
Abstract
Introduction
Researchers in various fields like medical science, computer networks, and advanced communication systems are working together in order to make a broader smart e-healthcare unit or telemedicine system possible. The crisis of availability of good medical doctors, nurses, clinics, or hospitals and excessive cost incurred during medical treatment increase the seriousness of the problem. Because of the unavailability of these factors, telemedicine is needed to collect the vital information from patients remotely through a telemedical hub (TMH). The body area sensor network is a set of several nodes distributed over the body to collect physiological information. These networks are usually meant for the acquisition of data. The wireless body area network (WBAN) infrastructures are complex and need many functional support elements. WBAN is also called wireless personal area network (IEEE 802.15-WPAN), where current technology allows very tiny radio transmitting devices to be securely installed on a human body. Biosensors are attached to the body for remote health monitoring with extremely high mobility. It consists of three types of nodes: (a) an implant body area network (BAN), used for internal communication around the inside of the body where sensors and actuators are connected to the BAN coordinator (BANC) that serves as a data acquisition center; (b) external BAN, for external communication between sensor nodes surrounding the body and the outside world, not contact with human skin; and (c) surface BAN, placed on the surface of the human skin. 1 These data are collected by telemedicine systems through the faster network connectivity for processing and analysis. Chen et al. 2 presented the difference between a wireless sensor network and BAN in terms of mobility, data rate, latency, node density, power supply, network topology, node replacement, security level, etc., and also compared them with existing body sensor nodes. 3 –5
Several ongoing projects like firmware-based CodeBlue, 6 MobiHealth, 7 AlarmNet, 8 the advanced care and alert portable telemedical monitor (AMON), 9 MagIC, 10 medical remote monitoring of clothes (MERMOTH), 11 microsystems platform for mobile services and applications (MIMOSA), 12 wireless sensor node for a motion capture systems with accelerometers (WiMoCA), 13 CareNet, 14 Advanced Health and Disaster Aid Network (AID-N), 15 SMART, 16 ASNET, 17 MITHril, 18 wearable health monitoring systems, 19 NASA-Lifeguard, 20 the noninvasive LifeShirt, 21 iSIM, 22 HealthGear, 23 ubiquitous monitoring (Ubimon), 24 eWatch, 25 Vital jacket, 26 m-health, 27 Personal Care Connect, 28 and HeartToGo 29 have contributed to establish practical solutions for WBAN. Chin et al. 30 highlighted power-efficient and energy-efficient solutions toward in-body and on-body sensor networks. According to a World Health Organization report, approximately 17.5 million people die because of heart attacks each year, more than 246 million people suffer from diabetes (increasing to 380 million by 2025), and almost 20 million people will die from cardiovascular disease in 2025. 31 So these deaths can be potentially prevented in the help of WBAN-based telemedicine systems. Medicine is the third largest market for wireless sensors (Fig. 1).
