
Abstract
A biobank is a biorepository that stores biological samples (usually of human origin) for use in research. Since the late 1990s, biobanks have become a key resource, supporting contemporary research in many fields, including genomics and personalized medicine. The ethical requirement for anonymity currently results in irreversible severing of the link between patients and their biobank samples. However, the maintenance of an anonymous link would increase patients' control over their samples and the efficacy of sample management. We propose a system for anonymous, real-time communication between the biobank and the patients providing samples based on the short message service (SMS) of mobile telephones. The patient and the biobank communicate via a cryptographic protocol, using a trusted third-party server. The biobank-SMS (BioK-SMS ) communication system provides answers to certain persistent ethical questions relating to biobanking. BioK-SMS makes it easier to obtain renewed consent when required, gives patients more control over their samples, and protects their privacy.
Introduction
The Organization for Economic Cooperation and Development defines a biobank as “a collection of biological material (e.g., tissues, cells, blood), the associated data, and information stored in an organized system, for a population or a large subset of a population.” Biobanks have invested in the creation of international scientific collaboration networks for the harmonization and standardization of techniques and data exchange. However, ethical aspects has not kept pace with biobank development. 1
How can we best guarantee donors' rights to autonomy and the protection of their private lives, without limiting the field of scientific investigations? Researchers sometimes need to add information to their sociodemographic and environmental databases, like in longitudinal case studies of population aging, in which patients must be recontacted. Conversely, some patients may wish to be informed of the fate of samples or of scientific results. In such cases, patients and samples must remain linked. For traditional biobanks and stem cell banks, this requires improvements in anonymization tools, for the maintenance of traceability, to ensure high quality without donor re-identification. This would help patients' association to motivate donors and to obtain financial support. Patients are the principal stakeholders in medical and biotechnological advances because only they can consent to the often-anonymous donation of their samples. For the initial use of samples, patients are informed of the reasons for which the sample is requested, the aim of the study, and the fate of the biological samples, 2 when consent is given. Specific consent is required for the use of samples in the creation of biological collections and in genetic or pediatric studies in which consent must be obtained from the parents or guardians of minors. 3 In other situations, individuals may have died since giving consent. Many such patients will have had complex diseases that are still being studied, such as neurodegenerative diseases. The use of their samples may thus be compromised. 4
Various legal and ethical dispositions are in place in different countries, to allow the use of these samples. The situation is even more complex in cases of a change of use or secondary use of the samples, 5 although patients' relatives can be asked for authorization. Ethics committees can provide general answers to certain ethical questions. In this particular situation and, indeed, generally, samples are rendered irreversibly anonymous to ensure they cannot be traced back to patients. However, more effective solutions are required to avoid the non-use or loss of precious samples. The most striking example concerns the prospective or retrospective use of embryonic stem cells, 6 a very promising and potentially lucrative domain that can be used to repair damaged tissues in patients. Such work is currently confronted with the problem of finding and recontacting patients when researchers find a potentially interesting use of samples other than that for which they were originally collected. 7
It was hoped that the use of induced pluripotent stem cells and their derivatives would overcome the need to recontact patients. However, induced pluripotent stem cells and donor cells are almost identical genetically, raising potential ethical questions concerning the rights of the donor, which could jeopardize the use of these stem cells. 8 Another ethical minefield concerns the discovery of a disease or disease predisposition in the patient, such as predisposition to breast cancer, for example, for which treatment is effective if initiated sufficiently early. Who is ethically responsible for divulging this information to the patient? 9 We must also consider the legitimacy of patients wanting to know whether their samples are still stored in the biobank or have been destroyed. By dealing with these aspects, we might be able to encourage reticent subjects to give consent, to reassure those who have already given consent, and to maximize the utility of samples already donated. It is also essential to maintain confidentiality, one of the key elements restricting the management and use of biological specimens. Improvements in these aspects would provide patients with greater autonomy, including the freedom to withdraw their commitment, or their samples from the biobank, at any moment. A sample stored in the biobank may be useful for studying several diseases, but consent is generally given for a particular target disease, for which the patient consulted or was hospitalized. Furthermore, the samples stored may be insufficient for detailed explorations or for the needs of collaborative research projects, particularly for neuromuscular samples or other samples stored in tumor banks. Clinical and biological data remain available in dedicated databases, but the lack of a sample may add to the frustration of researchers unable to find answers to their questions.
The use of mobile telephones has often been considered in clinical medicine. 10 Studies have confirmed the efficacy of mobile phone-based methods in studies of observance 11 and even in emergency situations in which the doctor needs to obtain consent for patient management. 12 Biobanks could make use of this to contact patients in an anonymous, secure manner, via a trusted third-party server.
