
Abstract
Introduction
Remote areas throughout the United States are at an increased need for improved access to dermatological care. California's Central Valley, located approximately 100 miles northeast of San Francisco, is a prime example of a populous community with a relatively robust agricultural economy that lacks timely access to most specialist physicians, in particular, dermatologists (Fig. 1). To address this problem, the Kaiser Permanente (KP) Northern California (KPNC) Region instituted a teledermatology program in the Central Valley in January 2009 to provide primary care physicians (PCPs) with same-day dermatologic consultations using “store-and-forward” technology.

Overview of the Kaiser Permanente Northern California's Service Area including San Francisco (encircled on the left) and the Central Valley (encircled on the right). Licensed from
The literature contains many studies that validate the accuracy and reliability of teledermatology as a diagnostic service. 1 –3 A prospective study by Shapiro et al. 4 showed that both clinic-based dermatologists and teledermatologists recommended biopsy for the same 26 out of 49 patients, which yielded a sensitivity and specificity of 1.00 for the teledermatologist. A review article by Levin and Warshaw 3 reported that teledermatology has demonstrated good performance in terms of diagnostic accuracy and reliability compared with clinic-based consultation. They reported complete agreement in diagnosis between teledermatologists and clinic-based dermatologists to be 41%–94% and partial agreement to be 50%–100%, whereas diagnostic accuracy rates ranged from 30% to 92% for clinic dermatologists and 19% to 95% for teledermatologists.
Teledermatology has been shown to be an accurate and reliable diagnostic tool for skin diseases compared with traditional office visits 5 ; because of this, KP has implemented a teledermatology program in the Central Valley, a remote area where dermatologists are highly in demand and waits for an appointment can be several weeks to months long.
Skin cancer is the most common type of cancer and causes much morbidity and mortality in the general population. It is important for patients to have suspicious skin lesions promptly evaluated and biopsied when appropriate by a physician and for treatment to be rendered in a timely manner. A delay in diagnosis and treatment of skin cancer can lead to greater morbidity and mortality. 6
A study by Hsiao and Oh 7 from the Veterans Administration in San Francisco, CA, investigated the impact of teledermatology on skin cancer diagnosis and treatment in remote areas. This study found that the overall mean time intervals for initial evaluation, biopsy, and surgery were, respectively, 44 days, 19 days, and 21 days shorter for teledermatology than for conventional consultations. This study concluded that the Veterans Administration teledermatology program is comparable if not superior to conventional referrals in remotely located patients in terms of time to initial evaluation and biopsy of skin cancer.
The Veterans Administration study by Hsaio and Oh 7 is encouraging in terms of the utility of teledermatology for the early diagnosis of skin cancer; however, results from the Veterans Administration population may not be generalizable to the broader U.S. adult population with regard to distribution of socioeconomic status, age, gender, and race/ethnicity. Because of these differences, we felt it was important to assess the use of teledermatology in our remote KP patients in the Central Valley of California. Teledermatology programs can aid remote primary care providers in the identification of lesions that are suspicious for skin cancer as well as assist in the triage of these patients to dermatology clinic in a timely manner. 8
We retrospectively compared the time intervals from initial primary care visit to biopsy between traditional clinic referrals and teledermatology referrals.
Subjects and Methods
This study design was reviewed and approved by the Institutional Review Board Committee, KPNC. Waiver of informed consent was obtained because of the nature of the study. Funding for this study was provided by the KPNC Residency Program, Kaiser Foundation Hospitals.
Study Population
KPNC is a large, integrated healthcare delivery system serving more than 3.2 million members in northern California. We selected patients for this study from automated health plan clinical and administrative databases. KPNC maintains electronic databases containing information on patient demographics, membership, inpatient and outpatient visits, and patient referrals, as well as laboratory, pathology, and pharmacy utilization. This study focused only on patients who ultimately received a diagnosis of skin cancer, specifically squamous cell carcinoma (SCC), basal cell carcinoma (BCC), and malignant melanoma (MM). Patients were eligible for this study if their referral to dermatology had been completed using either the traditional e-consult referral system or the new teledermatology program by which patient charts are routed electronically to the teledermatologist.
