
Abstract
Introduction
Chronic heart failure (CHF) represents a major public health problem in Western countries and, despite new and more effective treatments, is associated with poor life expectancy, impaired quality of life (QoL) and repeated hospitalizations. 1,2
In Italy, in the last 10 years hospitalizations related to CHF have increased by 21%, and in 2009, diagnosis-related group (DRG) 127 (heart failure [HF] and shock) was the first reason for hospital admission after vaginal delivery (DRG 373), with more than 1,800,000 hospital days. 3 In recent years, increases in healthcare costs, mainly due to in-hospital treatment, have highlighted the need for exploring new management strategies for these patients. The weight of evidence from meta-analysis of randomized trials showed that multidisciplinary nonpharmacological approaches resulted in prolonged survival and reduced readmissions. 4 Thus, these care strategies have been incorporated into the guidelines for the management of HF syndrome. 5,6 In the last 10 years, remote monitoring (structured telephone support or telemonitoring) has been widely explored as adjunctive components of CHF management strategies. 7 Up to now, the efficacy of such models on mortality and hospital readmissions is still unclear, and trials reporting their effects on surrogate end points such as left ventricular function, physical performance, and QoL are lacking.
In Italy, a home-based program including a multidisciplinary management and remote telemonitoring for patients with CHF was introduced as an experimental model by the Institute of Care and Scientific Research, Salvatore Maugeri Foundation, Lumezzane, Italy, in 2000. In a national multicenter randomized study, supported by the National Ministry of Health, we demonstrated that this program is useful in reducing hospital readmissions and related costs.
8
Based on these preliminary results, the model was improved and extensively tested in the Lombardy region in the following years. In 2006, the home-based telesurveillance program (HTP) was formally adopted as part of the services delivered by the regional healthcare system within a project called “Nuove Reti Sanitarie” with a specific experimental reimbursement (
This article is focused on the following research questions: • What is the effect of the HTP on the functional status, physical performance, and health-related QoL? • What patient characteristics are associated with a positive response to the program? • What is the effect of the HTP on readmission and mortality at 1 year?
Materials and Methods
HTP
Clinical protocol
Patients of both genders, living in the Lombardy region, with confirmed diagnosis of CHF, older than 18 years, and with at least one hospitalization for acute HF in the previous 6 months could be enrolled in the HTP. Exclusion criteria included the presence of unstable angina, non-cardiac debilitating illness with inauspicious prognosis, clinically evident cognitive impairment, planned surgical procedures (coronary revascularization, valve surgery, heart transplant), participation to other studies, and in-hospital patients. Access to the HTP could be suggested by the attending cardiologist or the family physician at the time of hospital discharge or after a visit at the outpatient clinic. Before enrollment, all patients were clinically stable and trained about CHF, including advice on self-measurement of weight and blood pressure, dietary restrictions (including sodium and fluid), and signs and symptoms of HF exacerbation.
At the beginning and the end of the HTP, patients underwent in-hospital physical examination, two-dimensional echocardiography, and the 6-min walking distance (6MWD) test. 9 A complete medical history and symptomatic status related to CHF, New York Heart Association (NYHA) class, vital signs, and concomitant treatments were also collected. QoL was assessed by the Minnesota Living with Heart Failure Questionnaire (MLHFQ). 10
All patients and their general practitioner signed the informed consent form.
Program design
The HTP was organized as a multidisciplinary care approach functioning through structured telephone support and telemonitoring. An intensive nurse care management program was created, and a nurse-tutor followed up the enrolled patients for 6 months. Nurse-tutors performed a weekly intervention mainly through structured appointments (from Monday to Friday from 8:30 a.m. to 4:00 p.m.), collecting information about disease status (blood pressure and body weight measurements) and symptoms (general information). Patients were provided with a portable one-lead electrocardiograph (Card Guard® 2206; Card Guard Scientific Survival Ltd., Rehovot, Israel) and instructed how to transmit the electrocardiogram trace via a fixed or mobile telephone line to the nurse-tutor.