Description of the Potential Short Message Service
The biobank–short message service (SMS) system (BioK-SMS) ( Fig. 1 ) could fulfill this purpose. It is based on several steps:
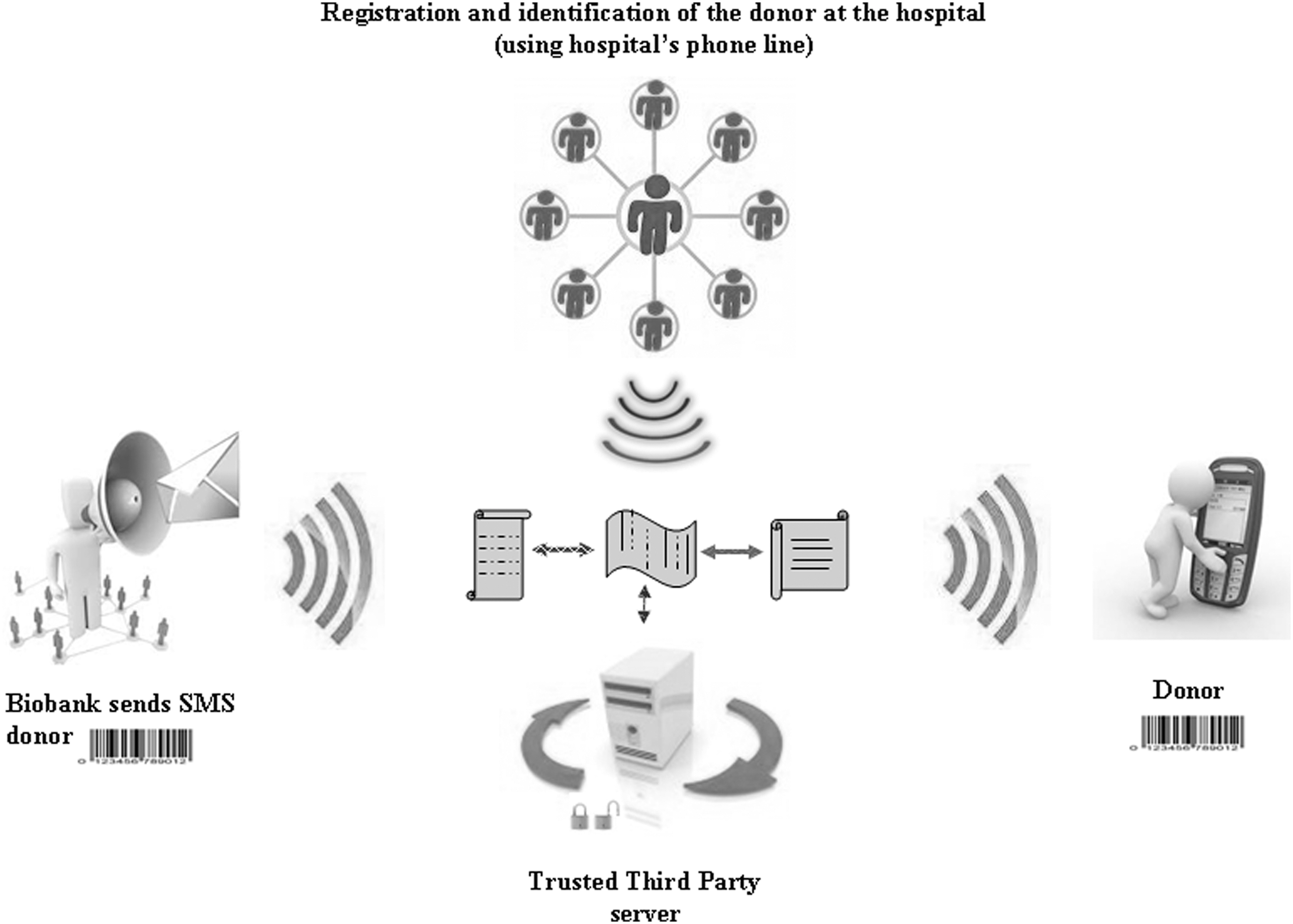
Biobank–short message service (Biok-SMS) system.
1. At the hospital, patients use a hospital mobile telephone to identify themselves as sample donors on the biobank server, by entering an identification code consisting of, for example, their date of birth (18011955), sex (M), a personal code consisting of their time of birth, in hours and minutes (2330 would correspond to 11:30 p.m.), and the mobile telephone number (0660039764) via which the server can contact the patient. The nurse provides the patient with a sample code (e.g., BLD), 13 a collection code (e.g., A for arthritis), and a sampling service code (e.g., 1 for the rheumatology department). The identification code for this example would thus be 18011955M23300660039764BLDA1. The biobank server is configured to generate a sample number from the identification code (e.g., 58124BLDA1). It is also possible to have a mixed code, with the number coded as a pictogram or bar code and the details of the sample visible.
