
Abstract
This article provides background information on the history of telemedicine in Arizona and the Arizona Telemedicine Program (ATP). Following a brief overview of the growth of the ATP over the past 16 years, special focus is directed toward a description of the ATP business model, sustainability efforts of the Program, and ATP's future directions and goals. The ATP was established by the Arizona State Legislature in 1996 and, today, operates a large university-based statewide telemedicine consortium. It provides a spectrum of telemedicine support services to dozens of independent healthcare organizations throughout Arizona and bordering states. The ATP's backbone is a regional, 160-site dedicated healthcare and education broadband telecommunications network called the Arizona Telemedicine Network (ATN). The ATN is a fixed-cost network operated 24/7 by ATP engineers. In addition to providing access to the ATN, the ATP also provides its member individuals and organizations with benefits including biomedical communications services and expertise, telemedicine training on financial, legal, regulatory, and administrative support aspects, and access to subspecialty telemedicine consultation services.
Telemedicine in the State of Arizona
The Arizona Telemedicine Program (ATP) has benefited from a multigenerational telemedicine presence in Arizona, which has contributed directly and indirectly to its sustainability. 1 –4 Telemedicine in Arizona antedates the creation of the ATP and can be traced, in part, to perhaps the earliest multispecialty telemedicine services delivered by the Massachusetts General Hospital–Logan International Airport Medical Station telemedicine program. The ATP benefited from this legacy as Ronald S. Weinstein was one of a group of Massachusetts General Hospital resident physicians participating in providing the first clinical telemedicine services in 1968. Jay Sanders, another member of the Massachusetts General Hospital group, established a telemedicine program in Miami, FL and in 1993 led the Georgia Telemedicine Program. In 1994 Arizona State Representative Robert Burns heard Sanders speak on the Georgia program. He visited it and returned to Arizona enthused about the opportunities to be found in telemedicine's capability to provide services to remote and underserved populations.
Meanwhile, in 1971 the National Aeronautics and Space Administration (NASA) was interested in developing a prototype telemedicine project that would go well beyond what was being done in Massachusetts. NASA was intent on showcasing terrestrial applications of space medicine being developed and implemented as part of their “manned space” program. NASA envisioned a telemedicine-based healthcare delivery system linking, by real-time video, innovative mobile telemedicine vehicles, community health centers, secondary hospitals, and tertiary hospitals, linked by a microwave-based broadband telecommunications network. Patients would have portable electronic health records, a new concept at that time. Several sites competed for the project, 1 which was awarded to the Papago Tribe (known today as the Tohono O'odham Nation), a large Reservation bordering Tucson in Southern Arizona.
Concurrently in the early 1970s, the University Medical Center on the Arizona Health Science Center (AHSC) campus in Tucson established itself as a leader in healthcare system computerization and patient electronic health records. The dean of the College of Medicine, Merlin K. DuVal, envisioned creation of an “all-electronic” paperless hospital with an in-house electronic laboratory information system. Space Technology Applied to Rural Papago Advanced Healthcare (STARPAHC) was part of NASA's terrestrial telemedicine program to support the larger U.S. Space Program, running from 1971 to 1975. It ended when the government funding ceased—despite the successful implementation of important innovations and the achievement of positive, well-documented, clinical outcomes that met the expectations of STARPAHC administrators. Its abrupt termination was disruptive to the Papago patients and the Indian Health Service (IHS). 1 Nevertheless, STARPAHC's accomplishments made an indelible impression in Arizona, which still benefits the ATP today.
