
Abstract
Introduction
In the last 30 years, we have assisted in the increase of production and marketing of health technologies, which have significantly contributed to the growth in healthcare costs, 1 which are not always associated with a real increase in patients' benefits. 2 Therefore, we can be confident with using the new methodological guidelines of technology assessment, which is no longer based on technology-oriented paradigms, typical of the 1970s and exclusively focused on the direct use of technology (Is it accurate? Is it safe? Does it work?), but on problem-oriented paradigms, more aware of clinical, social, economic, epidemiological, scientific, and ethical aspects.
In this case, the technological innovation analyzed is the development of a telematic structure, the TOCOMAT system for telecardiotocography, for the specialized management of pregnancy. This system provides prognostic parameters for pregnancy thanks to the connection between Level III specialized units and the peripheral area in which the woman lives, so that healthcare needs are satisfied without the expensive and inappropriate hospital setting.
The aim of this study was to determine whether the cardiotocography (CTG) technology with the TOCOMAT system can improve the hospitalization data by reducing the number of potentially preventable or inappropriate hospitalizations.
If diagnostic-related group (DRG) 384 (other antepartum diagnoses without medical complications) collects almost all the contacts with obstetric emergency departments, because of the lack of assessment of the risk by CTG outside the hospital, an estimate of the appropriate use of hospitalization for the prepartum period can be obtained by measuring as its indicator the average hospital stay for DRG 384.
In particular, the hypothesis of the study is that the reduction of improper hospitalization leads to an economic and management cost saving, in comparison with investment and TOCOMAT system management costs.
The objective of the analysis conducted at the Department of Obstetrics, Gynecology, Urological Science and Reproductive Medicine of the “Federico II” University Hospital of Naples, Italy, was the following: to analyze the length of the hospital stay at the Department of Prenatal Medicine in terms of number of hospital stay days saved, dividing patients into “pregnant women under CTG monitoring” and “pregnant women not subject to CTG monitoring.”
Materials and Methods
Appropriateness Of Pregnancy And Delivery Setting
According to current Italian Ministry of Health statistics, in 2010 pregnancy and delivery (727,489 hospital admissions) were the third major diagnostic category for incidence of hospitalization (9.9% of total), with 2,806,375 hospital stay days (average, 3.9 hospital stay days), 9.9% of which were same-day discharges and with 546,077 hospital stay days exceeding the threshold (6.8% of hospital admissions). Of the admissions, 169,042 were day-hospital (5.6% of major diagnostic category) with 240,907 admissions (average of admissions, 1.4). Of day-hospital admissions, 71.8% were the only admission. Birth assistance (232,632 discharges) was the most frequent hospital procedure performed, with “cesarean section” (212,671 discharges) in third place.
Hospitalization for pregnancy and postpartum complications is usually excluded from analysis of appropriateness. However, an estimate of improper use of hospital admissions can be made from the short (emergency or elective) prepartum admissions that ended without complications and without the need of delivery. They are often performed for maternal concern or by the doctor's request, perhaps for the lack of a risk assessment through TG.
DRG 384 (other antepartum diagnoses without medical complications) is the most frequent discharge DRG for such cases. In particular, it offers a consideration of the following characteristics of hospital stay at the national and local levels (Table 1).
Rate of Discharges, Average Hospital Stay, and the 0–1 Days Percentage of Diagnostic-Related Group 384 Cases in Italy and at the “Federico II” University Hospital in Naples in 2010
The “Federico II” University Hospital Of Naples Tocomat System
The computerized telecardiotocography (TOCOMAT) project was designed and developed by the Department of Obstetrics, Gynecology, Urological Science and Reproductive Medicine of the “Federico II” University Hospital of Naples in 1998 with the aim of detecting the early fetal hypoxic state and thus leading the obstetrician to a rapid delivery, preventing severe hypoxia and fetal compromise, 3 avoiding the subjective interpretations typical of the conventional system and any unclear fetal heart rate signals, often found with the Sonicaid System, both used throughout Italy.
The development of the network of Level I regional centers, served remotely by the reporting system of the Department of Obstetrics, Gynecology, Urological Science and Reproductive Medicine of the “Federico II” University Hospital of Naples, has allowed high-risk pregnant women needing intensive monitoring to have the CTG trace performed “near home,” reducing the frequent and often unnecessary travel to Level III facilities, often due to the lack of medical personnel able to analyze the CTG traces.