The server then ensures that the number of the patient's sample (58124BLDA1) is associated with three other numbers: the patient's mobile telephone number (0660039764), the biobank mobile telephone number, and the patient's access code, according to the origin of the call. The sample number is sent, via the server, to the hospital mobile telephone, in the form of a text message (SMS). The mobile phone is linked to a printer, and labels bearing the sample number (58124BLDA1) are printed. These labels are stuck on the patient's medical file, sample tubes, consent form, and the form accompanying the sample. The samples are sent to the biobank labeled with a unique number attributed by the server, which may be a mixed code, containing anonymous information about the sample, a bar code, or a pictogram. Before leaving the hospital, patients are provided with information about creating their own personal code for access to the biobank via their personal mobile telephone, to enable them to follow the fate of their samples. The document provided includes information about the composition of the patient access code and the identification number, with no information about the samples (e.g., 18011955M23300660039764).
2. The biobank server acts as a “trusted third party,” a concept developed for another application. 14 The network from the identification code H (e.g., 18011955M23300660039764BLDA1) generates a sample code E (e.g., 58124BLDA1), which is stored on the server. E can recognize:
• The patient access code (18011955M23300660039764), allowing the patient to interrogate the server from his or her mobile telephone, A
• The biobank mobile telephone, by default, B
• The patient's mobile telephone (0660039764), P
If a call of type A is received, it is decoded into E, and the SMS is sent to B. If a call from B is received and the code E is given, the SMS is sent to P.
3. On request, the biobank technician calls the server and enters the unique code generated from the identification number. Patients changing telephone numbers can initially continue to enter the old code, containing the old number, for identification by the server. They can then select the appropriate button for a change of telephone number, as indicated by the server, and record a new code. Alternatively, patients without a new telephone number can place themselves in “standby” mode. If the biobank calls the patient, it then receives a message that the patient wishes to remain in contact and will soon provide a new number. With the new number, the server can keep the same identification code for the same patient. It may become possible for patients to use biometric methods to identify themselves. 15 The mobile fingerpass, 16 a fingerprint scanned with a mobile telephone that can be used as a secure entry code, constitutes a step in this direction, as would vocal and iris-based identification methods.
Discussion
Mobile telephone use in health is becoming inevitable. 17 SMS use has proven to be effective, particularly in behavioral studies requiring the maintenance of contact between the patient and healthcare professionals. 18 The main challenge will be convincing future sample donors of the benefits of using BioK-SMS. Even if patients are convinced of its utility, the key issue will be getting patients to use the system. On the day of the consultation, the doctor will inform the patient about the use of samples and the utility of BioK-SMS for following their fate and ensure that the conditions are satisfied for the patient to give written informed consent. Patients can then choose to proceed with BioK-SMS registration in the presence or absence of a person of their choice.
The principle of patient control over the future management of these samples comes into operation at this point. The parents or guardians of minors or of others unable to give consent will be asked if they wish to subscribe to BioK-SMS. Patients' rights remain central, but it is still necessary to convince clinicians and sample users of the value of this project. Indeed, the type of consent required for sample use remains a hotly debated issue, and BioK-SMS could help to reassure clinicians on this point. Will consent be general, or will it be necessary to adapt personal consent according to the planned study?
Patients are not only members of a society in which they can exert an influence, they are also influenced by others, in a sociocultural and geographic environment in which scientists make considerable efforts to provide responses matching societal expectations as closely as possible. Requesting informed consent for each project, as even adepts of this principle would admit, requires a particular type of management, with certain limitations, particularly when patients must be recontacted to request a renewal of consent (“reconsenting”). It is important for clinicians and users to be able to predict the next step in a study or the setting up of a new study for which fresh consent is required.
The potential utility of this system is most evident for precious samples and the protection of collections. In such cases, the patient could be asked to sign a general consent form as an alternative to giving fresh consent. The debate on this subject remains open. Many believe that the fundamental rights of the patient, control, and the obligation to provide information override other considerations and should not be eroded by the introduction of general consent, despite its utility and completeness. 19 Professional biobanks always ensure that their samples are stored in accordance with current legislation. In addition to being able to inform patients of the results obtained with their samples, biobanks wish to move toward optimizing the use of biological collections, requalifying their samples to change their end use, and ensuring that patient data are interoperable. In this context, patients could sign a basic consent form that could be expanded according to the type of research. In this case, overlap between research axes for a target disease or a well-defined population could be dealt with by an addition to the basic consent form and the information of patients that their personal data are to be used by another team for another research project.
