
Abstract
The Veterans Health Administration (VHA) is a large integrated healthcare system with a mission to care for over 5.6 million Veteran patients annually. VHA, like other healthcare organizations, is challenged with providing access to care to those it serves when they live at a distance from a physical site of care. VHA has embraced telehealth as a way of delivering care at a distance and increase access to specialty care services. Since 2003 VHA has developed large national telehealth networks that provided care to 497,342 patients in fiscal year 2012, who received 1,429,424 episodes of care, and is recognized as a national leader in this field. To ensure the safety and effectiveness of its telehealth networks in their delivery of care VHA has implemented a dedicated quality management (QM) program for telehealth. QM data for telehealth are reviewed at 3-month intervals, and the procedures and processes in place to support telehealth in VHA are assessed biannually in an internal accreditation process called “Telehealth Conditions of Participation.” This collegial, nonadversarial process has ensured that all designated telehealth programs meet minimal standards and disseminate best practice. As a result of VHA's QM program, telehealth services in VHA meet consistently high clinical outcomes and have received no adverse Joint Commission citations. The Joint Commission regularly assesses patients managed via telehealth under its tracer methodology reviews.
Introduction
The Veterans Health Administration (VHA) within the U.S. Department of Veterans Affairs (VA) provides care to over 5.6 million eligible Veteran patients annually. VHA serves its Veteran population through services delivered from 152 VA Medical Centers (VAMCs) and a further 1,100 additional sites of care that include community-based outpatient clinics, VET Centers, and other community outreach programs. Organizationally, the operational management of VHA's VAMCs and community-based outpatient clinics is accomplished through 21 regional administrative units called Veterans Integrated Service Networks (VISNs). Despite this inventory of physical assets from which it provides care, VHA, like other healthcare organizations, is challenged in providing convenient access to care, especially for Veterans living in rural and remote locations.
Telehealth 1 is the use of electronic information and telecommunications technologies to support long-distance clinical healthcare, patient and professional health-related education, public health, and health administration. For VA and other federal agencies in the United States, telehealth provides a means to expand rural access to care. 2 From July 2003 VHA has systematically implemented national telehealth programs with a focus on expanding access to care for Veterans. These national telehealth programs included home telehealth 3 (HT), which used a case management model and focused on addressing noninstitutional alternatives to care for those with chronic conditions (e.g., diabetes and chronic heart failure), store-and-forward telehealth (SFT), which focused primarily on teleretinal imaging to screen for diabetic retinopathy, 4 and clinical video telehealth (CVT), which focused initially on telemental health. 5,6
VHA's development of these national telehealth programs was based on prior work in the organization to develop systematic models of telehealth-based care and creating dedicated information technology platforms designed to provide services to hundreds of thousands of Veteran patients annually. A program office, Telehealth Services (formerly the Office of Care Coordination Services), was created to oversee the strategic development of telehealth in VHA, project-manage its implementation, and subsequently monitor associated clinical services to ensure their safety and sustainability. In planning the clinical, technology, and business processes requirements necessary to implement and sustain telehealth operations on this scale, a critical success factor that Telehealth Services identified was instituting an accompanying quality management (QM) system. With no comparable telehealth networks of the size and scope of those planned within VHA and no precedent for such QM activities in other organizations' telehealth initiatives, VHA established a telehealth-specific QM program as it project-managed its telehealth expansion.
VA's existing QM system and associated processes, supervised by VHA's Office of Quality, Safety and Value (OQSV) (formerly the Office of Quality and Performance), provide an exemplary QM framework for the delivery of traditional face-to-face services within VA. 7 In developing a QM system for telehealth, Telehealth Services worked closely with OQSV to develop a QM framework for telehealth that was consistent with VA's existing QM system for its other healthcare activities.