From the start date, the number of centers and pregnant women enrolled increased gradually with a progressive increase in CTG traces performed (Fig. 1), with a significant increase between 2006 and 2011.
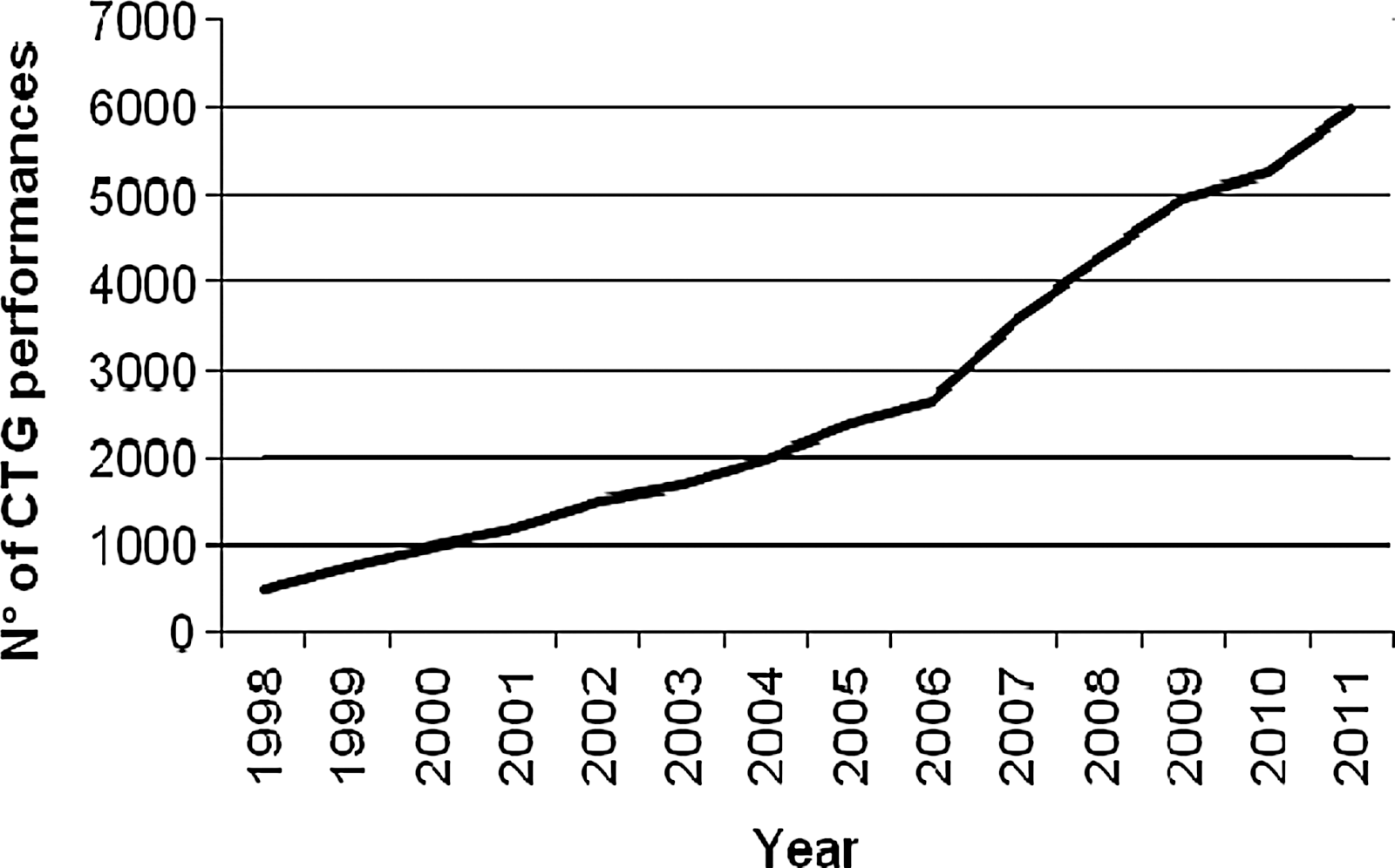
Trend from 1998 to 2011 for cardiotocography (CTG) performances provided at the Department of Obstetrics, Gynecology, Urological Science and Reproductive Medicine of the “Federico II” University Hospital of Naples, Naples, Italy.