There were other telemedicine initiatives in the Southwest in the early 1970s. During STARPAHC's tenure, planning was underway at the University of Arizona's (UA's) Department of Family and Community Medicine to develop a multitribe IHS telemedicine program. The network would join IHS hospitals and clinics on five Reservations (Papago, Hopi, San Carlos Apache, White River Apache, and Navajo) and extend from the northern to the southern Arizona border. The plan was to design, install, operate, evaluate, and maintain a telecommunications network to be utilized by the IHS and to assess the network's impact on the delivery of medical services and patient outcomes. Among others, specific network objectives were (1) to direct diagnostic, medical, and therapeutic services and to provide (2) on-line supervision, advice, and medical consultation to health service personnel, (3) radiographic and laboratory interpretations and other technical ancillary services via biotelemetry, video, facsimile, and computer analysis, (4) online computerized health information on individual patients, and (5) educational activities to upgrade skills of healthcare personnel. 5 The demise of STARPAHC played a role in closing the door on the five-nation telemedicine network plan.
In the early 1970s there was also communication and fact-sharing among the telemedicine planning groups at the UA and the University of New Mexico (UNM). In 1975, Phelps Dodge Corporation opened its Playas Telemedicine Clinic, the product of the detailed planning of the Playas Telehealth System (PTS). Design and implementation had been the shared responsibility of the New Mexico Health Resource Center, UNM, the not-for-profit MITRE Corporation, and Phelps Dodge. UNM faculty and staff participated in all aspects of the planning, implementation, and assessment of the PTS. The PTS was implemented in a medical clinic in a Phelps Dodge company town near a copper smelter, to provide primary care and specialty medicine services, by telemedicine, for employees, their families, and other local residents. The telemedicine service providers were in Silver City, NM, 100 miles to the north of Playas, NM. The Playas telemedicine service was active for a quarter of a century, until the copper smelter was closed because of declining copper prices in the year 2000. After a hiatus of many years, UNM and the UA telemedicine groups now work together and in 2004 founded the Four Corners Telehealth Consortium.
Since 1979, the AHSC has provided continuous “telemedicine services.” The Arizona Poison and Drug Information Center provides telephone-based services to answer questions from patients and providers throughout the state on poison and drug exposures, 6 handling approximately 70,000 inquiries a year. Since 1990, the UA Health Network Physician's Resource Service has provided physicians across the state with telephone-based and e-mail patient-specific specialty consultations without charge. It provides 11,000 medicine consultations to off-site physicians per year. Telepathology services were initiated in Arizona, Mexico, and China starting in 1992, 7 and teleradiology has been offered continuously to some 25 hospitals in Arizona and adjacent states since 1994. 8
ATP Legislative Mandate
There were several telemedicine initiatives involving the Arizona State Legislature (ASL), the Arizona Department of Health Services (AZDHS), and AHSC between 1993 and 1996. 9 The ASL budgeted $1.2 million to centralize these initiatives and to fund the first year of operations for a new Arizona Rural Telemedicine Network (ARTN). (The ARTN was later renamed the Arizona Telemedicine Network [ATN] but retained the name ARTN in the Arizona State Budget.) The initial charge to ATP was to establish telemedicine services in eight rural sites, including one at a Department of Corrections facility, one at a hospital on an Indian Reservation, and six at non-Indian rural hospitals. The AHSC was designated by the ASL as the ATP's administrative hub, with Weinstein as its founding Director. 2,3,9 –15 Ironically, UA had not proposed the creation of the telemedicine program and was surprised to find the ARTN as a new line item in the 1996 state budget for the AHSC. The proposal for the program was “self-generated” within the ASL, and the ASL continues ownership of the ATP and strongly supports the ATC with a commitment to its sustainability. 9 One lesson to be learned from the ATP experience is the importance of ongoing support by significant gatekeepers.
As originally envisioned, the ATP would oversee and coordinate telemedicine clinical, educational, research, and telecommunications programs and operate the ATN. This expanded role was endorsed by the House and Senate Appropriations' Committees of the ASL. Today the ATN spans the state of Arizona, and the ATP with its multi-organization panel of service providers offer telemedicine services at 160 sites in Arizona and some of its neighboring states (Fig. 1).
