
Abstract
Modern medical practice has become extremely dependent upon diagnostic imaging technologies to confirm the results of clinical examination and to guide the response to therapies. Of the various diagnostic imaging techniques, ultrasound is the most portable modality and one that is repeatable, dynamic, relatively cheap, and safe as long as the imaging provided is accurately interpreted. It is, however, the most user-dependent, a characteristic that has prompted the development of remote guidance techniques, wherein remote experts guide distant users through the use of information technologies. Medical mission work often brings specialist physicians to less developed locations, where they wish to provide the highest levels of care but are often bereft of diagnostic imaging resources on which they depend. Furthermore, if these personnel become ill or injured, their own care received may not be to the standard they have left at home. We herein report the utilization of a compact hand-carried remote tele-ultrasound system that allowed real-time diagnosis and follow-up of an acutely torn adductor muscle by a team of ultrasonographers, surgeons, and physicians. The patient was one of the mission surgeons who was guided to self-image. The virtual network of supporting experts was located across North America, whereas the patient was in Lome, Togo, West Africa. The system consisted of a hand-carried ultrasound, the output of which was digitized and streamed to the experts within standard voice-over-Internet-protocol software with an embedded simultaneous videocamera image of the ultrasonographer's hands using a customized graphical user interface. The practical concept of a virtual tele-ultrasound support network was illustrated through the clinical guidance of multiple physicians, including National Aeronautics and Space Administration Medical Operations remote guiders, Olympic team-associated surgeons, and ultrasound-focused emergentologists.
Introduction
Ultrasound is a versatile diagnostic tool that can be applied to nearly every clinical interaction by bringing an additional clinical sense to the bedside. An ever-increasing clinical utility coupled with dramatic decreases in costs and technical improvements means that the modality of ultrasound may be available almost anywhere on and even off the planet. 1,2 This potential utility has long been appreciated by the World Health Organization (WHO). The WHO considers ultrasound one of the most important technologies needed by developing countries, 3 rating access to general-purpose ultrasonography as a minimum global standard. 4 However, this potential benefit to patients may be compromised or even negated either if the images are not generated and pathology is missed, if they are misinterpreted and misdiagnoses are made, or if inappropriate interventions are undertaken by inexperienced ultrasound users. The National Aeronautics and Space Administration (NASA) has addressed the issue of inexperienced (typically non-physician) care providers using ultrasound by championing real-time remote mentoring by distant experts using the Internet and advanced communication technologies. 5 –7 Initial efforts have also begun to extend the utility of this paradigm to benefit terrestrial care, 8 including actual clinical practice. 9 Furthermore, the requisites for such tele-ultrasound consultations are becoming simpler and more portable, 10 to the point where a hand-carried portable tele-ultrasound system (PTUS) was constructed suitable for self-transport on-board commercial airliners to an overseas medical mission.
We herein report what we believe to be the first trans-oceanic description of a PTUS used to enable self-conducted examination with assistance of a virtual network of remote experts who thereafter collaborated to diagnose, recommend treatment, and ultimately follow up the care of an injured surgeon to avoid any interruptions in the medical mission.