Participants in the study were also informed that telesupport, aside from the normal weekly nurse call, could be reached by the patients themselves for urgent conditions and emergencies. Unscheduled contacts could also be activated 24 h/day 365 days a year and would be with the nurse on duty in case of symptoms, signs of possible decompensation, or any doubt about therapy. Moreover, the electrocardiogram trace was transferred during each call to the telemedicine center, which stored and sent it to the hospital unit (Fig. 1). At the end of each phone call, the nurse-tutor may provide support to the patients, offer advice regarding diet, lifestyle, and medications, suggest changes in therapy within patient-adapted criteria previously defined with the cardiologist supervising the program, require consultation with a cardiologist, and schedule the next phone appointment. All conversations were recorded; electrocardiogram tracings, patient's clinical data, and suggestions were filled into a personal health electronic record by the nurse-tutor.
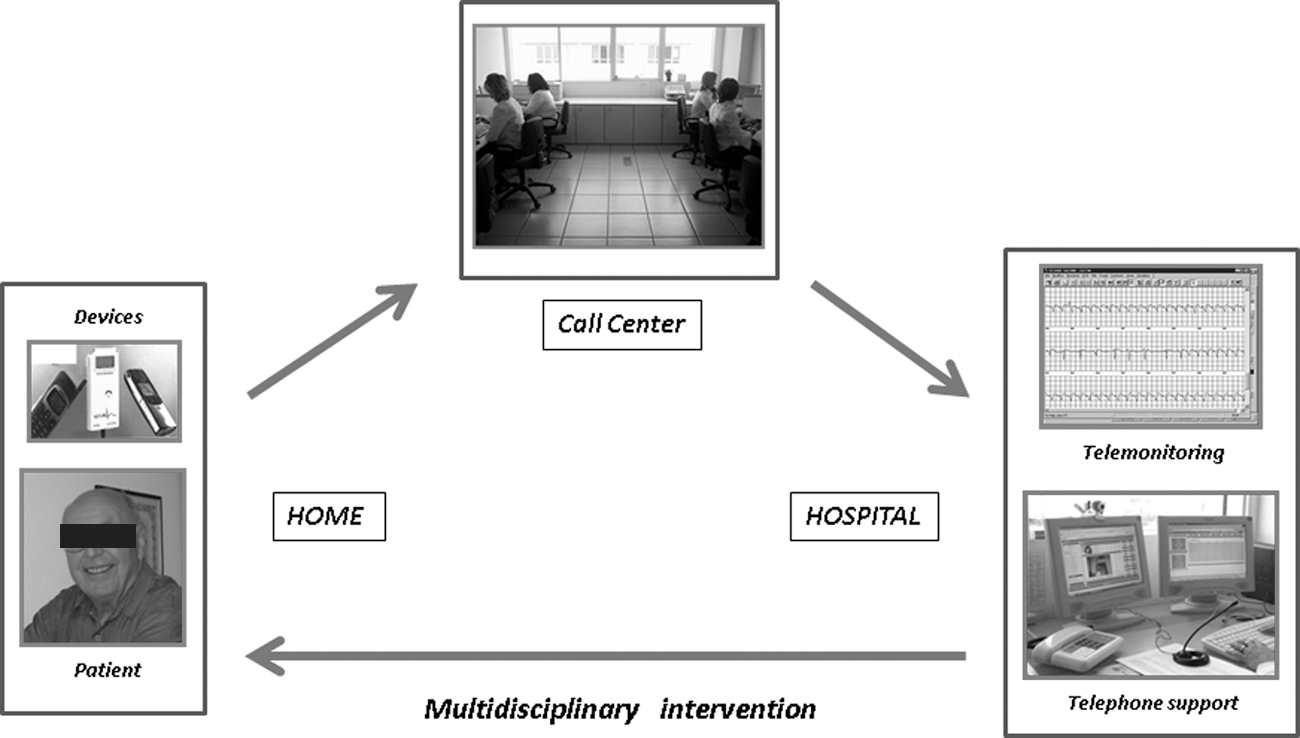
Scheme of the relevant level of integration between technology and medical staff within the home-based program.
Medical doctors (cardiologist and/or general practitioner) were consulted before referring the patient to the emergency department or to the HF clinic.