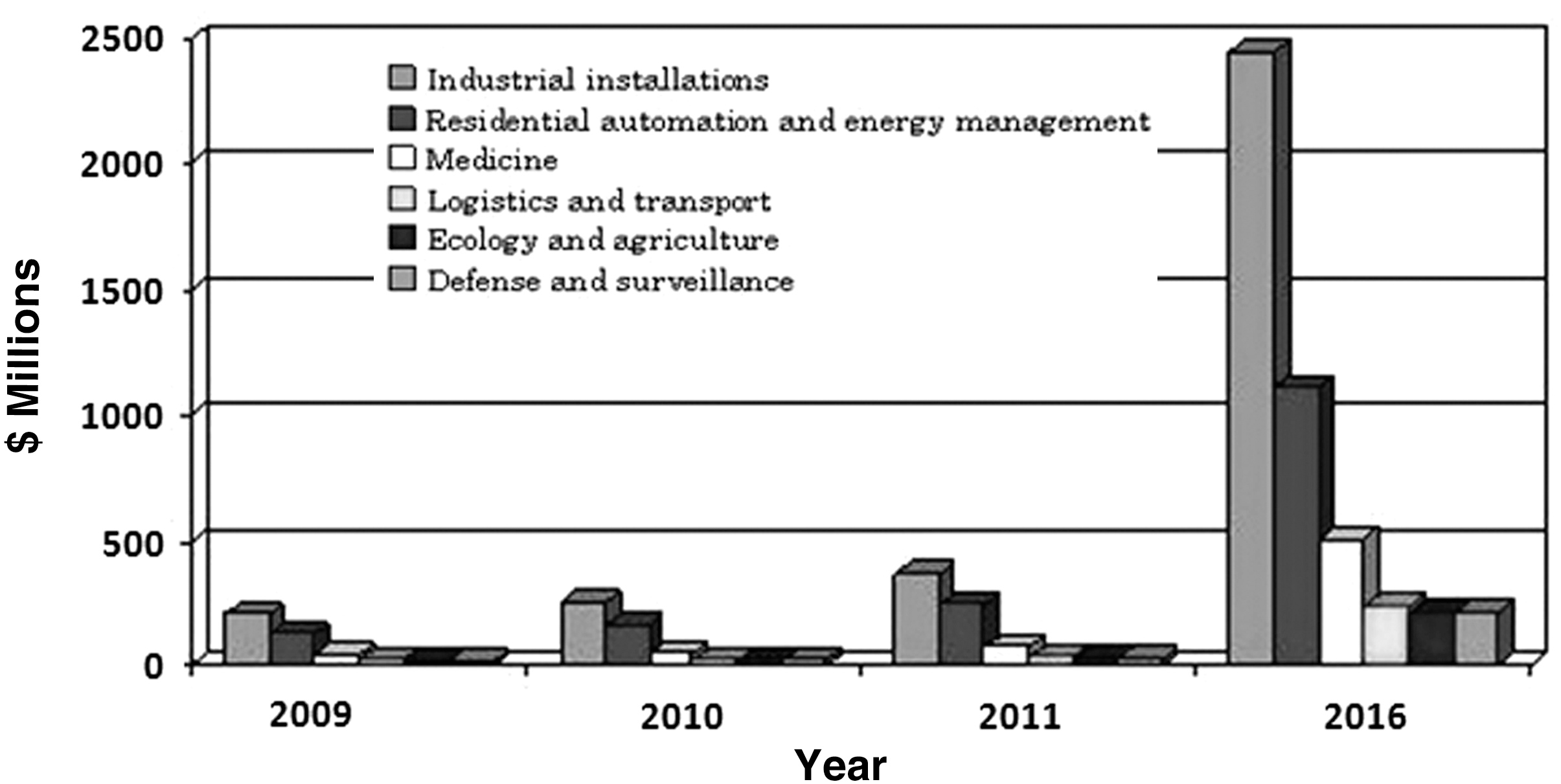
Value of the global market for wireless sensor devices by end vertical application (from BCC Research 32 ).
Issues and Challenges
Various WBAN-related issues and challenges are addressed here. The important issues and challenges are as follows: need for extremely low-power operation, lightweight, avoidance of wearable/implantable sensors, maintenance of security and privacy, reliable transmission of patient's vital data, emergency medical care, real-time connectivity over heterogeneous networks, low complexity, standardization, interoperability, low cost, and better quality of service (QoS). 33
Various Types of Sensors
A typical WBAN consists of several sensor nodes with a low power constraint, each acquiring a specific physiological parameter from the body. These nodes act as a bridge between the patient and technology-enabled devices. We can easily capture important aspects of the patient's health status, and early detection of abnormalities is also possible using sensor nodes. Response to these data should lower mortality. An efficient WBAN requires sensors with the following properties: portability, lightweight, low power consumption, and miniature and autonomous sensor nodes that monitor the health-related applications. The obvious applications are as follows: (1) an electrocardiogram sensor, which can be used for monitoring heart activity; (2) an electromyography sensor, which monitors muscle function activity; (3) an electroencephalogram, which monitors brain electrical activity; (4) a blood pressure sensor, which measures the force exerted by circulating blood on the walls of blood vessels; (5) a tilt sensor, which monitors trunk position; (6) a breathing sensor for monitoring respiration; (7) motion sensors, which can be used to discriminate the user's status and estimate level of activity; (8) body temperature; (9) a pulse oximeter, which indirectly measures the oxygen saturation levels in an individual's blood; (10) respiration; (11) blood sugar; (12) carbon dioxide monitor; (13) blood pressure; (14) a capsule endoscope; (15) a phonocardiogram; (16) an accelerometer, which is used for motion capture; and (17) a cardiac defibrillator. All the body sensor nodes are in close proximity (a maximum of 2 m) to the centralized BANC. The most challenging issues are as follows: (a) these sensor nodes must have the flexibility and freedom to move to acquire the patient's condition; (b) we should try to minimize the number of sensor nodes, thus reducing the signal-to-noise ratio; (c) a properly planned location is needed with high accuracy; (d) a convergence device is required to gather multiple signals from the human body; and (e) body sensors should be optimized. Cordeiro and Maulin 34 discussed various technical issues typical of data rate, bandwidth, latency, etc. Table 1 depicts the functional requirements of BAN technology.
