
Abstract
This article highlights the deployment of telemedicine by the U.S. Army through the various echelons of care and in overseas locations, including range and scope of health services provided by telemedicine in a challenging environment. This is followed by a discussion of technological developments advances in mobile communications likely to change the practice of telemedicine in the military from limited fixed-point access to a highly mobile individual with handheld communication devices.
Introduction
The U.S. Army early on recognized the additional new capabilities telemedicine could provide and help improve the delivery of care for its servicemen and -women at home, abroad, and in war zones. Since 1992, military medicine has considered the relevance, the sustainability, and the promise of telemedicine in the context of its mission and its obligations. 1 More recently, with advances in mobile technology and increased adoption of the smartphone with increasing sophisticated capabilities such as use of the smartphone camera for imaging and diagnosis of dermal problems, another new medical capability now widely called mobile health, or m-health, has emerged. 2 m-Health is complementary to telemedicine and should be viewed as another tool for practicing or implementing telemedicine. This article highlights the use of telemedicine and m-health in the Army for augmenting care in the military health system.
Telemedicine Enables the Continuum of Care Through All Medical Echelons
The U.S. military medical echelons of care is a sophisticated, integrated trauma care system for management and evacuation of casualties from point of injury on the battlefield and progressing through increasingly sophisticated levels of care as the casualty is evacuated from the battlefield to the Continental U.S. (CONUS) hospitals. 3 Telemedicine enables this continuum of care from the battlefield all the way back to the peacetime healthcare system. The following echelons of care are described within the context of Army medicine to clarify the operating environment and capabilities available and the challenges and benefits of telemedicine in improving the care of the wounded and others in need of care.
At Echelon 1, point of injury on the battlefield, the primary goal is to stop bleeding and stabilize the casualty for evacuation. First aid and lifesaving measures are performed by trained non-medical personnel, buddy aid, or trained combat lifesaver. Any casualty not able to return to active duty within 24 h will be evacuated to a battalion aid station, where a physician or physician assistant could initiate resuscitation and other advanced trauma life support. If surgical resuscitation is needed, the casualty would be evacuated directly to Echelon 2, where the earliest surgical resuscitation can be performed by a highly mobile Army forward surgical team. At this echelon, there is basic laboratory capability such as radiography. Holding capacity is limited to 72 h, and only 30 medical operations can be performed without resupply. Medical staff of a forward surgical team is a 20-person team that includes an orthopedic surgeon, three general surgeons, two nurses, and additional nursing staff. At Echelon 3, the first large medical facility in theater, also known as a combat support hospital, offers the highest level of medical, surgical, and trauma care available within the combat zone. More sophisticated medical capabilities include laboratory, radiography, blood bank, physical therapy, intensive care unit, and operation tables. Trained medical teams include general surgeons, orthopedic surgeons, thoracic surgeons, vascular surgeons, obstetrician/gynecologist, urologic surgeons, nurses, and physical therapists. Definitive surgical care is offered outside the combat zone at Echelon 4, where patients are held no longer than 72 h before they are evacuated to an Echelon 5 care facility in CONUS (e.g., Walter Reed National Military Medical Center in Bethesda, MD, Brooke Army Medical Center in San Antonio, TX, or the Naval Medical Center in San Diego, CA).
The use of telemedicine is designed to augment communication of medical information among these medical echelons, providing a link and seamless transmission of medical data from the far-forward medical echelons of care all the way up through one of the stateside major military medical centers. 4 For example, all radiology information collected at the first available echelon of care is now transmitted in digital format from the combat support hospital to the major medical center in Germany, providing a seamless transmission of x-rays from the battlefield to the peacetime environment while maintaining the longitudinal electronic health record with the various images representative of the soldier's care on the battlefield. Thus, telemedicine allows the Army to span these hierarchical echelons of care.