Education of the staff/operators
A comprehensive training program was developed and presented to the clinical staff (physicians and registered nurses) of the various hospitals. Education was provided in different sessions on the following topics: chronic disease management for HF, medication management, use of the standard HF care plan, explanation of how to use patient education material, and telemonitoring integration. Nurses received additional training as far as filling out of the patient's personal health record, use of the telemedicine equipment, and interpretation of the patient's vital sign data trend.
Telemedical centers
Three telemedical centers offered technological support, biomedical devices, and a call center for telemonitoring activities, managed the database of collected data, and provided clinical and nursing activities during the night and weekends through its health personnel, therefore guaranteeing the 24 h/day service.
Patient Sample and Data Extraction
All of the patients registered in the regional telemedicine database and who had completed at least 1 year of follow-up after the end of the program on December 31, 2009 were identified. Administrative and medical data were retrieved and organized in a single database for the current analysis. Privacy of patient data was ensured using dynamic encryption of the fiscal code. Moreover, all hospital records of these patients were retrieved from the regional administrative database and linked to the telemedicine records. Only hospital records referring to Major Diagnostic Categories 5 (diseases and disorders of the circulatory system) and unplanned hospital admission were considered for the analysis.
Data obtained from the regional administrative patients' records included data of hospital admission, length of stay, primary and secondary diagnosis or complication, medical or surgical procedures, DRG classifications, ward of hospitalization, planned/unplanned admission, and status at discharge (alive/death). HF index hospitalization was defined as the closest to beginning of the program. Moreover, all patient refined-DRG (APR-DRG) severity of illness and risk of mortality scores were calculated for each HF index hospitalization using APR-DRG Expert software (releases 24.0 and 25.0; 3M™ Health Information Systems, St. Paul, MN).
Causes of readmission were derived from the regional administrative database. The principal diagnosis of each hospitalization was assessed using International Classification of Disease, 9th revision (ICD-9). Secondary ICD-9 codes were not examined as there is discretion in their number and order.
Information regarding death was obtained by hospital records.
Data retrieved from each patient's telemedicine records included age, gender, comorbidities, CHF etiology, number of hospitalizations in the previous 6 months, cardiac devices, NYHA class, left ventricular ejection fraction (LVEF), main laboratory data, 6MWD, MLHFQ total score, and prescribed medications. Patients taking the combination of angiotensin converting enzyme inhibitors/angiotensin receptor blockers, β-blockers, and diuretics were considered optimally treated.
Primary outcome measurements included changes in functional status (NYHA class, LVEF), physical performance (6MWD), and health-related QoL (MLHFQ total score). Secondary outcome was a composite of unplanned cardiovascular readmission or cardiac hospital mortality within 1 year from the end of the program.
Statistics
Effect on primary outcomes
The changes in the primary outcomes (i.e., functional status [NYHA class], physical performance [6MWD], and health-related QoL [MLHFQ]) from baseline to the end of the program were assessed using a two-tailed Student's t test for paired data (continuous variables) or chi-squared test (categorical variables). The associations between continuous variables were tested using Pearson's correlation coefficient and between categorical and continuous variables by analysis of variance. Variables showing significant relationships were then entered into a stepwise multiple regression considering changes in the outcome variable as the dependent variable.
Responders versus non-responders
A reduction in NYHA class was considered as a favorable result. Changes in LVEF, 6MWD, and MLHFQ total score were categorized according to their quartile distribution, and changes ranging from the median to the maximum were considered clinically significant. Patients who showed a clinically significant improvement in at least two of the primary outcome measurements (including NYHA class) were considered to be responders.
The differences between responders and non-responders were analyzed by chi-squared test for discrete variables, by Student's t test for normally distributed continuous variables, and by Mann–Whitney test for non-normally distributed continuous variables. Predictors of responsiveness to HTP were tested using binary logistic regression analysis.