The TOCOMAT network is based on the principle that the CTG traces are made at Level I centers and sent (via a SIM card connected to a public telephone line with a transmission speed of 40–60 s) to the operations center at the Department of Obstetrics, Gynecology, Urological Science and Reproductive Medicine of the “Federico II” University Hospital of Naples, which analyzes and electronically processes the traces and finally transmits the processed trace back to the initiating Level I center. The electronic processing of the trace avoids any “subjective” interpretation, which requires adequate skills by the gynecologist, without which inaccurate interpretations could be derived.
The Level I centers involved include eight remote units located at clinics and hospitals in the Campania region, which do not have medical staff with appropriate skills for the analysis of CTG traces. The remote units are located in Ravello, Ischia, Monte di Procida, Mugnano, Castelvolturn, Barra-Ponticelli, Miano, and Salerno. The system has two additional remote units at Semmelweiss University, Budapest, Hungary, and the Instituto Nacional Maternal Perinatal, Lima, Peru, which are connected via the Internet. These latter two remote units are not evaluated in this study because the end points cannot be measured.
Each unit provides a cardiotocograph to record traces and to send them via modem to the operations center, with the personal data of the patient. An update of the prenatal telemedicine network equipment has recently been performed, with the application of wireless technology also to the TOCOMAT system. In fact, using portable and lighter cardiotocographs, with a USB port, traces are transferred to a smartphone that via general packet radio service sends data to the operations center. Within a few minutes, the report of the computerized analysis is sent to the remote unit by e-mail and is displayed again on the mobile phone. In this way, space limitations of the previous version of the TOCOMAT wired system are overcome. 4 –6
General Characteristics Of Ctg Networking And The Tocomat System
CTG is the most widely used technique for the monitoring of fetal well-being. The CTG system is composed of an ultrasound transducer (BCF Technology), to detect the fetal heartbeat, and of a pressure transducer, to detect the uterine contractile activity. The ultrasound transducer is placed on the woman's abdomen, next to the fetal back, as close as possible to the focus of maximum auscultation of the fetal heart. Using the echoes of opening and closing of the heart valves as triggers, it defines the duration of the cardiac cycle. The pressure transducer is located on the uterine fundus, and it detects the tone of the myometrium. As it is an external monitoring, the intensity of the contractions recorded is not real, but because it is noninvasive and not harmful for fetal health, it is used more than the internal systems. Pressing a button connected to the cardiotocograph, the mother can also report the fetal movements she perceived. On the centimetric scale-trace two paths are simultaneously recorded: the fetal heart rate above and the uterine activity below. In Italy and throughout Europe, the scrolling speed of the paper is 1 cm/min. Acoustic and visual alarms are related to the normal range of the parameters and to the quality of the signal (green=good, yellow=good, red=absent). A printer connected to the system will print the trace. Monitoring takes at least 30 min, with the pregnant woman lying on an armchair or on a bed; the left lateral position is better to avoid supine hypotension. The monitoring is normally carried out once a week, starting from week 37 of gestation. The parameters analyzed are fetal heart rate, baseline variability, and fetal acceleration determination contractions. Moreover, the computerized system provides analysis of short-term variability, long-term variability, interval index, change in DeltaMS, approximate entropy, spectral low frequency, spectral medium frequency, and spectral high frequency. The device involves an electronic method, based on ultrasound, used for simultaneous recording of fetal heart and uterine contractions.
According to the 2001 classification of the Royal College of Obstetrics and Gynecology, the prepartum CTG traces can be considered (Table 2): (a) suspected, if there is only one non-reassuring parameter, and (b) pathological, if there are two or more non-reassuring parameters.
Classification of Cardiotocographic Traces
bpm, beats per minute.
If the trace is not suspected or pathological, the woman is re-evaluated according to the timing of pregnancy and the individual risk.
In this case, performing a trace in a local setting near home avoids returning to the hospital and reassures the woman. In the absence of a CTG system near home or in consulting rooms or if it is not considered reliable enough by the pregnant woman, returning to the obstetrics emergency department may be possible.
In such cases, the woman is admitted under ordinary and urgent hospitalization, which will continue until one of the following conditions is realized: (1) normal pregnancy, shown by a series of traces, so that a discharge is allowed; or (2) high-risk pregnancy, shown by a series of traces, so that the hospitalization continues until the resolution of the complications or until the delivery.