U.S.-Based Telemedicine
The U.S. Army Medical Command (MEDCOM) provides command and control of the Army's fixed facility medical, dental, and veterinary treatment facilities as well as preventive care, medical research and development, and medical training. Figure 1 shows the MEDCOM, divided into five Regional Medical Commands. These are responsible for day-to-day operations, including command and control over the medical treatment facilities in their respective regions: Europe Regional Medical Command, Northern Regional Medical Command, Southern Regional Medical Command, Western Regional Medical Command, and Pacific Regional Medical Command. Currently, there are a total of 91 U.S. Army medical sites providing over 60,000 consults per year.
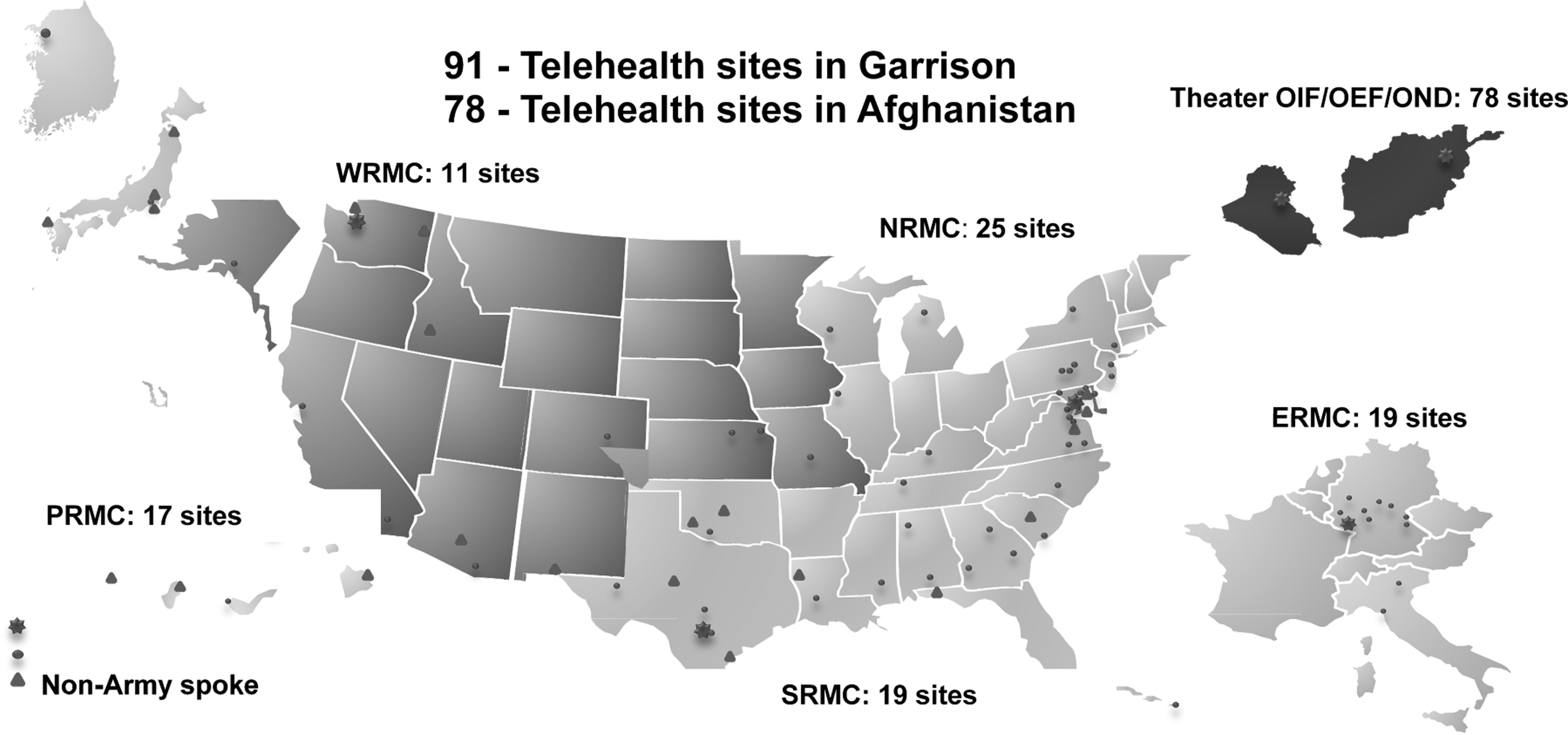
Map showing the division of coverage among the five Regional Medical Commands for the United States. ERMC, Europe Regional Medical Command; NRMC, Northern Regional Medical Command; OIF/OEF/OND, Operation Iraqi Freedom/Operation Enduring Freedom/Operation New Dawn; PRMC, Pacific Regional Medical Command; SRMC, Southern Regional Medical Command; WRMC, Western Regional Medical Command.