Referral Types
At KPNC, remote teledermatologists in San Francisco provide services to over 100 PCPs in the KPNC Central Valley Service Area, which includes primary care clinics in Stockton, Modesto, Manteca, and Tracy, CA. KPNC's San Francisco teledermatology program is a tool that allows a PCP to consult a remote dermatologist by transmitting digital images and a short description of a patient's skin lesion and history through KPNC's electronic medical record system (Fig. 2). The teledermatologist is able to view the images and review the PCP's notes in the electronic medical record. The teledermatologist can then provide the PCP with a diagnosis and treatment plan. If the teledermatologist feels that an in-person dermatology appointment is needed, he or she will automatically send a request for an in-person consultation to the local dermatology department, which can include a note on priority scheduling depending on the suspected dermatologic condition.
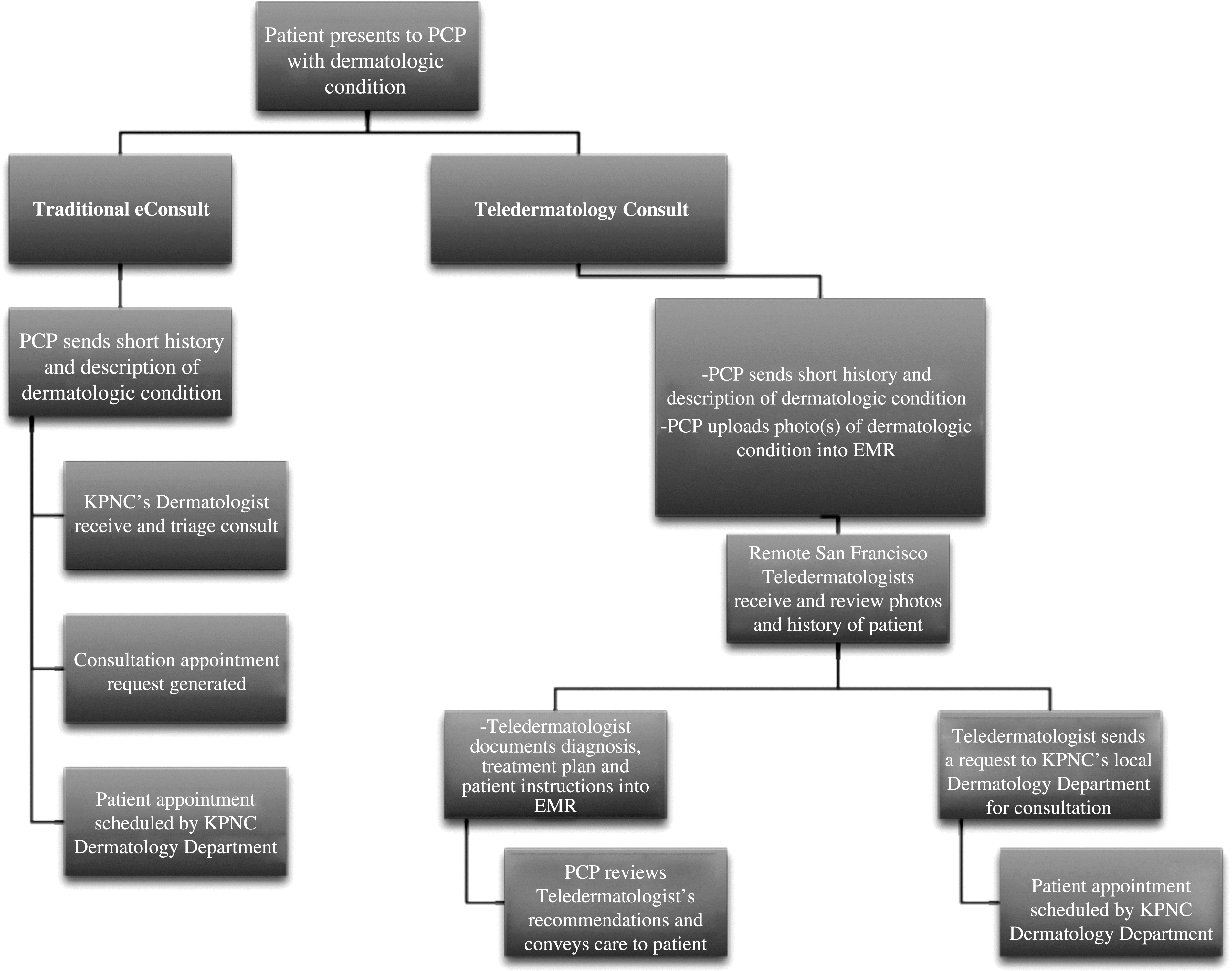
Referral system for traditional e-consults versus teledermatology consults. EMR, electronic medical record; KPNC, Kaiser Permanente Northern California; PCP, primary care physician.