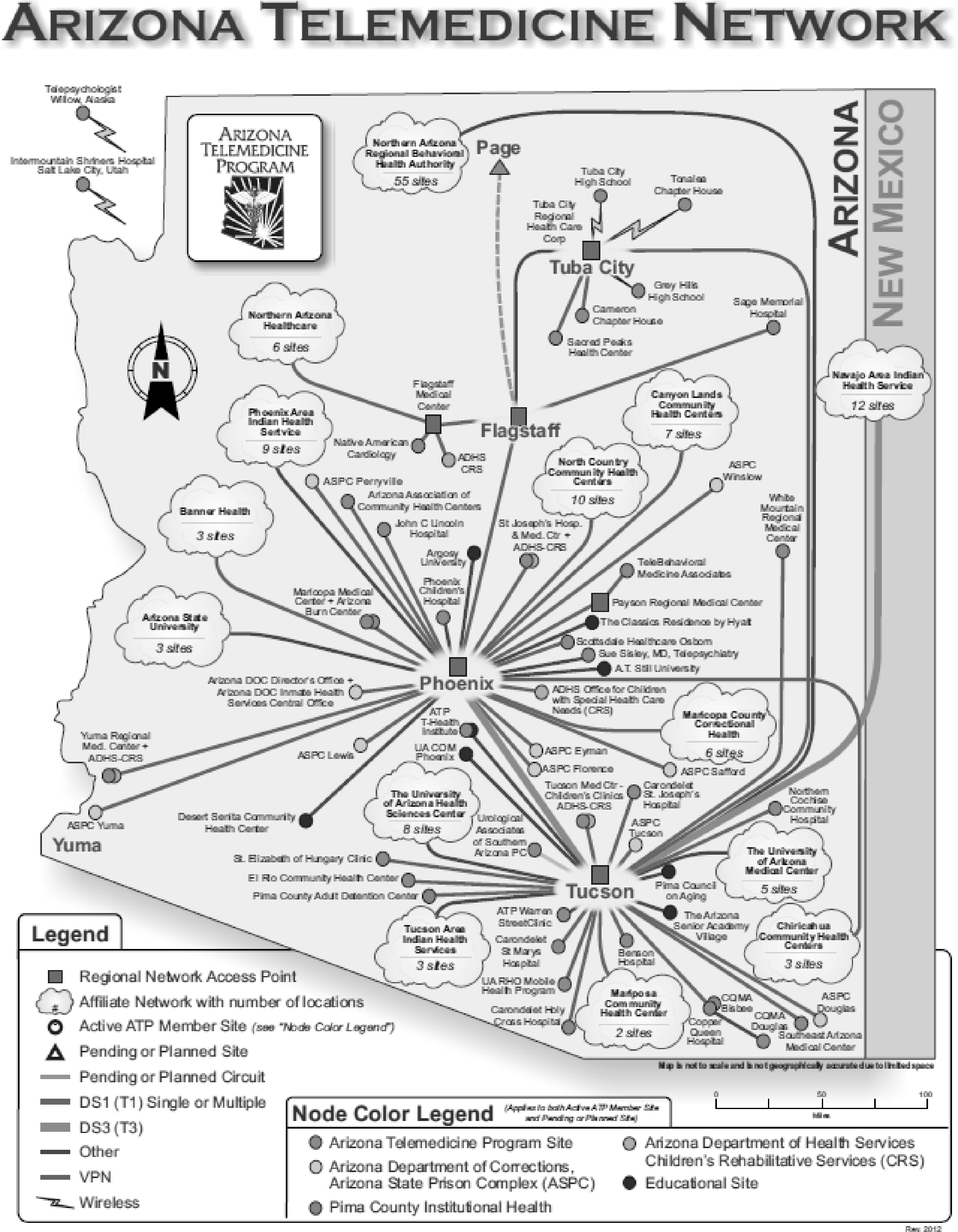
Map of the Arizona Telemedicine Network.
