
Abstract
Introduction
A randomized controlled study by Berman et al. 1 is part of a growing body of research on the use of home telehealth in promoting illness self-management. 2 –5 This study demonstrated improved health outcomes and cost-effectiveness over a 21-month period. In addition, results from that study showed that the number of nurse–patient contacts for medical outliers decreased significantly over time.
In the present study, we examined the longer-term effects (42 months) of nurse oversight on home telehealth monitoring in a larger population of high-risk dialysis patients. We conducted an economic analysis based on the number of hospital and emergency room (ER) visits, the number of hospital days, and the total charges for in-patient and ER services for all patients, including comparison with a control group. The purpose of this study was to determine if the improved outcomes and economic advantages found in the pilot study were reproducible in a larger sample followed for a longer time period.
Subjects and Methods
Sample
This study was approved by the Western Institutional Review Board. Patients in this study had a diagnosis of end-stage renal disease and had been undergoing outpatient dialysis three times per week for at least 3 months. They did not require additional services such as home healthcare or hospice. The sample size for the analysis was 99; 43 patients were enrolled in the intervention group (remote technology [RT]), and 56 patients received the usual optimum dialysis care (usual care [UC]). The sample size does not reflect 1 patient who was withdrawn from the study (RT group) after the observation of multiple ER visits seeking narcotics.
Measures
Healthcare resource outcomes
Data collected included the number of hospitalizations and ER visits, number of days in the hospital, and total charges for inpatient and emergency room services for all patients (n=99). All utilization variables are cumulative over an approximately 1,260-day period, although the number of days in the trial varied for each patient.
Remote care nurse–patient contact
Patients in the RT group were asked to submit their physiologic measurements (i.e., blood pressure, pulse, weight, oxygen saturation, and blood sugar) per a physician's plan of care as well as answer 10 health questions on their nondialysis days. The frequency and nature of remote care nurse–patient contacts were recorded and distinguished by medical and technical occurrences. Medical issues concerned physiologic outliers or subjective changes in clinical conditions of patients prompting contact by the remote care nurse. Technical issues usually occurred as a result of equipment malfunction, problems with Internet connectivity, or difficulty mastering the technology, also prompting contact by the remote care nurse. A scatterplot chart with linear trend lines, which included data from all 43 patients who were enrolled in the RT group, was generated to illustrate the number of medical and technical occurrences at 30-day intervals.
Results
Health Resource Outcomes
Data from 99 patients were included in this analysis. There is an inverse proportion of females to males between the RT (18/25) and UC (30/26) groups and a slightly higher mean age in the UC group compared with the RT group (63.1 years versus 58.6 years); however, all patients were clinically similar based on their qualifying risk scores. 1 The number of study days per patient ranged from 120 to 1,264 (mean, 572.2) for those in the RT group and 72 to 1,231 (mean, 565.7) for those in the UC group. The number of hospitalizations and hospital days are significantly lower in the RT group than in the UC group. The differences in hospital and ER costs and hospital and ER costs per study day were also significantly lower for the RT group than the UC group, as shown in Table 1.
Healthcare Resource Outcomes
Data are mean (standard deviation) values unless stated otherwise.
p<0.05 was defined as a significant difference.
ER, emergency room.
Nurse Clinician–Patient Contact
The frequency of medical outliers and technical problems improved over the 42-month period of telemonitoring (Fig. 1). During the first month of the intervention, the number of nurse-initiated telephone contacts required for medical issues totaled 82 (1.9 per patient), and there were 88 (2.0 per patient) for technical issues. At the end of the data collection period, the frequency of nurse-initiated contacts decreased to zero.