Traditional referrals to dermatology are sent using KPNC's e-consult referral system, which is an automated electronic medical record referral function that asks the PCP to include a short pertinent patient history, exam findings, and reason for referral. No photos are sent through traditional e-consult referrals. In the case of traditional referrals, the dermatologist at KP's Central Valley Dermatology Clinic reviews these referrals and must prioritize these appointments based on the information provided by the PCP. These traditional consults are reviewed daily by the KP Central Valley dermatologists and then scheduled for an in-person appointment by the local staff.
Both traditional e-consults and teledermatology consults are reviewed within 24 h of receipt from the PCP by the appointed local dermatologist or teledermatologist, respectively, and then scheduled via the KP Central Valley's Dermatology Clinic, if an appointment is necessary.
At the time of data collection for this study the teledermatology program was still in the early phases of adoption by the PCPs across KP's Central Valley service area. Therefore, some primary care clinics continued to use the traditional e-consult referral system, whereas others used the same-day teledermatology referral program. The referral method was decided by individual clinics, and an individual PCP used only one method. Patients were not referred based on the PCP's decision between the two referral methods or based on potential severity of their dermatologic problem, but rather by whether that clinic had adopted the teldermatology referral method. This overlap in the use of the two referral systems allowed us to compare them head to head during the same time period.
Data Collection
This was a retrospective observational study using database abstraction and medical record review. Patients referred to the Dermatology Clinic for SCC, BCC, or MM between April 1, 2009 to October 31, 2009 were identified using the pathology diagnosis of skin cancer on the Co-Path database using the respective appropriate Systematized Nomenclature of Medicine (SNOMED) codes for SCC, BCC, and MM. In addition to diagnosis, data collected on these Central Valley skin cancer patients included gender, age at biopsy, ethnicity, KP site, PCP visit date, consult type chosen by PCP (teledermatology versus traditional e-consult), consult date, whether the patient was seen by dermatology, date of biopsy, type of physician performing biopsy (ear/nose/throat versus dermatologist versus general surgeon versus other), and pathology diagnosis.
Statistical Analysis
We performed univariate analyses to report the distribution of skin cancer diagnoses as well as type of consult. We then performed bivariate analyses to assess the association between type of referral and time to biopsy. We also assessed the association between population characteristics and type of referral. Population characteristics assessed were age, gender, skin type (white versus nonwhite), and skin cancer diagnosis. The continuous variables, time to biopsy and age, were not normally distributed; because of this, we used the Wilcoxon–Mann–Whitney nonparametric test to compare time to biopsy and age across the two referral groups. We assessed the association between gender and referral type as well as skin type and referral type using the chi-squared test. For evaluating the association between skin cancer diagnosis and time to biopsy, we chose to report all possible combinations of skin cancer diagnosis; for example, numbers for patients who had BCC only are reported separately from numbers for patients who had both BCC and SCC. We used the chi-squared test to evaluate the association between types of skin cancer and types of referral; however, where cell size was small, we used Fisher's exact test. We performed multivariable analyses assessing time to biopsy by referral type, controlling for patient sex and age at referral, using ordinary least squares regression. A p value of 0.05 was the significance level used for this study. Statistical analyses were performed using SAS version 9.1 software (SAS Institute Inc, Cary, NC).