ATP Goals Become Arizona Telemedicine Public Policy
The primary mission of the ATP is to enhance healthcare delivery to medically underserved populations throughout Arizona using telemedicine technologies. Additionally, the ATP's vision is to be a leader and significant player in development and implementation of telemedicine and telehealth services, technologies, and education programs. As such, the ATP has eight charter goals originally endorsed by the ASL at the time of ATP's creation and that serve as a framework and guide to the ATP's efforts and future directions. 9,10
The goals (and corresponding public policies) are as follows: • to create a single multiservice telemedicine program • to establish a program governance framework with an overarching authority structure to support the unique missions of a telemedicine organization • to operate the ATP as an inclusive virtual organization capable of creating incentives for all healthcare organizations to participate in a single telemedicine program • to provide access to the ATP's telecommunications infrastructure for all legitimate healthcare organizations • to encourage the development of interoperability of all telemedicine facilities • to develop an open staff model for participation of telephysicians as service providers for multiple healthcare organizations • to promote evidence-based best practice guidelines • to have the ASL encourage state agencies, including the Department of Corrections and AZDHS, to participate in the ATP.
The foregoing historical overview of the development of the ATP pertains directly to the major themes of this article, namely, sustainability and future development of telemedicine. The all-encompassing goals and public policies listed above were deemed essential to establish ATP's status as a statewide agency. The philosophy underpinning this approach is that a more limited set of goals and corresponding public policies probably would have been approved in a piecemeal fashion, 9,16 and, had they been approved, the ATP may have been viewed as “just another” university telemedicine pilot project, rather than supporting its status as the start of a large, open-ended, inclusive statewide telemedicine enterprise. 3 Approval by the ASL also resulted in a 3-year funding cycle that included a “sunset” clause if expectations were not met. Fortunately, interim goals were met, and the first federal grant had been awarded, thus gaining support for an additional role for the ATP, namely, as a recognized academic program at UA.
The UA College of Medicine designated the ATP an academic department, enabling it to manage its own extramural grant portfolio. In 2004, state funding was significantly increased when a federal budget set-aside funded a new division of the ATP, the Institute for Advanced Telemedicine and Telehealth (T-Health Institute), located on the Phoenix Bioscience Campus. The T-Health Institute provides telemedicine training programs and curriculum development and for distance education. 17 –19
Arizona Telemedicine Council
The Arizona Telemedicine Council (ATC) was created by the Joint Legislative Budget Committee of the ASL in 1996, concomitant with the creation of the ATP. The ATC has played an important role in ATP's sustainability. It was implemented to provide a direct communications bridge between the ATP and its ASL. 9 Today, it is regarded one of the ATP “cornerstones.” Its creation reflected early recognition of the complexity of the academic and political landscape of the medical communities in Tucson, Phoenix, and the state's rural communities. The ATC is the “non-statutory overarching authority” providing oversight of ATP initiatives, but fiduciary oversight is provided by the College of Medicine.
The ATC is chaired by a present (or former) member of the Joint Legislative Budget Committee and is composed of members from public and private sectors. (In 2012 the ATC members include state legislators, public agencies [e.g., Department of Corrections, Department of Health Services], public members [e.g., Indian Health Services, Mayo Clinic, Barrow Neurological Institute], and ex-officio members [e.g., Northern Arizona Behavioral Health Authority, Arizona Department of Education].) It has met quarterly since 1996. In addition to having financial oversight of the ATC, agendas include progress reports on various independent Arizona telemedicine programs. The ATC enhances communication and interoperability between these programs and, thereby, the probability of their success. Meeting minutes go directly to the Director of the Joint Legislative Budget Committee and satisfy the Legislature's reporting requirement. In addition to performing an important oversight function, the ATC plays a significant role in promoting telemedicine in Arizona.