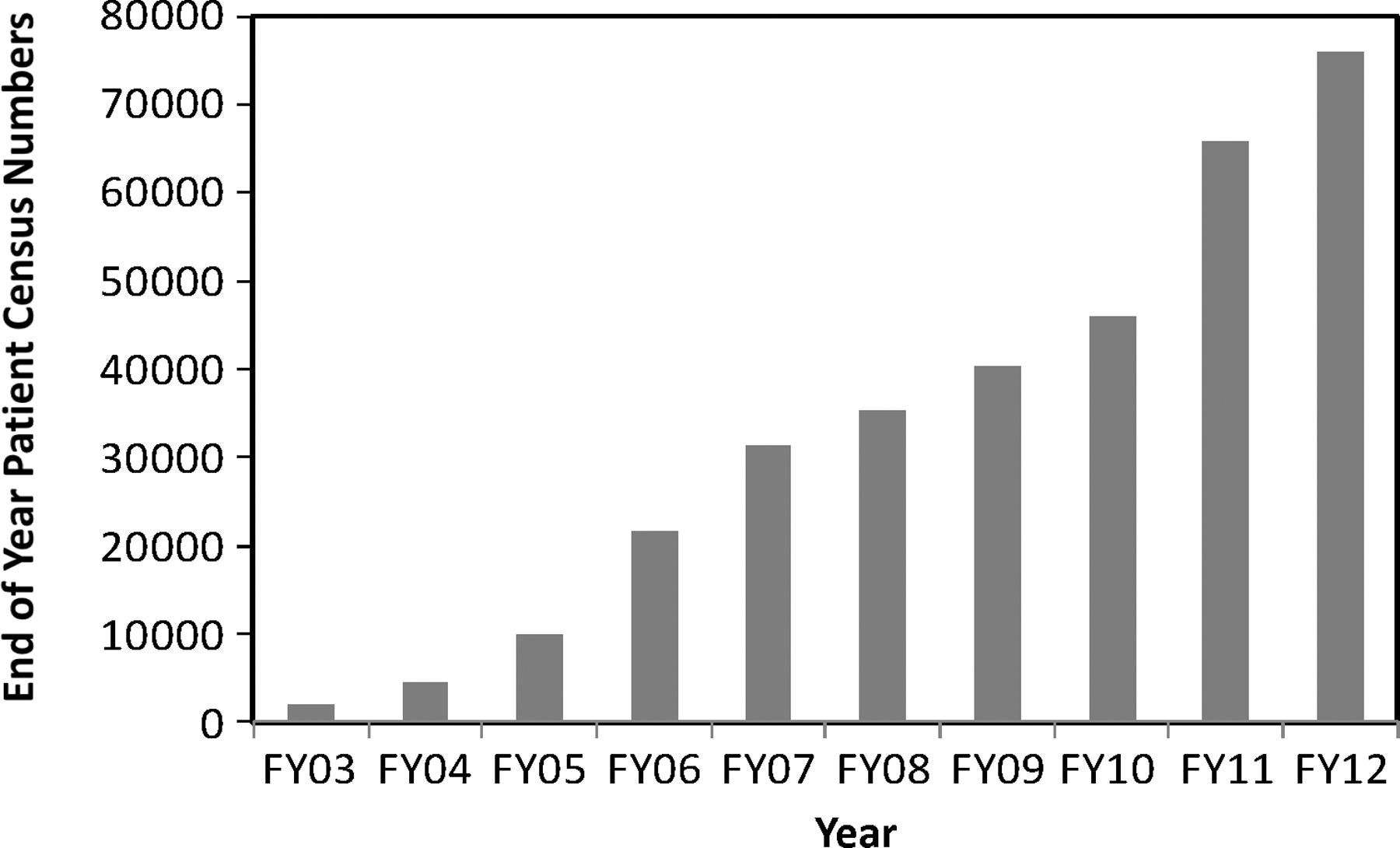
Figures 1 –3 show the growth of the national telehealth programs in VA from 2003 to 2012 to provide information on the scale of clinical operations of telehealth in VA and the context for implementing QM for telehealth.

VA store-and-forward telehealth patient numbers, fiscal year (FY) 2000–FY2012.
VA home telehealth patient numbers, fiscal year (FY) 2003–FY2012.

VA clinical video telehealth patient numbers, fiscal year (FY) 2005–FY2012.