The U.S. Army Medical Department Telehealth Network spans 50 countries and territories from America Samoa to Afghanistan, across 19 time zones. 5,6 In total, 22 service lines are available with behavioral health constituting 55% of all telemedicine services, followed by cardiology, teledermatology, infectious disease, neurosurgery, pain management, and orthopedic surgery. Radiology is not counted in these 22 service lines because it is completely digital in the U.S. Army. In fact, it is considered the standard of care, both at peacetime and on the battlefield. Thus, excluding teleradiology, approximately 100,000 telehealth encounters have been conducted in the past 2 years (2010–2011) with the current usage averaging about 60,000 teleconsults per year for 2012. For fiscal years 2010 and 2011, the average was 50,000 each year. Thus, there is increasing overall demand for the use of telemedicine, especially in telebehavioral health. This service includes a variety of clinical programs across all regional medical commands and covering traumatic brain injury, psychiatric, psychology, and neuropsychologic care. 7 –12 The MEDCOM Telehealth Network Initiative that was started in 2008 has grown exponentially and has expanded from about 1,000 tele-encounters a month to over 5,500 per month, from a handful of sites to greater than 90 in Garrison (CONUS, Alaska, Hawaii, America Samoa, Pacific Islands, and Europe) and in Afghanistan from none to over 78. Furthermore, the network has evolved from a state where the Regional Medical Command was not organized and had silo efforts to a network that shares resources across all Regional Medical Commands. It is now working with the Air Force and Navy in sharing ideas and programs.
Using a Web-based secure interface, teledermatology has been active in the CONUS by the U.S. Army since 1994. Currently there are 22 active sites in teledermatology incorporating all three services, the Army, Navy, and Air Force. To date, over 30,000 teledermatology consults have been performed at these various locations, and the Army still accounts for the largest activity at over 75%, compared with the other services. The primary method, a store-and-forward capability, has been in existence for over 15 years. For remote cardiology support in the CONUS, tele-echocardiography using cardiac echo imaging takes place in the central part of the United States, with over 25,000 different consults conducted to date at seven sites. This service relies on contracted cardiologists for interpretation of the results. This well-established process has transitioned over to core funding demonstrating a sustainable business service and is now a model for providing teleconsult care in a peacetime environment on a regular basis.
Telemedicine in Remote Overseas Locations
The application of telemedicine in deployed settings has many challenges, including the limited resources and austerity of the environment in providing medical care in remote regions of the world (Fig. 2). To meet these challenges, the U.S. Army has deployed different types and levels of telemedicine capabilities on the battlefield and at various locations where the soldiers are located. The U.S. Army developed a store-and-forward e-mail with an image attachment system called the “E-mail Teleconsultation Program” that has been implemented worldwide since 2004. This particular program is deemed effective and inexpensive to operate because all the providers use their own digital cameras and rely on the most accessible Internet connection. Since 2004, the average turnaround time for inquiries via e-mail has been 5 h. During the same period, over 10,000 e-mail teleconsults have been completed, involving several different medical specialties. 13 –18 About 43% of all consults were in dermatology, followed by infectious disease as a distant second, then by orthopedics and then neurology. Although the total teleconsultation in Iraq made up the vast majority of consult activity up through December 2011, Afghanistan consult activity is expected to surpass Iraq over the next year since the war in Iraq came to a close in December 2011 for U.S. military forces. Over 54% of the patients using the E-mail Teleconsultation Program are U.S. Army soldiers, with the rest coming from the Marine Corps, Navy, and Air Force. Thus, the teleconsultation program is a triservice effort.