In the first case, the discharge may give rise to DRG 384 (other antepartum diagnoses without medical complications). In the second case, one of the following DRGs is possible: • M 383: other antepartum diagnoses with medical complications • C 370: cesarean section with complicating diagnoses or co-morbidities • C 371: cesarean section without complicating diagnoses or co-morbidities • 372 M: vaginal delivery with complicating diagnoses • 373 M: vaginal delivery without complicating diagnoses • 382 M: false labor
Procedures
In order to analyze the length of the hospital stay at the Department of Prenatal Medicine, in terms of number of hospital stay days saved, dividing patients into “pregnant women under CTG monitoring” and “pregnant women not subject to CTG monitoring,” a case-control study analyzing the medical records of patients in the first 4 months of obstetrics of 2009, 2010, and 2011 was performed.
CTG monitoring was offered twice a week from week 37 of gestation so that there were the same numbers of traces in both low- and high-risk patients. A window of 30 min of trace was considered and analyzed for all the patients. The clinic staff was unchanged during the study period and was composed of qualified and experienced doctors and midwives. The computer-assisted equipment (Corometrics 170, General Electric; and Philips HP Series 50A) is updated quarterly by the respective official technicians of Philips and General Electrics.
The study was approved by the Health Department of the “Federico II” University Hospital.
Results
The control group consisted of 1,610 pregnant women: 504 high-risk and 1,106 low-risk (Fig. 2 and Table 3). The high-risk weighted average for (number of hospital stay days×number of patients)/total number of patients was 3,307/504, or 6.56. The low-risk weighted average for (number of hospital stay days×number of patients)/total number of patients was 6,245/1,106, or 5.65.
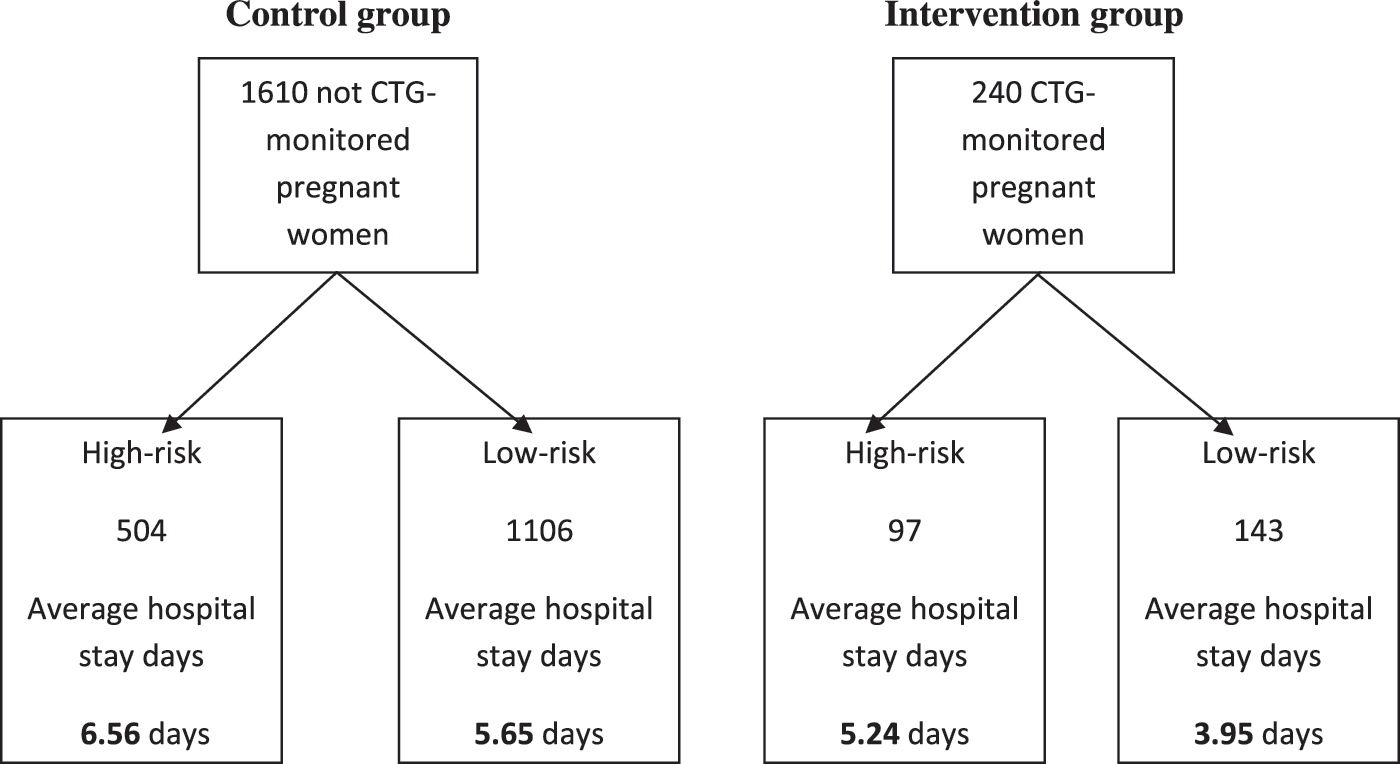
Case-control study design. CTG, cardiotocography.