Results
We identified 382 KP patients using SNOMED codes in our electronic pathology database as having been diagnosed with SCC, BCC, or MM in the California Central Valley between the period of April to October 2009 (Fig. 3). From this group we excluded 21 patients who had been diagnosed with extracutaneous SCC (all BCC and MM cases from our initial query proved to be cutaneous in nature), as the SNOMED codes did not allow us to narrow our query to “cutaneous” SCC, BCC, or MM. For example, our query included patients who had been diagnosed with SCC of the oropharynx or lung. Of these 361 patients, we verified that the SNOMED-derived pathology diagnosis was correct through electronic chart review. Through the chart review, we excluded 66 patients who were already being followed by dermatology, as we felt that this would affect the promptness with which a patient would be seen by their dermatologist. Lastly, we excluded 4 teledermatology consult patients (2 had previously been excluded for already being followed by a dermatologist) who were referred to nondermatologists for biopsy of their suspicious lesions as we were interested in evaluating the time to biopsy a skin cancer in the Dermatology Clinic in KPNC's Central Valley office via the two referral systems; these nondermatologic specialties included general surgery and ear/nose/throat. These 4 patients represented 1.1% (4 of 361 patients) of our total population who were diagnosed with a cutaneous SCC, BCC, or MM. Including these 4 patients in our statistical analysis did not materially change our results, which were still statistically significant with a shorter time to biopsy in the teledermatology group compared with the traditional e-consults.
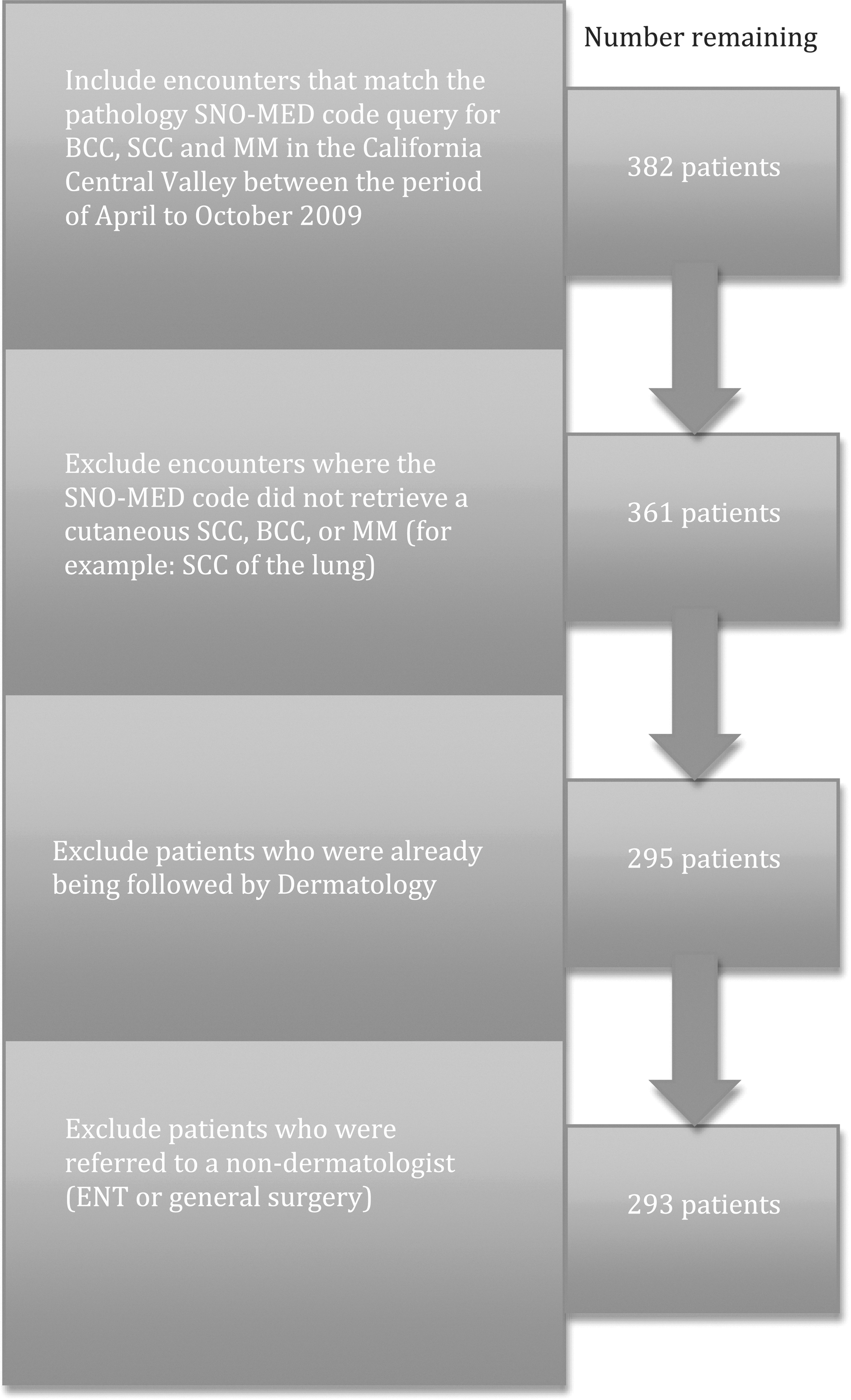
Inclusion and exclusion criteria for encounter selection. BCC, basal cell carcinoma; ENT, ear/nose/throat; MM, malignant melanoma; SCC, squamous cell carcinoma; SNO-MED, Systematized Nomenclature of Medicine.