Medicine in deployed zones.
The program includes physicians, nurses, and corpsman in Afghanistan, as well as corpsman on ships at sea and people deployed to Honduras, to the Sinai region, to Korea, and to other places around the globe where anyone within the deployed medical forces has a critical need for reach-back second opinion consultation. No patient-identifiable information is transmitted on the nonsecure, but ubiquitous, electronic network. For example, information transmitted is generally sufficient to make a reliable diagnosis, such as a 24-year-old man with a rash, with some pictures of the rash. For illustrative purpose, a particular case study with digital images sent via e-mail shows an Eveready battery on the neck next to a large fleshy neck mass (Fig. 3) and e-mail text describes the patient as a 50-year-old man with new growth over the last 6 months found on the nape of neck and history of long-term sun exposure. Close-up views of that fleshy mass shows that it turns out to be a malignant melanoma. Without this kind of teleconsultation system readily available in a theater with access to specialty medical care, this soldier may have gone throughout his 6- or 12-month deployment without medical treatment, and this malignant melanoma could have gone undiagnosed with disastrous results.

Digital images sent as e-mail attachments.
The E-mail Teleconsultation Program, also called the U.S. Army AKO Teleconsultation System, provides a continuum of care. It has now been implemented in all 19 medical and 7 dental specialties, including oral maxillofacial and periodontics, with 10,118 teleconsultations completed over 95 months from April 2004 to February 2012. This capability resulted in avoiding unnecessary medical evacuation of some patients from the battlefield with 131 known evacuations prevented during this period. However, most of the time, these teleconsultations facilitated timely and appropriate evacuations on the basis of medical necessity. Often patient safety may be compromised by a false sense of comfort when it is assumed that the problem can be managed locally, in a remote and austere environment, when in actuality the better course of action is to evacuate. During this period, in total, 462 known evacuations were based on the consultants' recommendations. The E-mail Teleconsultation Program also provided 1,153 teleconsultations on non-U.S. patients as well during this same time frame. The availability of an expert second opinion via telemedicine typically resulted in an optimal course of medical treatment given the limited medical resources on site.
To date, the U.S. Army has over 2,500 different providers using the e-mail system with an average turnaround time for each inquiry of about 5 h. Considering the remoteness of many of these sites and the numerous time zone differences among them, the system is well received by deployed providers. Data on average reply times from 2004 through 2012 are shown in Table 1, and percentage usage is shown by specialty, location, and patient branch in Tables 2 and 3.
Overall Average Response Time for Providers Using the E-Mail System for Teleconsultations
E-Mail Teleconsultation Program Summary for Deployed Forces from April 2004 Through February 29, 2012 by Specialty and Service Branch (n=10,118 Consults)
E-Mail Teleconsultation Program Summary for Deployed Forces from April 2004 Through February 29, 2012 by Location (n=10,118 Consults)
Teleradiology is a critical medical capability on the battlefield. The deployable teleradiology systems consist of the Theater Image Repository, which is how the theater images are sent to Landstuhl, Germany. Figure 4 illustrates the concept of digital radiological images transmitted from theaters of operations in Afghanistan to Germany, which then are sent to the U.S. military treatment facilities, following the medical evacuation of the casualty for a sustained continuum of care; similar set-ups are established in Iraq, Kuwait, and Qatar (data not shown). This illustration highlights how digital teleradiology images can be transmitted from any location in a country, including a deployed setting, to the CONUS for interpretation. As of December 2011, teleradiology systems have been established in Iraq with 13 operational sites and in Afghanistan with 22 operational sites. At Landstuhl Regional Medical Center in Germany, the U.S. Army has the ability to archive all radiological images and forward them to the CONUS medical sites on a daily basis. The network in Afghanistan is fully operational, and it is linked with Army facilities in Germany via satellite. The same is true in Kuwait and Qatar. Using the same images from teleradiology, the U.S. Army is able to manage trauma cases and to bundle images from the operating room during the weekly trauma care conferences, which started in October 2011. This capability enriches the discussion of trauma care management for battlefield wounds.