Functional Requirements of Body Area Network Application
ECG, electrocardiogram; EMG, electromyogram; Kbps, kilobits per second; Mbps, megabits per second.
Medical Data Management
The major objectives of medical data management are as follows: to improve patient care remotely with database support, to reduce health expenditure, and to give better consultancy by physicians. The main function of this unit is to collect patient physiological data and forward them to the medical center in an efficient and reliable way. The data can be classified as follows: (a) patient personal data (i.e., patient ID, name, address, date of birth, birth place, sex, etc.); (b) patient medical data (i.e., plain text, image, textual, video, etc.); (c) doctor's/medical expert's personal data (i.e., doctor's personal information, unique identification code); and (d) system management-related data (i.e., patient list, password files, log files, etc). 35 The medical data management is also responsible for accepting and recording emergency calls when the information is passed over high data rate technology, and, as well, it can maintain the patient history file for future analysis (Fig. 2). The electronic health record (EHR) and data analysis module can be integrated to the TMH for storing and analysis for diagnosis. The data acquisition center can be integrated with the BANC for data acquisition with statistical modeling. The patient information, medical data (i.e., signs, symptoms, test reports, etc.), archival and retrieval of patient records, and appointment scheduling have been covered by this unit. Standard databases like ORACLE, DB-2, SYBASE, MySql, and MS-SQL can be used to store the important patient's information record. 36 The fault-tolerant system operation and troubleshooting facility are needed for smart communication.
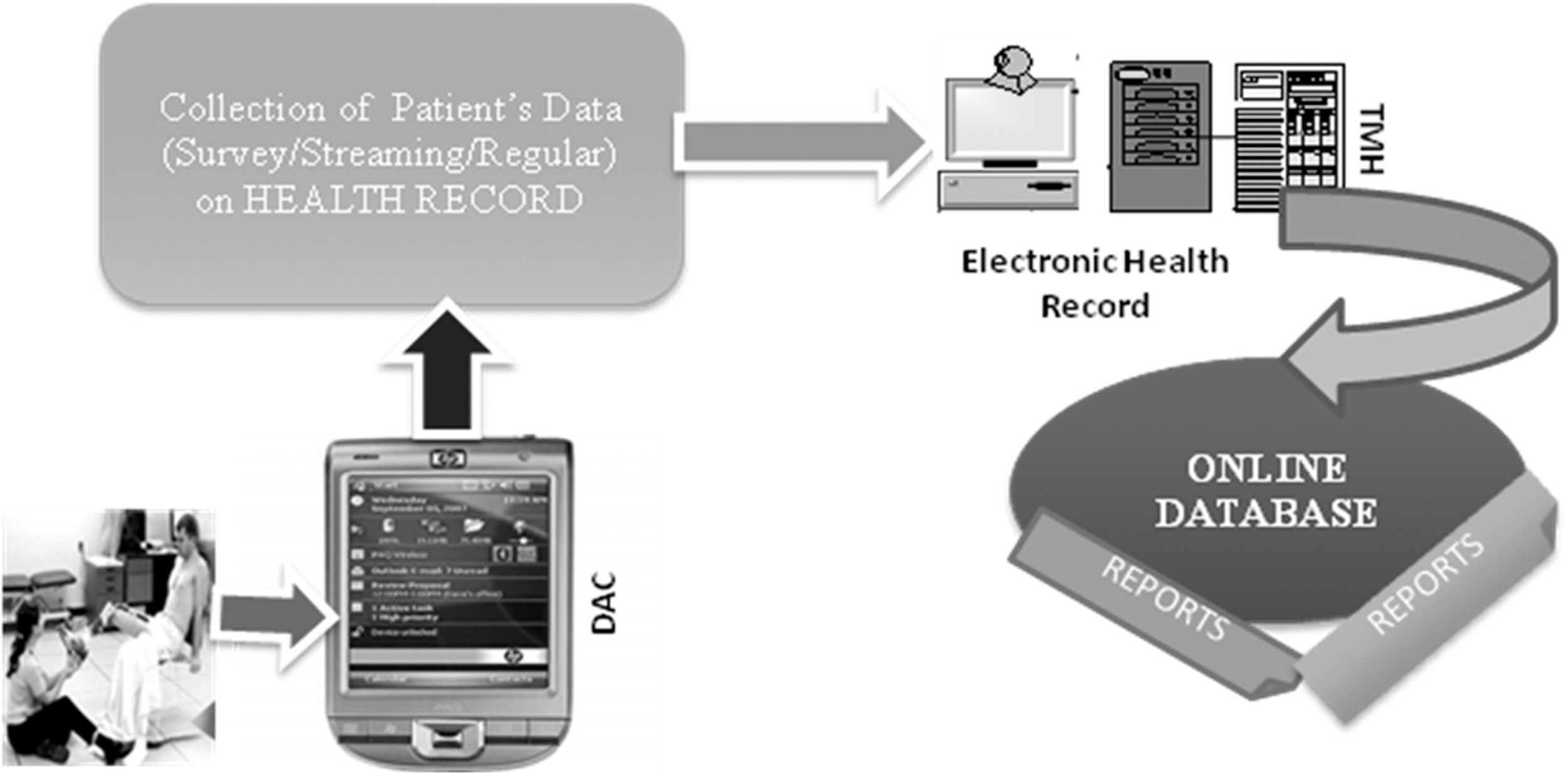
Eliminate human intrusion during analysis. DAC, data acquisition center; TMH, telemedical hub.
Routing Techniques
Various types of intelligent medical sensor devices can be placed on the human body. The physiological information is received from sensor devices and processed to the BANC. One of the critical issues in the implementation of WBAN is the design of routing structures and routing protocols. The routing protocols can be classified into two broad categories: (a) flat-routing protocols, where each sensor node in the WBAN plays the same role; and (b) hierarchical/cluster-routing protocols, where different sensor nodes may play different