Control Group Patients
The case group consisted of 240 pregnant women: 97 high-risk and 143 low-risk (Fig. 2 and Table 4). The high-risk weighted average for (number of hospital stay days×number of patients)/total number of patients was 508/97, or 5.24. The low-risk weighted average for (number of hospital stay days×number of patients)/total number of patients was 565/143, or 3.95.
Case Group Patients
The number of hospital stay days saved was multiplied by the DRG 384 value of the hospital stay day. This value is obtained by dividing the value for National Health Service cost/DRG 384 value of regional hospital stay for the total number of hospital stay days: DRG 384 value for 1 hospital stay day in hospital=€260.00.
Analysis Of The Economic Impact Of Technology
TOCOMAT technology had an economic impact on both the efficiency of the Department of Prenatal Medicine of the “Federico II” University Hospital of Naples, by reducing the average hospital days, and in the Campania region, with the creation of a network of units remotely connected to the operations center.
Tocomat economic impact on the operations center at the Department of Prenatal Medicine at the “Federico II” University Hospital of Naples
This study showed the cost savings related to the reduction of the average hospital days at the Department of Prenatal Medicine. In fact, the “Federico II” Management Control estimated that the average daily cost of hospitalization is around €700, and comparing the calculations with the average daily remuneration in reference to DRG 384, the efficiency derived by any reduction in the average of hospital stay days becomes evident. In particular, this study has shown significant cost savings for both high- and low-risk patients (Table 5). For high-risk patients, the reduction of the average of the hospital stay days was 1.32 days, with an average cost of €812, which, based on the 97 cases analyzed, resulted in a reduction of €89,628. For low-risk patients the reduction of the average of the hospital stay days was 1.7 days, with an average cost of €1,190, which, based on the 143 cases analyzed, resulted in a reduction of € 170,170.
Analysis of the Reduction of Hospitalization Cost
Economic impact of the regional telemedicine network
In order to evaluate the effects of the regional TOCOMAT network, we need to clarify how the system works and estimate the costs for the remote transmission of peripheral areas to the operations center. However, this study does not take into account an important implication of TOCOMAT: that monitoring patients in peripheral areas remotely connected to the operations center has a larger significance. In fact, it is not possible to do an assessment of the effects on the average of the hospital stay days, like the one performed at the Department of Prenatal Medicine, because data for these patients monitored in peripheral areas (Level I) are missing (because delivery has not always been at the Department of Prenatal Medicine).
The main equipment at the operations center consists of a computer (OB Trace Vue) that acquires digital CTG signals and patient information, displays the traces, stores all the data on a hard disk, and transmits them to another system for computerized analysis. Within a few minutes, all data and the medical report are printed and faxed back to the peripheral unit.
The costs of our analysis were those borne by the Department of Obstetrics, Gynaecology, Urological Science and Reproductive Medicine of the “Federico II” University Hospital during the year 2011. Costs were calculated for the equipment and the workings of the operations center and of the eight peripheral units. The costs included equipment depreciation, maintenance, charges for electricity, the salaries of medical personnel, CTG paper, CTG bands, consumables per patient (gel, paper for the bed, and paper to dry), and the SIM card.
