the call center judging events manually required 50.0 s for vital sign abnormality, 51.5 s for violation of measurement prescription, and 43.0 s for malfunction of device. On average, the nurse in the call center judging events with the help of TES required 12.5 s for vital sign abnormality, 10.5 s for violation of measurement prescription, and 11.0 s for malfunction of device. Therefore, TES saved 37.5 s (75.0%) for vital sign abnormality, 41.0 s (79.6%) for violation of measurement prescription, and 32.0 s (74.4%) for malfunction of device. This experiment indicated that TES reduced by 76.5% the time required for call center personnel to judge events.
Experimental Result with Two Groups of Senior Nurses
TES, Telehealthcare Expert System.
This large reduction can be attributed to the elimination of manual data lookup, manually operating the information systems, manually comparing the vital sign measurements and other data, and judging the events using the human brain. With the help of TES, the nurse in the call center only needs to receive the event detected by TES and read the alert message with urgent degree and additional information, without looking up any data or other manual processing that may introduce errors. They can easily address the event and phone the patient.
Conclusions and Discussion
This article presents an expert system application for one of the largest commercialized telehealthcare practices in Taiwan by Min-Sheng General Hospital. The main function of TES is to detect and classify events based on the measurement data transmitted to the database at the call center, including abnormality of vital signs, violation of vital sign measurement prescriptions, and malfunction of hardware devices (home gateway and vital sign meter). These last two capabilities are critical but not commonly found in expert applications in the telehealthcare domain.
During 2 years of clinical practice from 2009 to 2011, 19,182 patients were served by TES. TES detected 41,755 events, of which 22.9% indicated abnormality of vital signs, 75.2% indicated violation of measurement prescription, and 1.9% indicated malfunction of devices. On average, the expert system reduced by 76.5% the time that the nursing team in the call center spent in handling the events.
Although the expert system helped to reduce the cost and improve the quality of the telehealthcare service, a survey of 1,167 patients conducted in August 2011 revealed that only 1.6% thought that measuring and transmitting vital signs is helpful, in contrast to the 88.1% who judged phone visits and counseling to be helpful.
For patients just discharged from the hospital, the telehealth service is free for the first month. The cost is covered by the hospital from the savings in the 8.3% reduction in days of re-hospitalization after providing the telehealth service over the 2 years. The patients have to pay a monthly fee of NTD 600 (about $20) if they wish to continue subscribing to the service in the second month. Even though 91.1% were satisfied with the Smart Care service, 96.0% did not want to pay for a long-term subscription.
All citizens in Taiwan are covered by the National Health Insurance, started in 1995. Under the National Health Insurance, a patient pays NTD 150 (about $5) when visiting a doctor in the clinic. In our questionnaire, most people (76.3%) replied that they would rather see a doctor than pay NTD 600 per month to use the telehealthcare service, and 45.1% of the patients did not want to continue the service for the second month because they felt they had already recovered; 21.1% of the patients simply replied that they did not think they should pay an extra fee for telehealth service.
Footnotes
Acknowledgments
This research is sponsored by the Department of Industrial Technology, Ministry of Economic Affairs, Taiwan; the National Science Council, Taiwan; and the Ministry of Education, Taiwan. This research is also supported by Smart Care Inc., Taiwan. These supports are gratefully acknowledged.
Disclosure Statement
M.-S.H. and C.-M.C. are employees of Smart Care Inc. H.L. and Y.-L.H. declare no competing financial interests exist. The funding source did not influence study design, data collection, data analysis, interpretation, or presentation.