roles. With the help of the routing technique, we can easily measure the energy with respect to how many packets will traverse that route from the sensor nodes to the BANC. Hadda et al. 37 introduced five routing strategies: thermal-aware routing protocols, cluster-based routing protocols, cross layer-based routing protocols, QoS-used earlier-aware routing protocols, and delay-tolerant-aware routing protocols. Multi-hop routing algorithms like Low-energy Adaptive Clustering Hierarchy (LEACH), 38 Power-efficient Gathering in Sensor Information Systems (PEGASIS), 39 and Hybrid Indirect Transmissions (HIT) 40 are required for single cluster-based WBAN, where LEACH is responsible for transferring the data from sensor nodes to cluster heads or BANC with a minimum energy transmission scheme, PEGASIS is near-optimal chain-based care of data processing in terms of data fusion, which helps to reduce the amount of data transmitted between sensor nodes and the BANC, and HIT provides alternate routes to the BANC with the prevention of skin heating. This article also highlighted the advantages of the routing technique in WBAN. In reliable energy communication, the routing algorithm is responsible not only for the distance of each link but also its quality in terms of error rate as well. The routing mechanism will affect the end-to-end path reliability. An efficient routing mechanism is required for processing the vital information with optimal criteria.
QoS Requirements
Medical information has privileged precedence in communication networks. WBAN QoS is a critical parameter for any communication. The QoS issue in WBAN requires more interest because of the critical level of operations. The highest QoS is required for the operation of elderly heart patients. In order to achieve maximum throughput, minimum delay, buffer size limitation, removal of redundancy, and maximum network lifetime, QoS is needed. 41 It supports a bit error rate from 10−10 to 10−3, and latency in medical application should be less than the 125 ms, shown in Table 1. A WBAN should support QoS management features to offer better priority services. The main parameters of the medical QoS will be the bandwidth, packet transmission delay, packet loss, and link loss in the network in the healthcare domain. The path initialization, modification, and termination are required before the physiological data packets are sent from the WBAN to the TMH. Therefore signaling interworking between the WBAN and other networks is needed (Fig. 3).