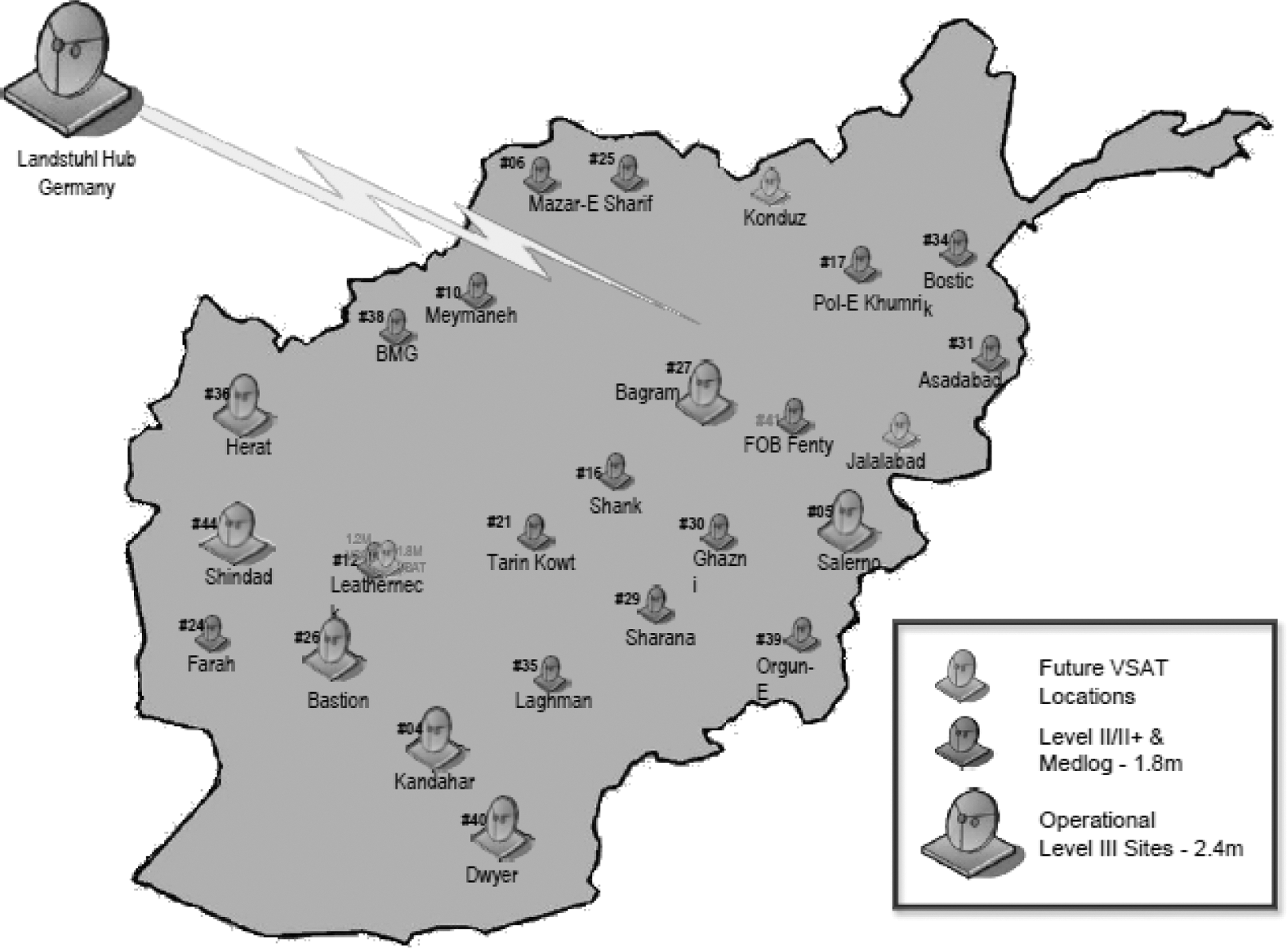
Illustration of Afghanistan teleradiology network sites. VSAT, very small aperture terminal.