Materials and Methods
In developing a comprehensive QM program to support telehealth expansion and sustainment in VHA, Telehealth Services worked with OQSV to define the scope for the QM program. Its requirements were as follows: • Supplementing VHA's existing QM processes to also cover the use of telehealth • Focusing on continuous quality improvement • Establishing a regular program of reviews for telehealth programs in VHA at the VISN or facility level • Providing data for peer review of programs and associated staff • Satisfying regulatory requirements • Covering risk management considerations including continuity of operations plans
In developing this QM framework for telehealth in VHA, Telehealth Services used the classic Donabedian approach 8 of structure, process, and outcome. Table 1 provides a matrix that shows how VHA's QM program for telehealth was designed to supplement the organization's existing QM framework and ensure the safe, appropriate, effective, and cost-effective delivery of care via telehealth with a minimum duplication of effort and resources.
Comparative Resources Matrix to Determine Telehealth Quality Management Framework
OQSV, Office of Quality, Safety and Value; QM, quality management; VAMC, U.S. Department of Veterans Affairs Medical Center; VISN, Veterans Integrated Service Network.
In establishing the standard operating procedures for its QM program to support telehealth expansion nationally in VHA, the design specifications identified in Table 1 were incorporated into two major operational components; the purpose of these was to generate ongoing objective data verifying that critical policies, procedures, and processes to support were in place and meet minimum standards and to assess appropriate outcome measures. These operational components were: 1. An “internal accreditation process” to review telehealth programs in VHA. This process was called conditions of participation (COPs) for telehealth. COPs for telehealth in VHA were initially defined and used for HT. Following the successful implementation of COPs for HT in VHA, COPs for SFT and CVT were subsequently developed. 2. A VHA Telehealth Scorecard was developed to collect routine outcome data quarterly and to make this available at the local VAMC, VISN, and national levels as part of systematic QM review of telehealth covering HT, SFT, and CVT.
Table 2 provides a selection of data items VHA currently includes in its VHA telehealth scorecards.
Selected Quality Management Data Elements for Telehealth Services Scorecards
HT, home telehealth; SFT, store-and-forward telehealth; VA, U.S. Department of Veterans Affairs; VR 12 Health Survey, Veterans RAND 12-Item Health Survey.
At the inception of the QM program for telehealth in VHA, Telehealth Services staff members met with staff from The Joint Commission to discuss the COPs and the COPs review process. These discussions included the crosswalk of the COPs with The Joint Commission standards chapters, identification of common goals, and defining common areas of focus. With subsequent revisions and expansions of the COPs and extending the review process to additional areas of telehealth, Telehealth Services met with staff from The Joint Commission again to update them on the COPs processes and to answer any questions about the Telehealth Services internal review process.
VISN and program level reviews related to the COPs for telehealth in VA are coordinated by Telehealth Services and undertaken by a dedicated QM team in VHA that is composed of three registered nurses, an optometrist, and an ophthalmologist. As additional areas of telehealth have been added to the COPs review process, relevant subject matter experts also participate in the review process. COPs reviews are designed to take place biannually in each VISN within VA. Although separate COPs were initially developed for HT, CVT, and SFT and reviews for these areas were undertaken separately, this process was subsequently combined into a single review process and a single site visit to each VISN at which the three major components of the review were undertaken concurrently. The reason for doing so was to avoid unnecessary administrative burden, improve operational efficiency, and obviate duplication. COPs reviews were undertaken using both physical site visits as well as virtual visits to sites. These reviews were expedited using tools such as high bandwidth videoconferencing, Live Meeting software (Microsoft, Redmond, WA) for virtual review of data and documentation, virtual review of documents and self-assessment materials posted on a SharePoint (Microsoft) site, and remote clinical workstation review in the case of teleretinal imaging for diabetic retinopathy. The process of conducting a COPs visit to a VISN typically involves a 4–5-day on-site visit, in addition to significant preparation by the VISN staff and prior review of self-assessment materials by the QM team. The COPs visit commences with an entrance visit with the telehealth program manager for the VISN and VISN leadership, including the Network Director for the VISN and the Chief Medical Officer.
The formal COPs review process examines: 1. VISN and program telehealth inventories and self-assessments using the COPs 2. Documentation in the form of written policies, procedures, and guidelines 3. Organizational charts 4. Training records 5. Routine QM data from scorecards, national datasets, and performance improvement initiatives 6. The care of individual patients utilizing a “tracer” methodology 7. Remote review of teleretinal camera workstations 8. Interviews with a variety of involved staff members
Table 3 outlines selected components of the Core COPs that apply to all telehealth programs as well as those COPs that are specific to HT, SFT, and CVT.