ATP Business Model
The ATP is an inclusive statewide telemedicine collaborative incorporating several independent healthcare organizations in both the private and public sectors. The ATP business model derives from an application service provider business model popular in the computer software industry in the 1980s. It uses a membership model formalized through legal contracts coupled with a shared-cost model to capitalize on economies of scale by sharing services at lower costs. 5,7,10,20,21 Sharing services across multiple healthcare organizations has contributed significantly to ATP's growth and sustainability. 22,23 Other advantages include low capitalization and low management and staffing overheads.
Approximately 30% of the ATP's revenue is derived from annual membership fees, 45% from state support, 24% from grants, and 1% from the UA. In 2012, full membership cost $5,400 with a multisite discount available. As many as 55 healthcare organizations have been members at any one time. The ATP business model can be thought of as consisting of three tiers, namely, physical infrastructure, operational services, and client. The bottom tier is the foundation, the physical telecommunications infrastructure of the network (e.g., leased T-1 and T-3 telecommunications lines) composed of vendor services. It represents services that support the basic ATP structure, including telecommunications, marketing services, funding support, and grant writing. This is the core of services that clients obtain with membership. The intermediate tier is composed of operational services and includes the activities essential to daily activities, such as clinic operation, equipment installation, practice management, training, transcription, billing, and reimbursement. It includes those actual services supported by or supplied by the ATP, including those of healthcare providers, clinical protocol development, continuing education, quality assurance, credentialing, licensing, and legal. Finally, the third tier is the client tier, which includes a range of clients such as patients, payers, or businesses that utilize the services supported by the ATP. Once members, clients may select (and pay for) desired services from a flexible model/menu. For example, a facility may contract for clinical teleconsultation services but have no need for distance education, therefore paying only for the former.
It is important that this model allows ATP members to maintain their traditional patient referral patterns. They may purchase, for example, access to the telecommunications infrastructure but not the clinical services operated by the ATP hub site, instead using their telecommunications link to connect to their existing specialty referring site if it is on the network. This model has provided a steady revenue stream that, when combined with recurring state funds and nonrecurring external funding for special projects, has contributed to the ATP's sustainability.
The ATP also serves as an umbrella organization and fosters the establishment of important innovative extramurally funded programs such as the Arizona Diabetes Virtual Center of Excellence, ¡VIDA!, and the Southwest Telehealth Resource Center (SWTRC). 12,24 –29 In each case, the program was initiated by applying for and receiving federal and/or state funds to support an initial infrastructure and human resource development. As extramurally funded projects evolve they become formally and operationally integrated into the ATP, creating a sustainable foundation into the future. Some members of the ATP Executive Team receive only partial support from the ATP, while their primary financial support comes from their affiliated department and grant funding. The team is currently composed of 23 members, and the program supports 16.2 full-time equivalents on its Tucson and Phoenix campuses.
ATP Branding and Marketing
An early ATP priority focused on creating a statewide “branding and marketing” strategy to coincide with the first public service announcements and advertisements for ATP. The central theme for the ATP was statewide resource access and sharing. The first steps included developing a standardized signage (logo) for remote sites and encouraging members to display them during video encounters, as well as standardizing the design and appearance of telemedicine lab coats. All personnel funded by the ATP, including site coordinators at the eight charter member sites, were encouraged to wear their “telemedicine-blue” lab coats when using the ATP video system. Through advertising, the display of ATP banners and accessories, and demonstrations and presentations at local, regional, and national meetings, there was and continues to be a growing awareness of the ATP.
ATP Administrative Units
Based on the National Cancer Institute Comprehensive Cancer Centers' model, the ATP has five administrative units designed to leverage synergies among units: patient services, distance education, basic and translational research, training, and infrastructure. 10
Infrastructure/Telecommunications Services
The ATP established a “virtual” telecommunications utility that functioned within the UA. The network and related infrastructure are primarily devoted to improving access to specialized medical care throughout the state using telemedicine technologies such as digital imaging and real-time videoconferencing. 13 The ATP (via the Arizona Board of Regents) “owns” the ATN, which is a private, scalable, Internet protocol–based, broadband telemedicine communications wide area network with connection speeds ranging from 1.5 megabits per second (Mbps) to 45 Mbps.