A second component of the teleradiology system (i.e., remote diagnostic access) provides for the maintenance of theater computed tomography (CT) scanners. Therefore, the CT scans performed in Afghanistan also use remote maintenance capabilities to detect potential problems with CT scans, and corrective patches are promptly provided from the CONUS to correct the problems. This capability ensures the full functional performance of CT scanners during trauma care.
Currently, telebehavioral health is the largest application in the U.S. Army theater. Long deployments and redeployments of soldiers present serious challenges. Provider shortages are being met with remote providers from other medical regions. Privacy concerns are being addressed with “whisper rooms.” Benefits resulting from implementation of this program include improved access to behavioral health providers for soldiers in need of on-site emergency evaluations. This extends the reach of providers to far-forward deployed locations without incurring significant risk due to travel. It also allows providers at remote outputs to see other patients who are unable to travel. In Afghanistan, for example, there are 78 sites in operation, and another additional 28 sites are planned. Behavioral healthcare in Afghanistan or any deployed setting is augmented with simple and inexpensive telemedicine equipment that enables patients to be evaluated daily regardless of operational tempo or inclement weather that may interfere with patient or provider movement. The U.S. Army Medical Department has established a secure network across the battlefield to link patients and providers on the hilltops with behavioral health capabilities. 19 This system extends the reach of providers, enabling them to reach out to patients who need immediate help, overcoming distance, inclement weather, and/or other constraints. For example, in Afghanistan the far-forward telebehavioral health consultation consists of an inexpensive laptop, a Web camera, a head-mounted microphone, and a receiver where the patient can have private conversations with his or her provider (Fig. 5). Typically, the provider has two computer screens: one to enable a video interaction with the patient in real-time, and the other to document the encounter in the electronic health record. The most recent telebehavioral health information technology solution consists of a small camera resting on top of a laptop or monitor and new bridges installed to support conference calls with an on-screen awareness capability at a unit cost of $355. Surveys conducted by the U.S. Army Public Health Command documented high satisfaction among providers, patients, and commanders. Furthermore, it was shown that greater than 70% of the behavioral health encounters would not have occurred if telebehavioral health was not available. 20
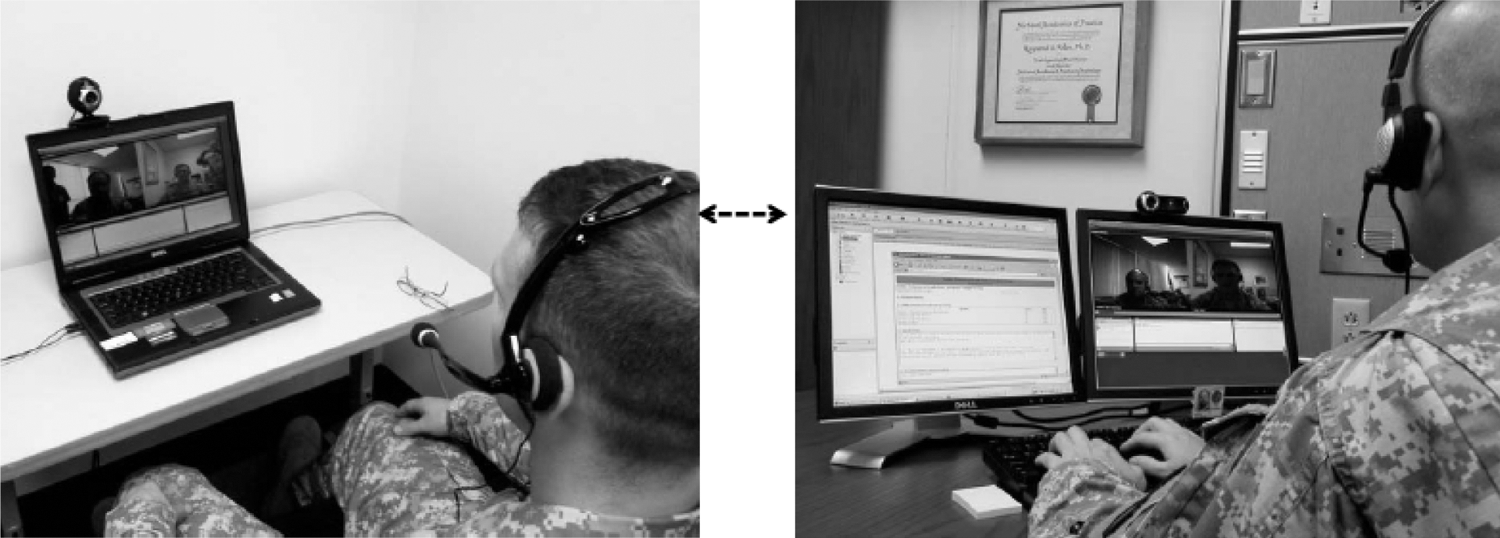
Typical set-up for telebehavioral consultation.