Selected Components of the Telehealth Conditions of Participation
CVT, clinical video telehealth; OIT, Office of Information Technology; VA, U.S. Department of Veterans Affairs; VHA, Veterans Health Administration; VISN, Veterans Integrated Service Network; MOU, memorandum of understanding.
Results
Cops Reviews
Including the piloting of the combined COPs review process in two VISNs, VA has conducted combined COPs reviews in all 21 VISNs between May 2009 and July 2011. Following reported successful completion of all required follow-up and corrective action items that were identified by the QM team in their final written report to the VISN Director, all VISNs have satisfactorily passed the COP review and been awarded Designation status.
Over the cycle of VISN reviews, considerable evolution occurred within each VISN's telehealth programs in meeting many of the COPs standards, as well as with regard to the organizational structures that support telehealth implementation and sustainment. Notable changes during the time frame of this cycle of COPs reviews include implementation of designated VISN Program Managers for Telehealth. A correlation was noted with deficits in meeting the COPs in those VISNs that had no such Program Manager or where the position had been vacant or in an acting capacity for a period of time at the time of review. In addition, many VISNs added facility-level telehealth coordinators, and many also added designated telehealth clinical technicians to support telehealth activities at the patient sites.
Relying on the success of the use of the COPs as standards for telehealth in the VA and on the review process as a means to help ensure quality and safety, COPs have also been developed for the newest emerging areas of telehealth in VA. As store-and-forward applications have been implemented for teledermatology, existing SFT standards have been adapted and added to the store-and-forward COPs that relate to these programs. As some VISNs have embarked on tele-intensive care unit initiatives, an additional set of COPs for tele-intensive care units, along with use of a program implementation checklist, has been developed and used for initial program reviews. These additional review initiatives using the COPs also show promise for being effective in ensuring quality and safety in these newer telehealth programs.
The most important areas of the COPs are those dealing with provisions to ensure patient safety, quality of care, and privacy and confidentiality as they relate to telehealth technologies. Supporting VISNs and facilities in their efforts to mitigate unwanted care trends in their systems and processes is a primary concern of the QM program. In those cases potentially involving quality, privacy, safety, or confidentiality issues noted during a COPs review, immediate corrective actions were required, along with a written report of actions taken, due within a short time frame. For elements requiring less time-sensitive corrective actions, written plans were typically due within 90 days, and they frequently resulted in ongoing consultations with the QM team and involvement of the designated telehealth training centers.
Commendable Practices
As part of the COPs review process, commendable practices were recognized as worthy of wider dissemination throughout VA. Table 4 provides examples of commendable practices that have been shared throughout VHA.
Selected Commendable Practices Noted During Conditions of Participation Reviews
CBOC, community-based outpatient clinic; COPD, chronic obstructive pulmonary disease; CVT, clinical video telehealth; HT, home telehealth; PACT, Patient Aligned Care Team; SFT, store-and-forward telehealth; VISN, Veterans Integrated Service Network; MOU, memorandum of understanding.
Discussion
The adoption of telehealth by healthcare systems is usually predicated on increasing access and quality of care. 9 Although the need for quality monitoring in telehealth has been identified, 10 efforts associated with QM in telehealth by healthcare organizations, to date, have focused on equipment, 11 rather than on the critical clinical and organizational processes that are necessary to safely develop and sustain telehealth services. One reason for this technology-centric focus is the variability of telehealth programs among different medical specialties and their frequent short-term nature 12 in many institutions. Perhaps because of this short-term nature of telehealth programs and associated lack of systems support, many telehealth programs have been “cottage industries” in which relationships rather than formal processes have predominated in their models of care delivery. As a result there has been a tendency to view telehealth as providing healthcare services and to consider that, apart from the technology, no particular QM systems or related training is required to support telehealth.
When a telehealth program is small, for example, a point-to-point CVT between a hospital and a distant clinic involving a clinical champion with his or her dedicated staff, the telehealth program can mirror traditional practice directly. Staff training and quality management can take place through informal mechanisms and personal relationships. It was VHA's experience before 2003 that such informal telehealth programs were often not sustainable if key individuals left. This resulted in telehealth as an interesting adjunct to usual care, but one that was difficult to sustain as a mission critical service.