Wireless body area network (WBAN) signaling Internet working and traffic pattern. BANC, body area network coordinator.
The traffic flow depends on multiple sensor node-to-sensor node, sensor node-to-sensor node, and sensor node-to-multiple sensor node architecture. The details of traffic classification have already been introduced. 42
Normal traffic is used to monitor the normal condition of the patient without a critical condition. These data are collected and processed by the BANC.
Emergency traffic is initiated by body sensor nodes when they are exceeding a predefined threshold. It is absolutely unpredictable.
On-demand traffic is initiated by the TMH and is associated with the doctor or clinician attempting to acquire certain information for diagnosis and prescription purposes.
Communication Path
The bandwidth requirement for WBAN is relatively low. WBAN provides a flexible data rate from 10 kilobits per second (Kbps) to 10 megabits per second (Mbps). Every sensor node can operate at 250 Kbps because of the duty cycling mechanism. An efficient compression algorithm is needed for medical data transmission. Reliability is another key factor in communication systems.
Standard/Technology (Table 2)
A WBAN uses licensed wireless medical telemetry services (WMTS) for a medical telemetry system, an unlicensed ISM band (2.4–2.4835 GHz), and ultra-wideband (UWB) and medical implant communications service (MICS) bands for data transmission. The WMTS band is also used by other technologies, such as wireless fidelity (Wi-Fi
Comparison of Different Standard Protocols
AES, advanced encryption standard; CRC, cyclic redundancy check; IR, infrared; Kbps, kilobits per second; LOS, line of sight; UWB, ultra-wideband; WiBro, wireless broadband.
Security
Another major concern in WBAN infrastructure is security. The BANC receives the set of physiological data about vital parameters from several parts of the patient's body. After that the data are processed over advanced communication paths to the TMH securely. This security scheme is dependent on factors like data confidentiality, data integrity, authenticity, non-repudiation, availability, data freshness, secure localization, and privacy. Lim et al. 57 discussed the risk assessment scheme for the telemedicine system in terms of data collection, processing, transmission, storing, and sharing. Health data are private and sensitive information, so that the security of data transmission within a BAN becomes a critical issue. TinySec 58 is the first fully implemented link layer security architecture for wireless body sensor networks. It generates secure packets by encrypting data using a group key shared among sensor nodes and calculating a message integrity code for the whole packet, including the header. WiMax (IEEE 802.16d) offers well-built security measures to protect against an extensive variety of security threats. The current research trends of the BAN-security framework have been demonstrated in the help of major protocols like security protocols for sensor networks (SPINS), 59 localized encryption and authentication protocol (LEAP), TinySec, ZigBee (commercial mode), and security manager. 60,61 The Health Insurance Portability and Accountability Act of 1996 62 has ensured a set of mandatory privacy issues to protect sensitive personal identifiable health information. The WBAN is dealing with private patient data, so a cryptography-based access control scheme is needed to protect the privacy of patients.
Simulation Environments
Various research agencies use different simulation environments for the performance evaluation of WBAN. The most fashionable tools are those like OPNET Modeler, 63 Network Simulator-2, 64 GLOMOSIM, 65 QUALNET, 66 the OMNET++ platform-based open source Castalia simulator, 67 mixed simulator (MiXim), 68 or the discrete event simulator TinyOS 69 or TinyOS-based TOSSIM. 70 None of these simulation tools perfectly meets the demands of wireless sensor networks.
Proposed WBAN Framework
The modeling and visualization of telemedicine-based WBAN systems represent another upcoming era of sensor networks. Figure 4 illustrates a proposed framework of a body area sensor network–based telemedicine system. It consists of three phases based on the usability of the standards and technologies. Our objectives are (a) how to gather and process vital patient information, (b) how to transfer the data quickly and securely, and (c) how to monitor and diagnosis the vital information accurately and quickly.