This would make it possible to include the patient in a new cohort or a study concerning his or her genome. 20 The idea of basic consent would cover the initial use of the samples and would bridge the gap between major axes of research for subsequent use, increasing the changes of research success. However, it remains important to inform patients of all future projects in which they could become involved. Placing the patient at the heart of the process is no longer the issue. Kohane et al. 9 have already proposed a strengthening of the doctor–patient link in a scenario describing the study of a cohort of 5,000 patients. By placing technology at the service of the patient and research, access via an anonymous e-mail address could be used to provide the patient with the necessary information about the needs of the study in terms of participants and medical discoveries implying a need for patient care. Who would take responsibility for the necessary breach of anonymity in such cases?
It is also important that all patients included in the study have equal and regular access to the technology on offer, with access to a computer to obtain broadcast information at the very least and investment from administrative bodies for the implementation of this system. Progress is inevitable, and the Bio-PIN is another possible new communication solution. This initiative clearly responds to the demands of the ethics and scientific communities. It provides solutions based on communication technologies and can contribute to anonymous data management, patient control and privacy, and provide a balance between research needs and patient confidence.
Through the use of a smart card encoding personal data, patients can manage their samples anonymously, via a PIN code. 21 This requires patients to have access to a structure enabling them to manage their samples. The development of this system should make it possible for patients to obtain feedback concerning the results obtained with their samples. 22 The system could be adapted to the laws in force in the country of application, which must have the financial means to implement this rigorous technology; most mobile telephone contracts include free messaging.
Some countries of the North and East and many in the South have difficulty investing in health. By contrast, investment in the domain of mobile telephones has been inversely proportional to the economic situation of some of these countries. Fortunately, this trend has, in some cases, encouraged medical development, as at the Center for the Development of Best Practices in Health in Yaoundé, Cameroon. The Cameroon Mobile Phone SMS trial focused on ensuring compliance with antiretroviral treatment in patients from Cameroon. 23 This study confirmed that mobile telephones were an effective tool for remaining in contact with patients. The importance of biobanks in health development is understood in Africa. Gambia took a first step in this direction in 2000, with the creation of the first national DNA biobank. 24 Other major biobanking projects initiated in Kenya in 2003 aimed to get several countries to participate in the establishment of a pharmacogenetic database; these projects focused on the polymorphism, in various ethnic populations. 25 The authors were interested in malaria, human immunodeficiency virus, and other infectious diseases and recognized that future use of the pharmacogenetic biobank would require improvements in ethical aspects and sample anonymization.
In 2010, more than 500 million mobile telephones were sold in Africa, according to the International Telecommunications Union. African biobanks are therefore highly likely to be interested in the BioK-SMS concept. Other means of communication and information, such as public forums, Web sites, and newsletters, for maintaining direct contact between the patient and the project and creating a climate of confidence, were investigated in Japan by Watanabe et al. 26 In this context, the Biobank Japan Project, which began in 2003, aimed to constitute a database for 200,000 patients diagnosed with diverse diseases, including heart failure, cerebral infarction, and various types of cancer. This study appeared costly because considerable effort was invested in communication and the transmission of information to patients who had just signed consent forms. The results were mixed, with greater patient confidence but a probable loss of control due to these efforts at information and communication.
Do we need to define a clear threshold for researchers, beyond which they can approach a patient without decreasing patient autonomy? 27 The ideal would be for patients to take the initiative themselves, and the BioK-SMS concept is a move in this direction. The principal objective of this concept is relational in nature: allowing patients to choose, from the outset, to accept as much freedom as possible in the management of their own samples, in an anonymous manner. The collaboration between participants will operate at all levels of sample management, from consent and information to the communication of clinical results, finding patients, requalifying samples, inclusion in a new project, sample distribution, data interoperability, and the use of pediatric samples and samples from deceased patients, minors, and wards of the court.
Economically, the largest costs of the project relate to management of the server (the trusted third party). This cost could be reduced by negotiation and putting the contract out to tender, to take advantage of competition. The costs of telephone communications between the patient and the server will be covered by the biobank. The current generation of young adults is used to using smartphones for listening to music and downloading various applications for everyday life. This should strengthen the link between humans and machines, and this was one of the driving forces behind the BioK-SMS project. The mobile telephone can be customized according to the patient's needs: increasing the volume for the hard of hearing or the size of the text for those with poor vision. A themed ringtone can be chosen, and translation tools are available. With this approach, we have every chance of being able to maintain contact with the patient in legal and ethical conditions.
Footnotes
Disclosure Statement
No competing financial interests exist.