Effect on 1-year outcomes
Comparison of baseline variables and secondary end-point data included chi-squared analysis, with calculation of odds ratio and 95% confidence intervals. A Kaplan–Meier time-to-event function for readmission or death was constructed, and the log-rank test was used to test the differences in the number or timing of secondary outcome between responders and non-responders. Data for all surviving patients were censored on December 31, 2009. The independent effect of all variables (measured at the entry and the end of the program) on event-free readmission or death was assessed by a Cox proportional hazard model (with initial entry and stepwise rejection of variables at 0.1 and 0.05 levels of significance, respectively).
All analyses were performed using SAS software (version 9.2; SAS Institute, Cary, NC), and values of p≤0.05 were considered statistically significant. Data are expressed as mean±standard deviation values or proportions.
Results
Patient Population
Among 1,196 patients registered in the regional telemedicine database as of December 31, 2008, 773 completed 1 year of follow-up after the end of the program. Of these, 602 concluded the HTP regularly without hospitalizations and were considered for the analyses. The baseline characteristics of this population are shown in Table 1. The majority of patients were males, were >65 years of age (69%), and had severe left ventricular systolic dysfunction (70% with LVEF ≤35%) and advanced functional limitation, with 86% being in NYHA functional class III–IV. Coronary artery disease was the most common cause of HF, and multiple comorbidities (two or more) were present in 27.5% of patients. Combined pharmacotherapy (diuretics+angiotensin converting enzyme inhibitors/angiotensin receptor blockers+β-blockers) was prescribed in 35% of the patients. Ninety-four patients (15.6%) had a severity of illness score of ≥2 (major or severe), and 37 (6.1%) were classified at higher risk of death (risk of mortality score of ≥2).
Characteristics of the Patient Population
6MWD, 6-minute walking distance; ACE, angiotensin converting enzyme; AF, atrial fibrillation; APR-DRG, all patient refined-diagnosis-related group; ARB, angiotensin receptor blocker; HF, heart failure; ICD, implantable cardioverter defibrillator; LVEF, left ventricular ejection fraction; MLHFQ, Minnesota Living with Heart Failure Questionnaire; NYHA, New York Heart Association; QoL, quality of life; ROM, risk of mortality; SOI, severity of illness.
Telesurveillance Program
The activities provided during the program are presented in Table 2. The median interval between index hospital discharge and enrollment was 17 days (range, 4–48 days). Of the patients, 89.8% received at least one phone contact per week according to the clinical protocol.
Activities Provided During the Program
CI, confidence intervals; EKG, electrocardiogram; n, number.
Effect on Primary Outcomes
At the end of the program, NYHA class, LVEF, 6MWD, and MLHFQ total score improved significantly (Table 3). The changes in NYHA class were weakly correlated with changes in LVEF (r=0.16, p<0.001) and MLHFQ score (r=0.22, p<0.0001). NYHA improved in 212 patients. Clinically significant changes, as previously defined, in LVEF (>5%), 6MWD (>30 m), and MLHFQ score (reduction of >24 points) occurred in 219, 289, and 264 patients, respectively. Patients taking β-blockers and combined pharmacotherapy increased by 7.6% and 4.2%, respectively.
Primary Outcomes
6MWD, 6-minute walking distance; LVEF, left ventricular ejection fraction; MLHFQ, Minnesota Living with Heart Failure Questionnaire; NYHA, New York Heart Association.
At multiple regression analysis (Table 4), the changes in NYHA class, age, male gender, and advanced NYHA at the entry were significantly associated with improvement. Changes in LVEF were inversely associated with its baseline value and age. Improvement in 6MWD was associated with age, β-blockers prescription, and lower 6MWD at baseline. Finally, changes in MLHFQ total score were inversely associated with the time elapsed between index hospital discharge and enrollment and baseline MLHFQ score values.
Multiple Regression Analysis
6MWD, 6-minute walking distance; LVEF, left ventricular ejection fraction; MLHFQ, Minnesota Living with Heart Failure Questionnaire; NYHA, New York Heart Association.
Responders Versus Non-Responders
Three hundred eight patients (51%) showed a clinically significant improvement in at least two primary outcome variables and were then classified as responders. Comparisons of baseline data between responders and non-responders are reported in Table 5.