The Telemedicine and Advanced Technology Research Center at the U.S. Army Medical Research and Materiel Command has embarked on the deployment of mobile communication systems to facilitate remote care, referred to as m-health. This application is divided into three domains: theater, garrison-based, and global.
At the garrison level, the focus is on cellular phones to help returning service men and women manage their medical care while at home. This will be part of the patient-centered medical home in an accountable-care-like organization. These new patient-centered medical home will offer a variety of medical services such as pain management and behavioral health consultation as well as other electronic capabilities such as e-prescribing/refills and e-appointing/scheduling. This will entail mobile applications on the cellular phone that enable patients to manage their own care.
The most important feature of the garrison-based cellular phone application is improved contact between recovering wounded soldiers in their home locations and their geographically remote case managers. This application is HIPAA-compliant and user friendly. It provides patients with appointment reminders, unit announcements, and health tips, while allowing them to store healthcare information on their own phones. The system provides access to a Web portal, where patients can update case managers on their progress and review their feedback. Since its deployment in early 2010, more than 600 users in 28 states and the District of Columbia have received healthcare services across distances of over 600 miles. From August 2009 to April 2012, more than 300,000 secure messages were transmitted, and over 5,000 unique patient appointments were scheduled using the soldier's personal cellular phone following implementation of the mCare program. 21
The use of cellular phones is widespread globally, and their applications for improving health and humanitarian response among foreign nations will be an important tool for the U.S. Army as its role in medical stability operations develops. 22,23 Capabilities for enabling global health management of an individual or population using mobile devices will become critical for future NATO and U.S. military operations, and the capabilities continue to evolve. 24,25
There exists a need to integrate the m-health capability with the electronic health record in order to enable clinical consultation over a mobile device with the requisite documentation in the electronic health record. Technology advances in the areas of wearable physiological sensors or “smart bandages” with the smartphone will be an important enabler for home telehealth, especially for chronic diseases. The smartphone has opened up the potential for improving health outcomes, empowering the patient, providing the clinician or researcher with mobile education and research, and assisting in biosurveillance and disease management (Fig. 6).