From 2003, with adoption of a specific strategy to develop large telehealth networks, VHA moved from an informal and ad hoc process of telehealth development to a “systems” approach. With large telehealth networks of hundreds of providers delivering care to hundreds of thousands of patients, informal relationship-based processes for care delivery, training, and QM were no longer tenable. Healthcare services are variable between institutions, 13 and by its very nature telehealth crosses between institutions and exposes risks from variability that is magnified during care transitions. 14,15 Because of the inherent patient risk associated with variability and uncertainty, VHA developed standardized models for telehealth with associated training mechanisms and explicit ways to code clinical activity conducted via telehealth. Although patient safety was of paramount concern, an associated consideration was that of external accreditation reviews of VHA healthcare facilities, such as The Joint Commission.
There is no specific, focused review of telehealth undertaken by The Joint Commission in the United States. However, as they conduct the Commission's “tracer methodology,” 16 “Joint Commission surveyors retrace the specific care processes that an individual patient experiences by observing and talking to staff in areas that the individual received care. As surveyors follow the course of a patient's, resident's or client's treatment, they assess the healthcare organizations compliance with Joint Commission standards. They conduct this compliance assessment as they review the organization's systems for delivering safe, quality healthcare.” Therefore, all telehealth programs are potentially subject to Joint Commission review. Having such programs without clear policies, processes, and procedures would not only expose patients to undue risk, it would also expose the organization to the potential consequences of an unfavorable Joint Commission review.
Faced with the necessity for a QM process, VHA developed such a process in synergy with the existing QM system and avoided replication and confusion. To date, there are no instances of Joint Commission warnings or citations associated with telehealth programs in VA despite the hundreds of thousands of patients served and the delivery of care across a continuum that includes 1,200 sites of care, as well as care of 119,535 patients in their own homes in fiscal year 2012. The COPs have not only ensured the quality of care, they have formed the basis of a continuous quality improvement process, 17 as exemplified by the nature of the process that sought to be collegial and not adversarial. The process also identified and disseminated commendable practices. Wherever possible and practicable, VA used health information technologies to measure outcomes and ensured quality of care across the continuum, as have been shown elsewhere. 18
VA has approached the issues of technical quality of the information technology systems to support telehealth through developing memoranda of understanding and service-level agreements among the program office Telehealth Services, VA's Office of Information and Technology, and Biomedical Engineering. This aspect of quality is an important adjunct to the QM process already described to ensure continuity of care and patient safety. 19
Of particular importance in the COPs process is the identification of the organizational relationships and processes necessary to sustain large telehealth networks. This is because telehealth programs operate in “an unusual organizational environment. They are composed of distributed systems, usually cooperative ventures linking independent hospitals and clinics. There is often no clear hierarchy of administration, leadership, or authority…this can magnify communication and organizational problems.” 20
The framework for QM for telehealth in VHA aligns well with principles adopted elsewhere, 21 based on ascertaining the adequacy of the therapeutic practitioner–client relationship, providing and documenting care, clearly defining roles and responsibilities, ensuring consent, privacy, and confidentiality are of paramount importance, and other ethical and legal considerations. The ethical issues in telehealth are complex 22 and evolving. They include issues of equity of access to both traditional face-to-face services as well as to telehealth, and not only health disparities 23 are important but also issues associated with the digital divide. The COP process raises such ethical issues that can be expected to evolve as telehealth practice grows, and these concerns need to be addressed proactively.
Adopting the traditional Donabedian model of quality was very helpful in developing the QM framework for telehealth in VA. However, in a rapidly evolving field where both technology and clinical practice are changing rapidly, the Donabedian approach is an older static model that has limitations 24 when applied to a dynamic healthcare system where interpersonal process aspects of care seem to be of much greater importance in defining and measuring quality.
Conclusions
1. VA's experience shows the importance of introducing a QM framework as an intrinsic part of developing large telehealth networks.
2. These QM systems should supplement existing QM systems.
3. As a rapidly evolving area of healthcare development with staff members, who are not primarily trained in their professional disciplines to use telehealth, there is a need to use the QM process as a means of continuous quality improvement and to support interdisciplinary care.
Footnotes
Disclosure Statement
No competing financial interests exist.