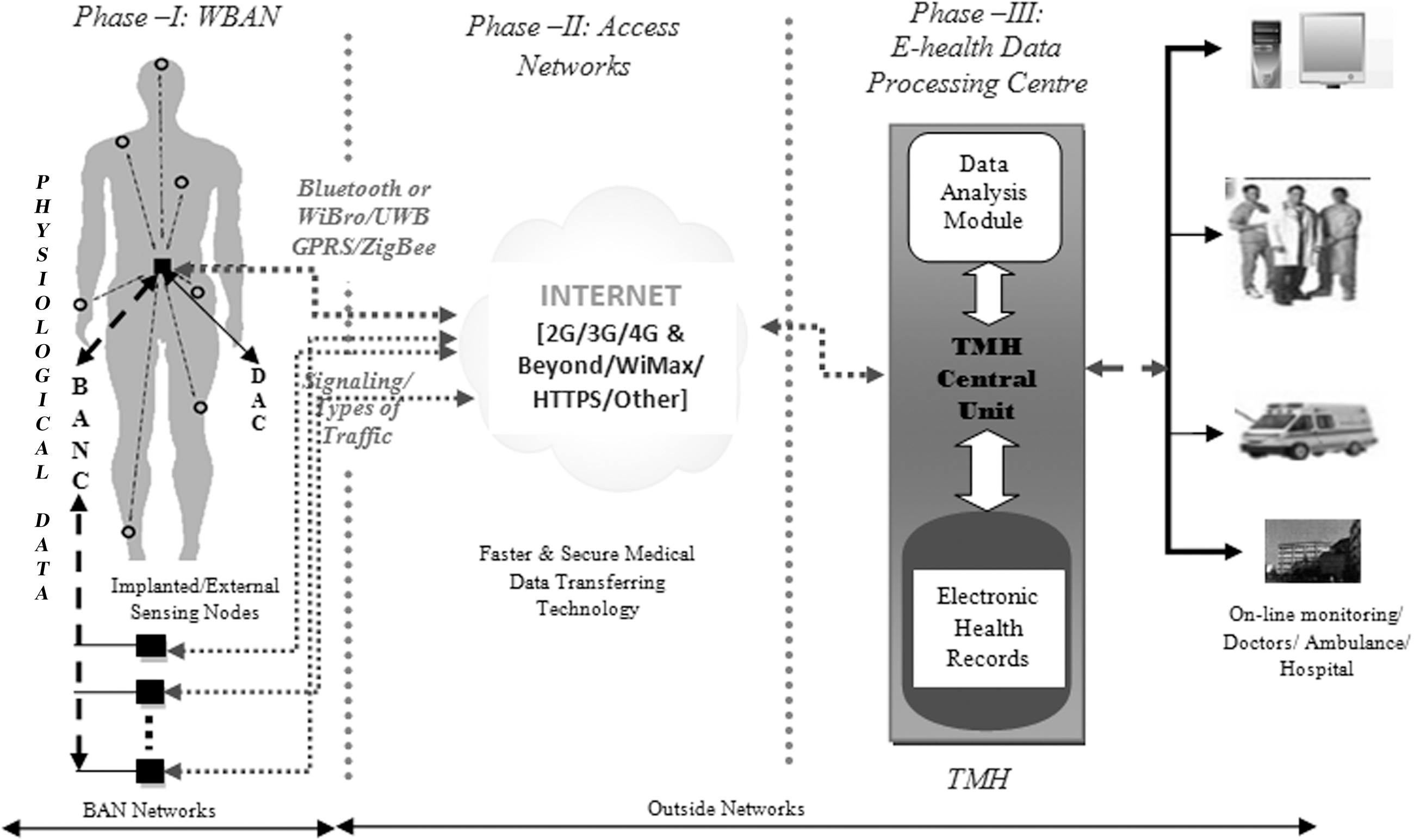
Proposed telemedicine system with remote monitoring facility. BAN, body area network; BANC, body area network coordinator; DAC, data acquisition center; TMH, telemedical hub; WBAN, wireless body area network.
In Phase I, a WBAN consists of several in-body and on-body sensor nodes, each acquiring specific physiological data from the human body and communicating with the master node, known as the BANC. Usually, a star topology 71 is quite sufficient in WBAN (network coverage of 2 m or extended to 5 m) where the BANC is centrally located and every sensor is directly connected with the master node. In general, multiple BANCs are needed for continuously receiving the clinical data from source nodes. Based on the criticality of patients the data are processed and forwarded to the expert doctors (and stored in the medical server) via the TMH. The statistical modeling, compression, privacy maintaining, optimal path designing, and scheduling process may be implemented here. A Picture Archiving and Communication System–based telemedicine system is needed for image and data acquisition purposes. 72 Technologies like Bluetooth or low-power Bluetooth (i.e., WiBro), UWB, global packet radio service (GPRS), and ZigBee are most widely used in WBAN for transferring the health status information from sensor nodes to the BANC.