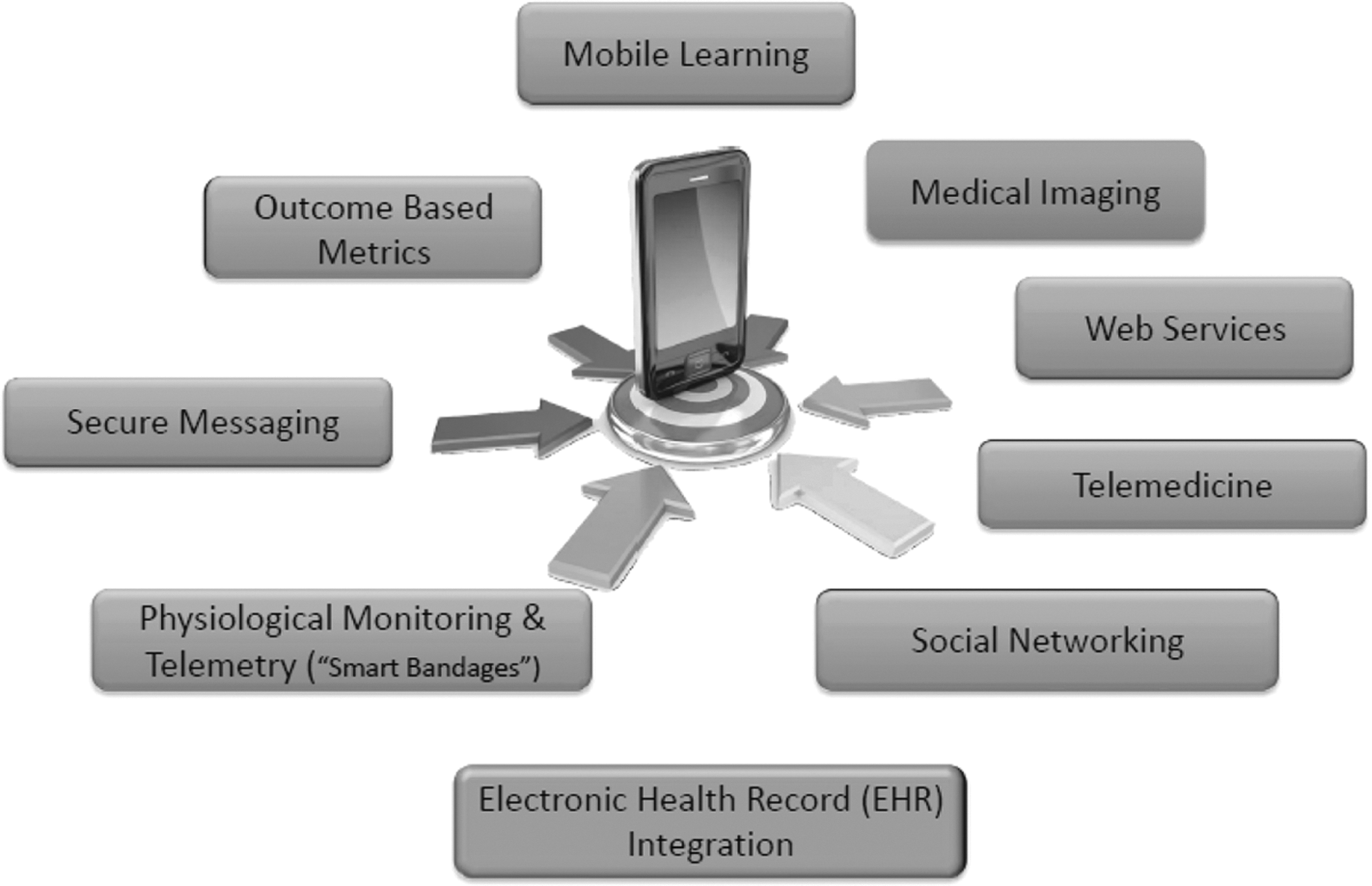
Illustration of mobile health capabilities in a smartphone.
Summary
In brief, the U.S. Army and Telemedicine and Advanced Technology Research Center, in particular, have adopted the use of telemedicine capabilities for both peacetime and remote settings. The specific technology now entails the use of mobile devices capitalizing on the increased sophistication and ubiquity of cellular phones, thereby empowering individuals to manage their own care irrespective of geography or time constraints.
Footnotes
Acknowledgments
We thank Dr. Rashid Bashshur, Director of Telemedicine at the University of Michigan Health System for organizing the Ann Arbor Telemedicine Symposium, bringing together a diverse group of leaders in the field to exchange best practices and emerging concepts.
Disclosure Statement
No competing financial interests exist.