Case Report
A previously healthy 48-year-old male surgeon was playing ice hockey 48 h prior to deploying on a medical mercy mission to West Africa. He had inadequately warmed up prior to engaging in play. Coincident with an elegant but aggressive “cut” to bypass an opposing player, there was an audible “pop,” and he was immediately incapacitated with pain and swelling to the left groin and proximal medial thigh. He applied ice and self-medicated with nonsteroidal anti-inflammatory agents, but otherwise practical logistical preparations for the mission and professional obligations precluded seeking medical advice prior to traveling to Lome, Togo, 11,183 km distant. The early physical findings consisted of a boggy, swollen medial thigh with subcutaneous hematoma extending throughout the medial thigh from groin to knee (Fig. 1). Even when painfully limping, however, the surgeon was able to transport a PTUS onboard a series of commercial airliners in his hand-carried cabin luggage, which consisted of freely downloadable software (Skype™ [Microsoft, Redmond, WA] and XSplit Broadcaster [SplitMediaLabs Ltd., Hong Kong, China]) installed on a Hewlett-Packard (Mississauga, ON, Canada) ProBook 4520s laptop computer, an analog-to-digital converter (LinXcel VC-211V; ActionStar™, Hsichih City, Taiwan), a compact ultrasound machine (NanoMaxx®; Sonosite, Bothell, WA), and a head-mounted Webcam (LifeCam VX-2000; Microsoft) (Fig. 2). The PTUS “passed” preboarding security screening in the Calgary (AB, Canada), Montreal (QC, Canada), Brussels (Belgium), Lome, and Frankfurt (Germany) airport. Both the images from the head-mounted Webcam and the ultrasound were input into the XSplit Broadcaster, which created a graphic user display, which was thereafter selected as the video source for Skype and which could thereafter be “shared: with any other securely identified Skype user. In this manner, any mentor worldwide could communicate verbally, view the ultrasound images, and guide the remote user's hands and probe movements to examine the distant patient, as long as both parties obtained “connectivity” to the Internet. Excellent connectivity of the system was demonstrated between the departures lounge of Dorval Airport (Montreal) and a hospital in Calgary, using standard publicly available Internet services.

Subcutaneous swelling and hematoma extending throughout the medial thigh within the first week after injury and travel to West Africa.

Portable tele-ultrasound system deployed on the top deck of a medical mission ship (MV African Mercy) in Togo, West Africa.
The first clinical deployment of the system was attempted within 48 h after arrival in Africa. The authors were able to obtain connectivity between West Africa and Calgary when the system was deployed on the top deck of a medical mission ship, the MV Africa Mercy (Fig. 2). As the connectivity was obtained by tethering the whole system through an iPhone® (Apple, Cupertino, CA), 10 the costs of obtaining even brief Internet services was prohibitive for a detailed examination. Furthermore, the information technology utilization policy of the Africa Mercy prohibited using the ship's internal information technology resources for this purpose.
Therefore, subsequent teleconsultations were conducted from a local hotel in Lome, where Internet connectivity was obtained by purchasing a pass to the hotel-lobby wireless access point (Supplementary Fig. S1; Supplementary Data are available online at

Screen capture of the surgeon in West Africa's computer demonstrating the images being transmitted to the experts in Calgary and Georgia, demonstrating a large perimuscular hematoma.
A rehabilitative regimen consisting of ice, nonsteroidal anti-inflammatory agents, and gentle stretching was instituted that did not conflict with daily operative duties. After 2 weeks of this regimen, the pain, swelling, and functional limitation gradually ameliorated, raising the question of a return to partial exercise. A repeat teleconsultation was arranged with another ad hoc clinical teleconsultative network consisting of the original surgeon in Calgary and the emergentologist in Georgia, with the added expertise of a remote guider in Houston, TX, who had extensive experience both in musculoskeletal sonography and in remote ultrasound mentoring for NASA. Each of the remote experts conducted a diagnostic session with the mission-surgeon and captured both still images and video clips representative of the examination. Each examiner verbally guided the mission-surgeon to image his own leg to their individual satisfaction. They each then prepared summary images and discussed the findings over e-mail. The consensus opinion was of partial healing (Fig. 4), and the virtual committee thus recommended a controlled return to further physical activities. A final imaging session with the Houston-based expert was conducted after the surgeon's return to Canada. This examination suggested continued resolution of the hematoma in the medial adductor compartment (Fig. 5), which was thereafter corroborated by a magnetic resonance imaging scan 8 weeks post-injury (Fig. 6).