The ATN links the UA campus, Internet, and Internet 2 networks at 1 gigabit per second via firewalled interconnections. It is supported 24/7 by a dedicated team of ATP engineers who proactively monitor network, video, and computing infrastructure operations and troubleshoot any network problems to resolve any operational issues. ATP members that observe problems are encouraged to contact the engineers via the ATP service desk. ATP engineers provide a full range of managed point-to-point and multipoint videoconferencing services for member organizations. The ATP uses various real-time videoconferencing and store-forward technologies, as well as peripheral devices in its clinical services. Member sites are not required to use the same equipment, but ATP staff provides specifications of compatible applications and network equipment. Members are strongly urged to select ATP-compatible equipment in order to ensure successful utilization of the ATN's clinical and educational capabilities.
Several independent telemedicine programs in Arizona use the ATP's ATN infrastructure and member benefits. Affiliates include the Northern Arizona Regional Behavioral Health Authority, 30 the Arizona Poison & Drug Information Center, 6,31 Banner Health, a centralized call center for electronic intensive care units, United Health, an insurer providing integrated telemedicine services in two Arizona rural communities, the Mayo Clinic Telestroke in Scottsdale, utilizing the ATP's training programs and ATP instructors for courses in the area of telestroke, 32 –34 and the Telemedicine Digital Retina Imaging facility at Mountain Park Community Health Center at St. Lukes' Hospital in Phoenix.
Telemedicine and Telehealth Training
A second key component of the ATP is training. In addition to providing specialized training for specific clinical applications and situations, 25 –27 a program was established in Tucson for potential telemedicine users to participate in a course offered by ATP staff. Training is now done simultaneously on the AHSC Tucson campus and at the T-Health Institute in Phoenix. 11,17 –19 The training centers are linked together for videoconferencing.
In 2010 the ATP received funding from the U.S. Office for the Advancement of Telehealth to form a subsidiary unit to provide additional training opportunities via the SWTRC. 29 The SWTRC assists start-up telehealth programs in their development and serves as a resource for existing programs regarding changes in technology and other issues affecting telehealth in the Southwest region. (Over the past 3 years the SWTRC had over 1,110 training and advice contacts, primarily to parties in five states but also from other locations across the United States as well as Argentina, Australia, Canada, China, Columbia, United Kingdom, France, Ghana, Iran, Japan, Norway, Russia, Serbia, South Africa, and Switzerland.) The SWTRC offers a quarterly “Webinar” series highlighting topics in telemedicine especially relevant to the Southwest region.
Distance Learning
The ATP offers several opportunities for member sites, including grand rounds viewed “live” via interactive videoconferencing. The ¡VIDA! Program, supported by the AZDHS and the Susan G. Komen Foundation, 28 was established primarily as a program for breast cancer survivors. Its mission is to facilitate access to health promotion information and to provide and evaluate culturally and linguistically appropriate health education for patients and their families, lay health educators, and the general public. The curriculum topics are developed by clinical and support personnel and cancer survivors. Each session is conducted as a virtual roundtable teleconversation with clinical experts and is accessible in English and Spanish. The educational content is also available via live videostreaming.
Several independent, non-university organizations rely on the ATN for broadband telecommunications services for their own educational programs. Although network sites function autonomously, when they require the additional services of a bridge to connect to multiple sites, the ATN engineers make these connections. These site-to-site and multisite events tend to take place along existing specialist to primary care provider referral patterns and are supported through membership fees.