In total, 293 patient cases met our study criteria; of these, 170 (58%) were conventional referrals, and 123 (42%) were teledermatology referrals.
Results from bivariate analyses comparing population characteristics by consult type are shown in Table 1. We did not detect a significant difference between the e-consult and the teledermatology groups for age at referral, patient sex, skin type, or skin cancer diagnosis. Patients who were referred to the Dermatology Clinic using the teledermatology program (mean of 9.7 days, median of 9 days) had a significantly shorter time to biopsy than patients who were referred through e-consult (mean of 13.8 days, median of 12 days). This difference was statistically significant at p<0.0001.
Population Characteristics by Consult Type
This test was performed using the Wilcoxon–Mann–Whitney nonparametric test.
The chi-squared test was used for this comparison.
Numbers for skin type do not add up to totals for e-consult and teledermatology because race data were available for only 139 (47.4%) of all patient cases in this study.
Fisher's exact test was used for this comparison.
BCC, basal cell carcinoma; IQR, interquartile range; MM, malignant melanoma; SCC, squamous cell carcinoma.
We performed multivariable analyses using ordinary least squares regression (Table 2). Time to biopsy was assessed separately for patients with BCC and patients with SCC. The 22 patients who were eventually diagnosed with both BCC and SCC are represented in results for both BCC and SCC. We did not report multivariable results for patients with MM because of small sample size (n=7) and inadequate power to determine a stable time to biopsy estimate for patients with this type of skin cancer. The association between type of referral and time to biopsy was evaluated controlling for patient sex and patient age at referral. We did not include race in the multivariable analysis because race data were missing for 52.6% of our cohort. Among patients eventually diagnosed with BCC the mean time to biopsy of skin cancer was 13.5 days (95% confidence interval 12–15 days) for conventional referrals versus 10.0 days (95% confidence interval 8.1–11.9 days) for teledermatology referrals (p<0.001). Among patients eventually diagnosed with SCC, the mean time to biopsy of skin cancer was 14.1 days (95% confidence interval 11.3–16.9 days) for conventional referrals versus 8.9 days (95% confidence interval 5.6–12.2 days) for teledermatology referrals (p<0.001). Patient sex and age at referral were not significantly associated with type of referral for patients with BCC or for patients with SCC.
Time to Biopsy Skin Cancer by Referral Type
Some patients had both basal cell carcinoma (BCC) and squamous cell carcinoma (SCC). These patients are reflected in the results for both BCC and SCC.
Ordinary least squares regression. Results are adjusted by patient sex and age at referral. Results were not adjusted by race, as race data were incomplete for this study.
CI, confidence interval; IQR, interquartile range; MM, malignant melanoma.
Discussion
Teledermatology has been validated as an accurate and reliable diagnostic tool for skin diseases compared with traditional office visits. 9 –11 However, there are few studies that have shown that teledermatology has a favorable effect on skin cancer treatment. 8,10,11 The introduction of the teledermatology program in KPNC's Central Valley Service area offered a unique opportunity to compare the outcomes of patients with skin cancer who have been triaged to dermatology with a conventional electronic medical record referral versus teledermatology referral.
We compared the time interval between initial evaluation and biopsy of the most common types of skin cancer for teledermatology versus traditional e-consult referrals from primary care. The time interval from initial dermatology referral to biopsy of skin cancers provides a convenient, yet objective, measure to assess management by two referral types (teledermatology versus e-consult). Our results demonstrate that there is a significantly shorter time interval between initial dermatology consult to time of biopsy of the most common skin cancers for teledermatology consults compared with traditional e-consults from primary care.