Comparisons of Baseline Data Between Responders Versus Non-responders
6MWD, 6-minute walking distance; APR-DRG, all patient refined-diagnosis-related group; HF, heart failure; ICD, implantable cardioverter defibrillator; LVEF, left ventricular ejection fraction; MLHFQ, Minnesota Living with Heart Failure Questionnaire; NS, not signficant; NYHA, New York Heart Association; ROM, risk of mortality; SOI, severity of illness.
The variables independently associated (logistic regression analysis) with a favorable response to the program are reported in Table 6. The percentage of cases correctly classified by the logistic equation was 72.4% (sensitivity, 65%; specificity, 72%).
Logistic Regression Analysis
6MWD, 6-minute walking distance; LVEF, left ventricular ejection fraction; MLHFQ, Minnesota Living with Heart Failure Questionnaire; NYHA, New York Heart Association; SOI, severity of illness.
Effect on 1-Year Outcomes
During 365 days of follow-up after the end of the program, clinical events (hospital readmissions or death) occurred in 120 patients: 71 (24.1%) in non-responders and 49 (15.9%) in responders (odds ratio 1.52; 95% confidence interval 1.02, 2.26; p=0.03). Figure 2 shows the event-free survival curves for both groups. Acute HF was the main cause of hospitalization in both groups (63.2% in responders versus 64.8% in non-responders), but the readmission rate (15.6% versus 9.4%; odds ratio 1.66; 95% confidence interval 1.01, 2.71; p=0.04) and the total number of readmissions (58 versus 31; p<0.01) were significantly higher in the latter group. Unresponsiveness to HTP, the presence of an implantable cardioverter defibrillator, and multiple (two or more) non-cardiovascular comorbidities were independently associated with the risk of cardiovascular readmissions or death (Fig. 2).

Cumulative probability of event-free survival during 1 year of follow-up. Relative risk (RR) with 95% confidence intervals is given for independent predictors. Level of significance: *p<0.04, **p<0.01. ICD, implantable cardioverter defibrillator.
Discussion
Disease management programs are now considered standard interventions within the multidisciplinary model of HF management. 5 Modern telecommunication technologies offer new options to deliver remote specialized healthcare, and in the last decade several randomized controlled studies focusing on the effects of various telemanagement programs for CHF have been published. A recent Cochrane Collaboration review and meta-analysis 7 found that such programs have a broad range of benefits and that both structured telephone support and telemonitoring interventions show similar benefits on HF-related hospitalizations. Moreover, all published trials have been powered to highlight the effectiveness in hard end points as mortality and cardiovascular hospitalizations; consequently, information on the efficacy of such programs on surrogate outcomes such as functional class, physical performance, and QoL are lacking. In Italy, the telemedicine database of “Nuove Reti Sanitarie” contains a larger national experience on HTP in CHF patients and offers the opportunity to investigate the efficacy of the model on these variables, as they were systematically collected according to the study design. Moreover, the linkage between telemedicine and regional hospitalization databases performed in this study has never been used in published studies and represents a reliable method to investigate the relationship between hard outcomes (death, hospitalization).
Few articles have reported the effects of telemanagement programs on the outcomes considered in the present study. Among 25 studies published as full peer-reviewed publications included in the meta-analysis by Inglis et al., 7 the effects of both telephone support and telemonitoring programs on functional class were examined in 4 studies, MLHFQ in 10 studies, 6MWD in 2 studies, and LVEF in only 1 study. NYHA class improved in 3 out of 4 studies, MLHFQ in 6 out of 10 studies, and 6MWD increased in 1 out of 2 studies, whereas no effect on LVEF was reported.
In the current study, we documented a significant improvement in all these outcomes. Although we cannot exclude a spontaneous variation of the outcomes as a consequence of the natural history of the disease, optimization of pharmacotherapy carried out during the program, confirmed by the increase in the number of patients taking β-blockers or combined therapy (diuretics+angiotensin converting enzyme inhibitors/angiotensin receptor blockers+β-blockers), and reinforcement/education of patients on adherence to the therapy during nurse-tutor calls could have played a significant role. In fact, therapy adjustments occurred at least four times during the 6 months of the program in the vast majority of the patients. By multivariate analysis, independent predictors of favorable response for the analyzed clinical outcomes included APR-DRG severity of illness score of ≥2, medical therapy at entry (β-blockers, aldosterone blockers), and more compromised baseline values of each primary outcome.