The costs were calculated on the basis that the units worked 6 h a day (from 8:00 to 14:00 h), 5 days a week. The recording of a trace takes about 45 min, so eight pregnant women can be monitored by a single CTG unit each day. The CTG device is simple to use, although a physician is required at the sending end, as well as a physician at the operations center.
The annual cost of CTG monitoring at the operations center was €104,480.13. The annual cost of operating a single peripheral unit was €101,884, and so the cost of all eight peripheral units was €713,188. Thus the total annual cost of the telemedicine network, including €30 for the SIM card, was €817,698.13. Table 6 shows the complete cost analysis for the autonomous operations center and the eight peripheral units in the system.
Cost of the Telemedicine System
CTG, cardiotocography.
Discussion
As we described in the Introduction, a health technology assessment is based not only on its cost and benefit evaluation, but also on its possibility to provide policy makers a management on decisions and outcomes.
Benefits obtained must be “quantified” both in the programming phase of the investment (based on the current structure of the operating systems) and in the phase of verification of the improvement obtained. In fact, monitoring and measuring the advantages of the decision are needed, as the “moving target problem” 7 is described—that is, the possibility that the evidence provided in the assessment phase may be overcome in time because of the innovation in technology or because of different modes of use of technology. That is why technology assessment must be considered as a dynamic process, to be reviewed periodically and not as a static analysis.
In the case we examined, the common indicators of “economic advantages” of the investment, which had shown efficiency of the adoption of CTG at both the micro (the “Federico II” University Hospital of Naples) and macro (Campania region) levels for the realization of the TOCOMAT network, must be associated with specific assessments of the benefits expected from the introduction of a computerized CTG system, especially in reference to the main parameters of efficiency and of “value” for patients.
In the case of CTG, the users are the pregnant women, for whom the expectations are not only safety and efficacy, but also humanization and comfort, which are hard to measure with quantitative variables.
At present, we are considering the possibility of offering satisfaction questionnaires to pregnant women and medical staff. In this phase we wanted to clarify the evidence derived from the 10-year adoption of the technology: • Reassuring the woman in labor. The computer analysis is able to extract all the information contained in the fetal heart rate, such as the short-term variability, the nonlinear control system of the fetal heart rate, and the periodic modifications of fetal heart rate generated by the cardiac pacemaker. They are “objective” parameters, which overcome the limits of the conventional method, such as the significant inter- and intra-observer variability and the human inability to extract quantitative information from the fetal heart rate.
8,9
• Reducing usage of the emergency department. In peripheral units, patients are monitored once a week, or more often or daily if maternal and/or fetal complications appear. This reduces turning for healthcare to the emergency department, which occurs only when necessary, avoiding overcrowding and psychological stress for the patient. By now, this indicator is difficult to estimate because a centralized system to record the total number of contacts of every woman does not exist. A pregnant woman can freely decide where she wants to be assisted during her pregnancy, and she can also choose a different place for delivery, with a possible fragmentation of the “delivery” process. • Reducing repeated hospitalizations. The constant interaction between experts of the operations center and the operators at the remote unit allows the planning of hospital admissions, which are offered to patients only when strictly necessary. In this way, the quality of care provided to pregnant women is improved because they take advantage of the CTG monitoring and of the advice of doctors at the operations center. • Humanizing the delivery. The woman assisted with this system gains more awareness because she is informed about the real fetal well-being, recovering her role as an “active player” during the delivery. Furthermore, the reduction of improper recourse to the emergency department and of the repeated hospitalizations avoids having the woman to leave her family for long periods, thus avoiding logistical and organizational problems.
In this study, the proposed technology is efficient in the economic terms of cost-effectiveness because it provided considerable cost savings to the “Federico II” University Hospital of Naples, as demonstrated by the case-control study.
Moreover, the simplification of reporting processes of the CTG allows the following: • compensation for the lack of adequate skills in reading the CTG traces by doctors, avoiding problems of interpretation • ensuring the rapidity of communication of diagnostic response, with the possibility of a reduction of turning for healthcare to the emergency department and a more rapid clarification of the clinical status of the pregnant woman and of the fetus (quickness of decision-making affecting the appropriateness of therapies or the safety of discharges); and • ensuring rapid response to the patient, optimizing both health and perceived efficacy (that is, accessibility and timeliness) in solving a clinical question, generating trust and loyalty in the individual who needs healthcare
Footnotes
Disclosure Statement
No competing financial interests exist.