Because both traditional e-consults and teledermatology consults are reviewed within 24 h by the appointed dermatologist or teledermatologist, we do not feel that the improved time to biopsy of a common skin cancer demonstrated by teledermatology consults is solely due to the efficiency of the teledermatology program. We feel that the reduced time to biopsy for patients referred through the teledermatology program is due to a more effective triaging mechanism inherent in the structure of the teledermatology program. Although we did not track which traditional e-consult or teledermatology consult was referred to the local dermatologists as a “rule-out skin cancer” case by the reviewing dermatologist or teledermatologist, we believe that triaging of suspected skin cancers by teledermatologists as “rule-out skin cancer” is superior to traditional consults in which the reviewing dermatologist must rely solely on the PCP's history, description, and assessment of the dermatological condition. We chose not to compare the time interval from the biopsy to the date of surgery as we felt the type of initial dermatologic consult would have no influence on this time interval because once a biopsy returns to the dermatologist as skin cancer, the referral for surgery does not take into account initial referral into the Dermatology Clinic (i.e., whether the patient was originally referred as a traditional e-consult or a teledermatology consult). Furthermore, not all diagnosed skin cancers undergo surgery.
In the face of the rising costs of healthcare, teledermatology offers an advantage over traditional consults in avoiding unnecessary dermatology clinic visits. A randomized study by Pak et al. 5 in a Department of Defense setting concluded that store-and-forward teledermatology was a cost-saving strategy compared with conventional consultation methods when productivity loss cost was taken into consideration. In our study, 1% of the teledermatology patients compared with none of the traditional e-consult patients were referred directly into ear/nose/throat or general surgery for treatment of their skin cancer and were therefore able to avoid an unnecessary dermatology clinic visit. This efficiency gain occurs when the treating physician (in this case, ear/nose/throat or general surgery) feels comfortable that dermatology has seen the case and that the clinical diagnosis is so strong that an excisional rather than incisional biopsy is warranted. Therefore, the intermediate step is eliminated. Taking into account both the large volume of skin cancers that are diagnosed yearly in KP's Central Valley Service Area and the rising healthcare costs, an avoidance of unnecessary clinic visits by even 1% of the skin cancer patient population equates to a large cost-saving measure. We postulate that this 1% decrease in costs may not be reflective of the potential cost savings that can be seen with KPNC's teledermatology program today as at the time of this study the teledermatology system was not fully incorporated, and physicians faced a new workflow.
Although we did not investigate teledermatology's impact on obviously benign lesions, we postulate that the teledermatology program has led to fewer appointments with a dermatologist for obviously benign lesions, which equates to further cost savings.
Limitations to our study include that this was a retrospective study that was conducted in the KPNC Region in the Central Valley Service Area. KPNC's patient population might not be representative of other remote populations in the United States and beyond in regard to socioeconomic status, ethnic make-up, and utilization of medical services. Also, there were few MM cases identified through dermatology referrals during the 7-month time period we investigated, and the difference in the time to biopsy of these lesions between traditional e-consults and teledermatology referrals was not significant.
In sum, our results demonstrate that teledermatology consults were associated with a shorter time to biopsy for common skin cancers compared with traditional e-consults. We observed this despite the lack of access to dermatologists in the Central Valley before the teledermatology program was initiated. Overall, teledermatology leads to improved service for patients within a large, integrated health system in terms of a faster time to biopsy of non-melanoma skin cancer, improved streamlined referrals that are better at triaging patients, and large cost-savings measures that eliminate unnecessary dermatology visits.
Footnotes
Acknowledgments
We are indebted to Drs. Elizabeth Kass and Dennis Oh for their helpful discussions and review of our manuscript.
Author Contributions
E.K. and S.S. had full access to all of the data in the study and take responsibility for the integrity of the data and the accuracy of the data analysis. E.K., S.G., and S.S. are responsible for the study concept and design. E.K. and S.S. are responsible for acquisition of data. E.K., S.S., and D.C. are responsible for analysis and interpretation of data. E.K., S.S., D.C., and A.G. are responsible for drafting of the manuscript and critical revision of the manuscript for important intellectual content. D.C. is responsible for statistical analysis. S.G. and E.K. are responsible for study supervision.
Disclosure Statement
S.G. is employed by and is a shareholder of The Permanente Medical Group.