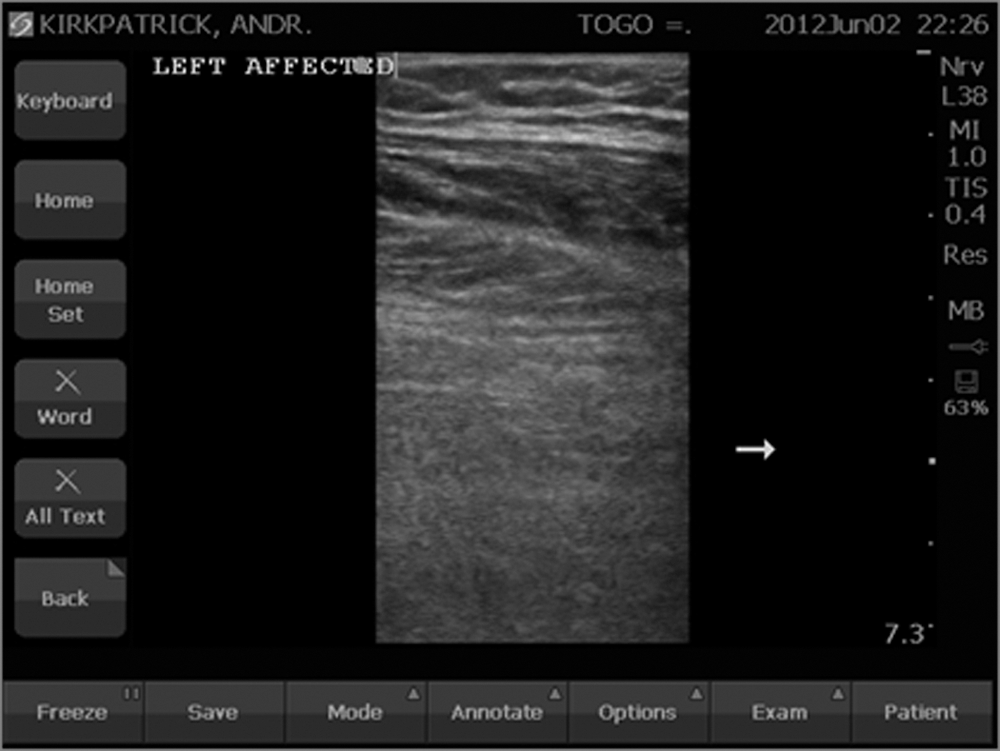
Image of the greatly resolved perimuscular hematoma 4 weeks after the original injury as viewed by remote mentors in North America.

Remote image obtained with remote guidance from Houston, TX, of a patient after the return to Calgary revealing residual hematoma related to a combined avulsion injury of the adductor brevis and longus muscles 7 weeks post-injury.

Coronal T2 and axial proton density large field-of-view magnetic resonance images 8 weeks post-injury demonstrate a complete tear of the left adductor longus origin at the pubic tubercle. The tendon stump is distally retracted 2.5 cm, and there is an accompanying fluid-filled defect of the tendon. The right adductor longus tendon origin is normal for comparison.
Discussion
The PTUS proved an effective tool to access a worldwide virtual network of clinical and imaging specialists to remotely diagnose and manage a disabling injury with the potential for not only personal disability in the patient, but also disruption of a humanitarian mission. Key elements in providing this overall capability can be conceptualized as being (1) the PTUS technical components, (2) Internet connectivity, and (3) the virtual network of mentoring clinical experts with advanced knowledge of ultrasound imaging.
The PTUS, which has been previously described, 8,11 comprised relatively low-cost components and freely available “shareware”-type software, with the main system cost being the ultrasound, which itself is becoming cheaper every year. A complementary embedded video image of the probe placement area was felt to be very valuable by the emergentologist, as this permitted advanced manipulations to be conducted such as augmenting venous return through calf compression to increase the venous Doppler signal. This is similar to the current NASA system, in which the cabin video of the International Space Station shows the subject's image with ultrasound probe movements and position.
Internet connectivity was obtained either using the integrated wireless receiver on the laptop computer or through tethering the computer through a smartphone on a 3G network. The WHO has considered access to the Internet as a basic human right. 12,13 Accordingly, as the planet increasingly connects, caregivers almost anywhere will be able to communicate and professionally support each other.