There are numerous examples of non-university educational programs that utilize the ATN infrastructure. For example, the Banner Good Samaritan Hospital in Phoenix connects with the Tuba City Regional Medical Center 222 miles away on the Navajo Reservation. In turn, Tuba City connects to Phoenix College for educating laboratory technicians. And, the Flagstaff Medical Center in Northern Arizona connects with a site in Verde Valley, 52 miles away, to provide periodic educational programs. North Country, a group of community health centers in Northern Arizona, holds weekly classes with physicians in a dozen communities on infectious disease education, especially with regards to hepatitis C clinical management. Thus, rural Arizona and its metropolitan areas are interlaced with several small “virtual networks” that share ATN telecommunications infrastructure, engineers, and expertise. Growing numbers of independent healthcare organizations outside the UA Health Network are encouraged to access to ATN, through ATP membership, to bring educational content by videoconferencing to a broad range of institutions. This enriches educational programming, customizes content to local needs, and contributes to the promotion and maintenance of traditional patient referral patterns. The diversity of “outside-the-university” users of the ATP's education infrastructure increases its “footprint” within the state and ultimately the sustainability of the ATP.
Assessment/Translational Research
The ATP fosters research and program assessment in telemedicine and telehealth within its core program and its subsidiaries. For example, the Arizona Diabetes Virtual Center of Excellence program for diabetes prevention, assessment, and management provides training for community health center staff on screening protocols, tele-ophthalmology consultations, care coordination for eye problems, telepodiatry, tele-wound care management, and a mobile health program. 24 The program was originally funded by Office for the Advancement of Telehealth and is now supported by the Office of Health Systems Development of the AZDHS. 35
Beyond Arizona, through funding from sources such as the U.S. State Department, USAID, and the Department of Defense, the ATP has assisted several countries in developing and assessing telemedicine programs. 10,35 In addition, the ATP has supported the activities of the International Virtual e-Hospital Foundation.
The ATP's research mission is also to assess a full range of telemedicine technologies. 36 –41 The ATP and UA Department of Pathology faculty have participated in Small Business Innovation Research grants from the National Cancer Institute and the National Institute for Biomedical Imaging and Bioengineering supporting the commercial development of digital colposcopy, digital pathology, and telepathology equipment. 42 –48 Observer performance studies assess the impact of telemedicine technologies on the end-users and their decision-making processes. 49 –53 Additionally, studies have been conducted to determine the utility and cost-effectiveness of telemedicine 36,37,54 –57 with special emphasis on patient outcomes. 37 –40,56,58,59
Telemedicine Services
The ATP is an “open staff” network of service providers and does not require member sites to refer its consultations to the AHSC hub site. Site-to-site consultations are strongly supported and encouraged, especially when they maintain existing referral patterns. Providers may be either university or non-university based.
University-based telemedicine services
To date, UA faculty-physicians have offered teleconsultations in over 60 clinical subspecialties using both store-forward and real-time technologies, including over 1.25 million teleradiology cases and over 15,000 patient contacts in other subspecialties. The most common store-forward application (after teleradiology) has been teledermatology, with nearly 2,800 teleconsultations. The most common real-time subspecialties have been telepathology (3,500 cases), telepsychiatry (over 3,700 cases), telecardiology (over 700 cases), telerheumatology (over 400 cases), and tele-infectious disease (over 300 cases). Nonradiology cases handled by university faculty-physicians represent the minority of nonradiology cases handled over the ATN.
Non-university telemedicine services
Many telemedicine cases conducted over the ATN are not tracked by the UA because cases are not handled by university physicians, so numbers of overall case encounters cannot be accurately assessed. Nevertheless, it is estimated that over 30,000 prison telemedicine cases have been handled by non-university telephysicians. The Arizona Foundation for the Eye reported over 4,100 digital retinal screening cases in which 30% unexpected abnormalities were detected.
Southwest Regional Partners
As mentioned previously, the ATP is a charter member of the Four Corners Telehealth Consortium. 60 The Consortium, initially funded by the Department of Defense, had as one of its objectives to develop strategies for overcoming jurisdictional barriers to interstate telemedicine and telehealth practice. Specific collaborative efforts included working on the establishment of an interstate licensure process (which remains a work-in-progress), coordination of a virtual “e-health” university for distance learning, coordinating provision of “best practices” telehealth clinical services, and developing an interstate disaster response.