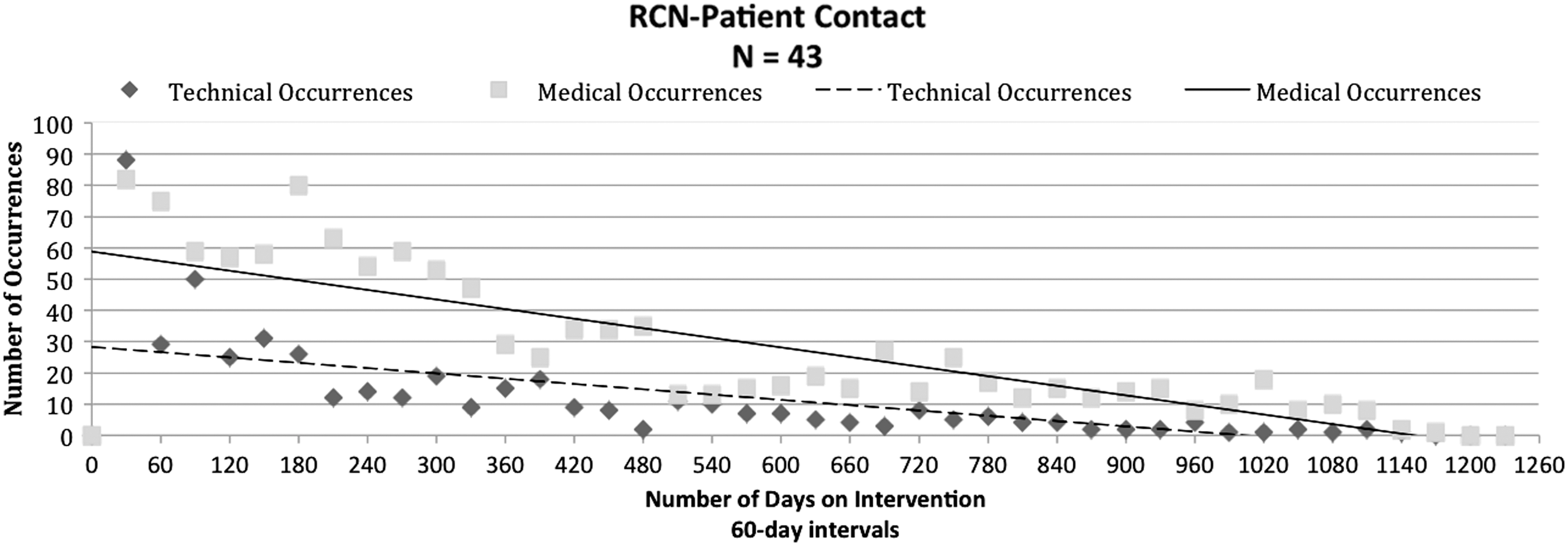
Remote care nurse (RCN)–patient contacts.
Discussion
The results of this study support our earlier findings that home telehealth with nurse oversight can improve health outcomes and reduce the cost of hospitalizations and ER visits in high-risk dialysis patients. The costs associated with hospitalizations and ER visits were again significantly lower in the intervention group compared with the control group. Our data also show that, over time, the number of medical and technical occurrences dramatically decreased and therefore required fewer nurse contacts. The significance of our findings makes a strong argument for home telehealth with nurse oversight to improve health outcomes by preventing hospitalizations in select patients with chronic illnesses.
In our pilot study, 1 we suggested that the reduction in medical occurrences over time was related to patients taking more ownership of their health with support from the remote care nurse. The pattern of decreasing frequency of telephone contacts by the nurse clinician prompted by outlier data was confirmed in the continuation of our pilot study.
The study population was derived from an outpatient dialysis program; despite their state of poor health, they lived at home, commuted to the dialysis center, and had home support or caregiver assistance. Furthermore, those diagnosed with cancer or AIDS were excluded. This suggests a level of vigor enabling patients to make health behavior changes. Further study is warranted to investigate the viability of such a program in other patient populations and to better define the element of predicting success.
Footnotes
Acknowledgments
This research was supported by the U.S. Department of Defense's U.S. Army Medical Research and Materiel Command Telemedicine and Advanced Technology Research Center under award number W81XWH-07-2-0064. The U.S. Army Medical Research Acquisition Activity (Fort Detrick, MD) is the awarding and administering acquisition office. Other sources of support include the Hawaii Medical Service Association and the Queen's Medical Center, Honolulu, Hawaii. We appreciate the efforts of Tamami Harada in the preparation of Table 1 and ![]() .
.
Disclosure Statement
No competing financial interests exist.