The quality of the live ultrasound image at the receiving sites varied within the “acceptable” to “good” range. No spurious “noise” or image distortions were noted. Spatial, temporal, and grayscale resolutions were assessed subjectively by all remote experts. Spatial resolution was initially assessed by the ability of the receiving expert to discern the characters of metadata, specifically, the values of mechanical index and thermal index on the ultrasound screen. This was considered important also in terms of the suitability of the PTUS for applications such as obstetric or ophthalmic imaging. The other spatial resolution criteria included sharpness of vascular cross-sections, fascial borders, and bone surfaces. Grayscale resolution, although clearly inferior to the original image displayed on the ultrasound system's screen, was found acceptable with a moderate reduction in the number of levels of “gray”; all experts agreed that the dynamic range of the overall system was still largely preserved. The temporal resolution (frame rate, or “refresh rate”) of the live ultrasound image was also variable but mostly sufficient to be perceived as “full motion” (i.e., above approximately 15 frames/s). Occasional slowing of the frame rate to 4–5 frames/s did not present a serious problem. Because of automatic software and possibly firmware adaptation to the actual bandwidth, all aspects of image quality were felt to change concordantly (i.e., better spatial resolution coincided with a smoother grayscale pattern).
Upon initiation of the call through the Skype service, a certain level of quality was automatically selected based on the instantaneous bandwidth and then retained throughout the session. In two occasions, call re-initiation resulted in substantially higher quality of image transmission. Subsequent degradation, if it happened, was thought to affect the temporal resolution before affecting the spatial and grayscale quality. The experts did not require full-resolution images to be saved locally and transmitted by e-mail (either during or after examinations), although such capability was available. Thus, the live nature of real-time ultrasound imaging with rapid succession of images was able to compensate for the relative degradation of image quality of individual frames.
Finally, the virtual network of experts was a critical component that has only rarely been discussed. 14 This network was fluid, as the composition changed with availability between the initial and follow-up examinations, but was therefore flexible with the emphasis being on the acute diagnosis in the initial consultation with the senior physician being an emergentologist and emergency medicine ultrasound fellowship director with extensive clinical experience, whereas the follow-up examination was led by a radiologist with extensive experience mentoring NASA astronauts. These team members were only representative, however, of a broader membership that could be increased at will depending on the particular clinical problem being addressed.
The human resource question has typically been the “Achilles' heel” of most telemedicine projects, as it was in the first real-time use of acute tele-ultrasound in trauma care that used a fixed base station requiring a physical presence of the remote expert. 9 Such virtual networks could presumably provide care to any site with connectivity allowing a single “on-call” group of any agreeable experts on any subject to connect to a provider–patient combination in need. Like so much in contemporary medicine, these virtual networks are technologically ready for prime time, yet the administrative, political, and legislational frameworks within which they would need to function on a national or even international basis are lacking. Although we, and likely others, have submitted granting requests, government or industry commitments to pursue these endeavors have not been obtained at present. Thus, although formalizing dependable mentoring networks with robust and immediate 24/7 mentoring remains a vision, the approach is a reality and can be used by any entity that has the desire and commitment to do so. In this case the remote experts voluntarily consulted with the mission-surgeon using freely available software to permit group consultations (saving time), to maximize efficiency, and to increase diagnostic accuracy. Thus, given concerns regarding lower standards in international surgical outreach missions, 15 the PTUS addressed these concerns, 16 being one example among countless other potential applications.
In summary, with easily available technologies, experts can easily support point-of-care clinical ultrasound, even self-performed, anywhere in the known universe where Internet from the planet Earth can be accessed. The usefulness of this resource is only limited by the ever-increasing scope of ultrasound-assisted diagnosis and therapy and the robustness and organization of the virtual networks of experts supporting the point of care.
Footnotes
Acknowledgments
We thank Dr. Bevan Frizzel, Department of Radiology, Foothills Medical Centre, Calgary, AB, Canada, for imaging support and Michelle Mercado and Alma Rados, Regional Trauma Services, Calgary, for Internet hosting. The Sonosite Corporation donated the unrestricted use of a NanoMaxx ultrasound machine to conduct this study.
Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.