Research University Environment
Locating a statewide telemedicine program at a research university can be a two-edged sword. On the one hand, basic and translation research are welcomed and encouraged, and collaborative research with major corporations helps keep the program current. On the other hand, university expectations with respect to scholarly productivity and extramural funding can be burdensome and therefore an impediment to the primary mission, namely, to bring specialty medical services to geographically underserved populations.
A steady stream of extramural funding, preferably from multiple agencies, is being important for the long-term sustainability of a university-based program. The ATP faculty is on a constant quest for funding opportunities. As a practical matter, the ATP occupies UA College of Medicine space designated as “research space” despite its clinical mission and its obvious medical service contributions. “Research productivity” (i.e., extramural indirect cost recovery as a surrogate for research productivity) of the ATP is monitored by the Medical School and the University.
Looking to the Future
The future of telemedicine, in part, may be found in mobile technologies. 61 –66 Over the next few years the field is expected to witness a rapid deployment of wireless and mobile Internet-based mobile health systems. Home medical care and remote diagnosis are expected to become common. With recent federal mandates regarding changes in healthcare, the electronic health records incentive program, 67 accountability, and meaningful use, 68 preventive medical care using mobile and Internet-based technologies will be emphasized for individual health management. 69 –71 Finally, the promise of the “smart home” using sensors, multimedia devices, and other advanced communication and monitoring technologies will also start to be practically realized within the next 10 years. 72,73
Two recent literature reviews on the effectiveness of telemedicine suggest some clear paths for future research directions. The first one 74 reviewed telemedicine for the management of five common chronic diseases—asthma, chronic obstructive pulmonary disease, diabetes, heart failure, and hypertension. There were 141 randomized control trials with 37,695 patients that met the criteria for inclusion in the review. Overall, 73% had outcomes favorable to telemedicine, 26% had no significant differences from the controls, and only 1% had outcomes unfavorable to telemedicine. Although these findings are clearly supportive of telemedicine, two caveats were noted: publication bias against negative results and the short duration of studies.
A second article 75 reviewed systematic reviews of the telemedicine literature to summarize the various methodologies commonly used as well as recommend approaches for future research. Out of 1,593 initial articles, only 50 reviews directly addressed assessment methods. Nevertheless, four future research directions were identified: (1) the need for more rigorous, controlled studies assessing impact; (2) standardization of populations, interventions, and outcomes measures to reduce the heterogeneity of the data and facilitate the conduct of meta-analyses; (3) conduct more studies that combine qualitative and quantitative methods; and (4) studies conducted with naturalistic methods (e.g., observational) in natural settings (e.g., practicing telemedicine clinics). Should these be followed, research is expected to have a significant impact of academic center–based telemedicine programs such as the ATP.
Sustainability
The long-term sustainability of the ATP seems secure. Foreseeable changes include a diminished need for the ATP's original hard-wired network's broadband as wireless telecommunications becomes ubiquitous. Additionally, many services enabled by access to the ATN are likely to outlive the ATN as individual programs and clinics establish their own networks and alternative infrastructures (especially mobile-based applications). Cost-sharing of information technology personnel, education experts, and access to a broad spectrum of telehealth services are benefits that would likely survive replacement of the original T-1/ATM telecommunications infrastructure. The hope is that the ATP's track record in innovation and healthcare resource sharing, both reducing costs and broadening the availability of specialty medical services, will continue to justify the ASL's investments in the future of telemedicine through its flagship state university. The ATP staffs' development of high-quality telemedicine-related academic programs at UA, leveraging both ATP and SWTRC resources and garnering significant extramural funding from multiple federal agencies, matches up well with the core missions of UA as a land-grant research university.
Footnotes
Disclosure Statement
No competing financial interests exist.