In Phase II, faster and secure services are needed for the physiological data transfer from the BANC to the TMH. The evolution of wireless communication systems from 2G to 2.5G (iDEN 64 Kbps, GPRS 171 Kbps, EDGE 384 Kbps), 3G (WCDMA, CDMA2000, TD-CDMA), and 4G systems will facilitate the provision of a faster physiological data transfer rate. The beyond 4G infrastructure is also introduced to provide faster processing of the real-time secure patient's data in a critical or non-critical condition remotely. 73 Hypertext transfer protocol secure is widely used to protect the patients' clinical data through the establishment of end-to-end secure sessions over the Internet and to ensure the confidentiality and integrity of data. Oleshchuk and Fensli 73 also indicated the limitation of previous technology (i.e., a GPRS system will normally prevent a real-time transmission of medical waveforms from a sensor on a human body).
In Phase III, the patient's vital data have been received by the TMH central unit and stored in the EHR, where the patients' records are maintained. The EHR is a secure, structured, digitized, real-time, point-of-care, patient-centric, and fully accessible information resource. It also maintains the clinical care unit that is associated with billing and pricing, quality management, reporting, and public health disease surveillance and reporting. The EHR will be incorporating the evidence-based decision support facility by handling the large volume of data. The data analysis module is associated with this hub for analyzing the clinical data to increase the patient volume through early diagnosis. The disease-wise specialist doctors, nurses, hospitals, and clinics are associated with the TMH for constant health status monitoring of a patient's health condition. The telemedicine system can be categorized into three sections: store-and-forward, remote monitoring, and live/interactive services. This hub also enables an efficient, effective, and equitable process of medical services delivery with improved patient safety and quality of healthcare.
WBAN Application
There are so many applications in the area of WBAN, like medical, sports, and military applications, because it provides portability, freedom to move, low power consumption, safety for human exposure, monitoring the human physiological activities, higher security protection, reduced clinical errors, and more significant in real-time data delivery. Current telemedicine applications of BANs target wellness monitoring, stress monitoring, heart problems, emergency response, asthma, deep brain stimulation, implanted drug delivery, cancer detection (ability to detect nitric oxide from cancerous cells), 74 and detection of abnormal situations with elderly depressed people. This network can also help blind people using implanted retina prosthesis chips. As well, WBAN provides the applications to situations such as (a) early intrusion, in that doctors can catch issues before the patient's condition becomes critical, (b) infection control, to reduce the risk of infection and need for cleaning procedures by using WBAN, (c) ease of patient transport, in that there will no longer be a need to disconnect and reconnect wires prior to transporting a patient, and (d) flexibility, in that a doctor will be able to quickly add or remove sensors for measurement of different physiological parameters as medical conditions warrant.
Conclusions and Future Work
In this article, we have discussed the major aspects of WBAN in terms of information gathering, processing data, and storing data from and monitoring of patients. This article also presents a scalable architecture of WBAN to provide patient health data in real-time. This architecture defines the QoS requirements for integration of both internal and external sensors into an autonomous system. A list of sensors and communication technologies has been presented. We have compared our approach with Wi-Fi, Bluetooth, Wibro, ZigBee, etc. Further, the article presents the key aspects for designing low-cost, unobtrusive, low-power telemedicine-based WBAN for healthcare monitoring. This article can be considered as a source of motivation for future research dimensions. Researchers have been developing signaling for very low power consumption. The specific absorption rate is also estimated from the safety point of view. The scope of our work is to minimize the health hazards from radiation because WBAN consists of multiple sensors. Engineers or computer scientists have been designing the advance technology-based WBAN model and improving its performances. So good communication is needed between doctors and engineers dealing practically with the WBAN platform. The hybrid authentication model is also needed to handle the large amount of data.
Footnotes
Disclosure Statement
No competing financial interests exist.