Because the changes in outcome measures were poorly related one to each other, we considered them as independent variables. Moreover, favorable responses in terms of changes in LVEF, 6MWD, and QoL were defined using cutoff values based on the sample distribution, and we decided to classify as responders patients who improved in at least two of the primary outcome measurements. Although arbitrary, these criteria appear to be acceptable for many reasons. First, an increase of 5% in LVEF is generally considered clinically relevant as predictive of better prognosis. 11 Second, a change of 30 m in the 6MWD corresponds to the value considered clinically significant by Guyatt et al. 12 and takes into account the reproducibility of the test. 13 Third, the cutoff value of MLHFQ changes adopted in the present study is higher than that considered significant (−5 points) by Rector et al. 14 and superior to the spontaneous improvement of the QoL scores that is usually observed over time after hospital discharge. 15
Finally, the definition of responders, combining more than a single outcome, seems more suitable for describing the overall effectiveness of the program in the light of the poor correlations between each of the other outcome measures. To date, the long-term implications of the telemedical management programs on the clinical course in CHF patients have been explored in one study only. Ferrante et al. 16 reported that the clinical benefits observed during the telephone intervention program persisted and were sustained after the intervention ended: after 1 year, a 19% reduction in the incidence of the primary end point (HF hospitalization or death) in the intervention group compared with the control group was reported. The present study is not comparable with the above-mentioned trial both for heterogeneity between patients' populations recruited and for features of the intervention. However, the 1-year event rate reported in the present study (19.9%) was quite similar to that observed in the treatment arm of the DIAL trial (14.8%), taking into account that we included as the end-point measure all cardiovascular (not only HF) hospitalizations.
Moreover, the favorable response to the program was independently associated with 32% reduced risk of clinical events during the 1-year follow-up (p<0.001), whereas an implantable cardioverter defibrillator and the presence of multiple comorbidities were associated with increased risk (Fig. 2). These findings could suggest the possibility to identify, at the end of the program, a subgroup of patients at higher risk who could require a closer and maybe more prolonged intervention.
Study Limitations
The major strengths of this study are the large number of the patient cohort, the uniform intervention protocol adopted, and the collection of hard end-point data directly from the regional healthcare system database. Weaknesses are the observational nature of the study, the arbitrary criteria used to define clinically significant changes in outcome variables, and the definition of responders and non-responders. Nevertheless, the restrictive criteria we adopted to define a favorable response to the program and its prognostic significance support the reliability of the results.
Finally, it must be emphasized that, because of the period of enrollment (2006–2008), the results of the present study could not be generalized to contemporary CHF patients and refer to a selected CHF population able to conclude the 6-month protocol without clinical events.
Despite these limitations, the consistency of the results across multiple institutions, together with previous considerations, again supports the strength of overall results.
Conclusions
In summary, the experience of HTP for HF patients in the Lombardy region of Italy shows that (1) the program is effective in improving patients' functional status and QoL, (2) the overall favorable results are more striking in patients who were more compromised at baseline, and (3) an unfavorable response to the program seems to be an independent marker of poor prognosis.
The assessment results described in the present study have had some practical consequences on the regional protocol. Indeed, in the year 2010 the regional HTP protocol was modified, allowing prolonging by a further 6 months the intervention in non-responder patients. Moreover, further analyses on integrated databases (administrative and telemedicine) have been planned to define the cost-effectiveness of the program in order to support the transfer of the HTP by the Healthcare Directorate-General of the Lombardy region into a routine clinical practice.
Footnotes
Acknowledgments
The authors would like to thank the Healthcare Directorate, Lombardy Region, Italy, and the health professionals of all hospitals involved in “Nuove Reti Sanitarie.” The authors are also indebted to Dr. Laura Comini and Mrs. Silvia Brognoli for technical assistance.
Disclosure Statement
No competing financial interests exist.