
Abstract
This article describes the evolution, current status, and future prospects of the Ontario Telemedicine Network (OTN). Started in the late 1990s (and formally established in 2006), OTN is a not-for-profit corporation primarily funded by the Government of Ontario, Canada, that aims to improve access to and quality of care throughout the Province. It covers a land mass larger than France and serves a population of just over 13 million, the vast majority of which live in a narrow strip close to the U.S. border. Telemedicine has been effective in reducing travel to usual sources of care, reducing hospital admissions, and improving efficiency and prompt access to care. The diffusion of telemedicine is accelerating in Ontario, and it is becoming an integral part of the health system.
Introduction
Ontario is a large province in Canada (Fig. 1), consisting of 415,000 square miles and containing a population of more than 13 million. The vast majority of this population, more than 12 million, lives in a narrow strip within 100 miles of the U.S. border in the more urban south. The remaining population (less than 1 million) is widely scattered across the vast north in a land area larger than that of France. Telemedicine was adopted to meet healthcare needs of the resident population of Ontario in this challenging geography.
A map of Ontario.
Telemedicine in Ontario began in earnest in the late 1990s with the goal of improving access to care while reducing travel for those seeking healthcare. Over the years, telemedicine services have been extended to urban areas where there was a need to improve the quality and efficiency of healthcare delivery. The Ontario Telemedicine Network (OTN) (Fig. 2) is the result of a merger of three independent regional networks that was formally established in 2006 with the active support of the provincial government and with the goal of serving the entire population of Ontario.
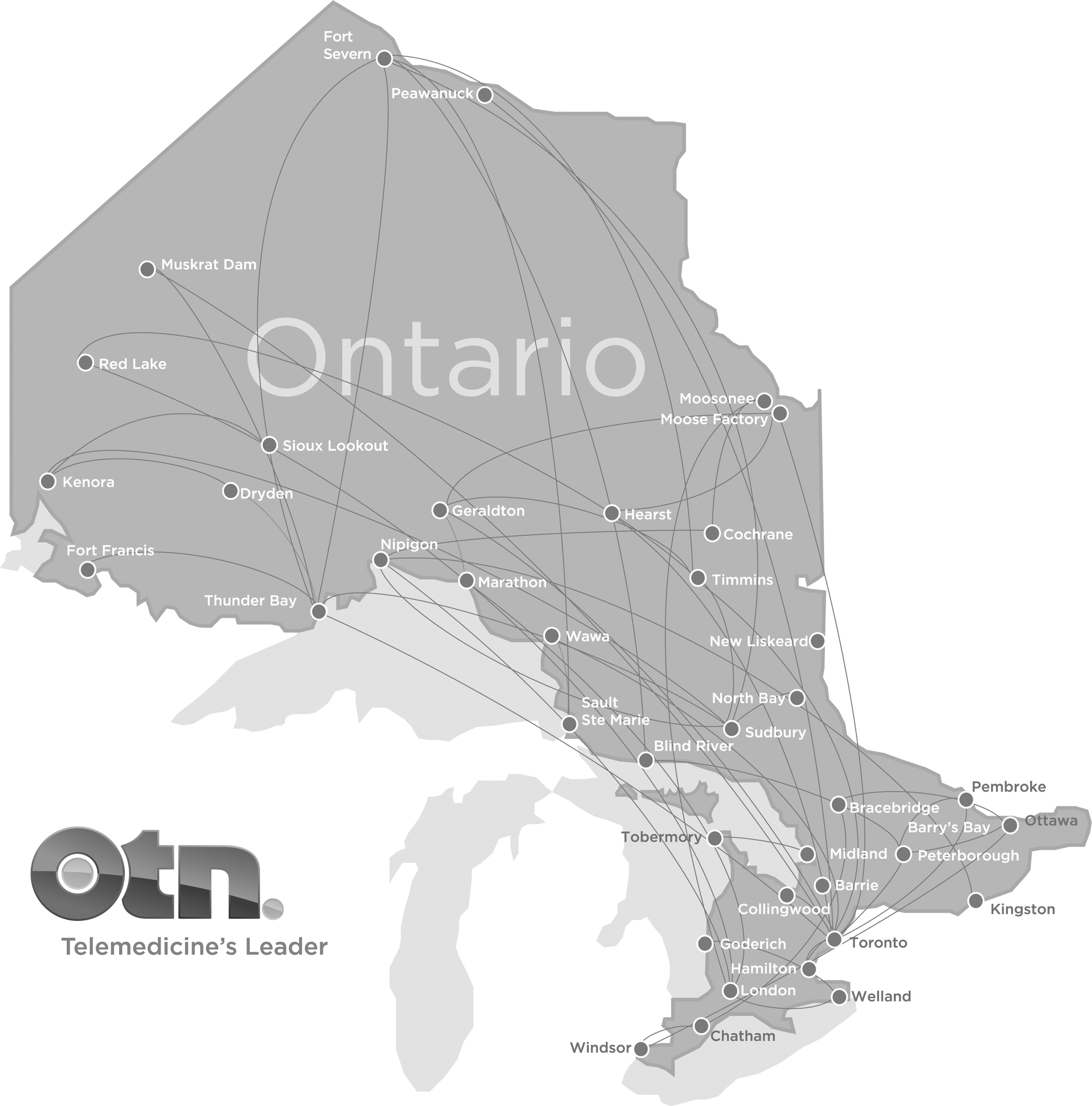
The area served by the Ontario Telemedicine Network and its partners.
OTN is a not-for-profit corporation operating in the Province of Ontario. Its mission is “to develop and support telemedicine solutions that enhance access and quality of healthcare in Ontario, and inspire adoption by healthcare providers, organizations, and the public.” OTN's stated vision for the future is “Telemedicine will be a mainstream channel for healthcare delivery and education.”
OTN System, Service Population Characteristics, and Activity Volume
In Fiscal Year (FY) 2011–2012, OTN supported telemedicine at 1,463 hospital and healthcare sites equipped with 2,630 videoconferencing systems sites across the province. These facilitated 204,058 patient telemedicine consultations.
Services were provided by 1,685 consultants in nearly every therapeutic area of care. The most frequent services provided were mental health and addictions. Together, they accounted for over one-half of all telemedicine encounters, followed, respectively, by internal medicine, oncology, and surgery. In addition to clinical activity, OTN supported 13,965 educational events and 16,523 administrative events (meetings). Growth in clinical activity in 2011–2012 over the previous fiscal year was 52%. This compares with an average growth rate of approximately 30% in the preceding 3 years. In the first two quarters of FY 2012–2013, growth has been more than 100% (double) of the activity seen in the same time period in the previous year, indicating a substantial acceleration in utilization. These figures do not include activities such as telehomecare (remote monitoring), which supports patients with significant chronic disease. OTN has been supporting telehomecare since 2007, and it is currently expanding this program.
There are numerous programs in a wide variety of clinical areas across the province. Some are local, and some are regional or province-wide. Additionally, there are several emergency services, including a well-established province-wide emergency telestroke program, a provincial teleburn initiative, and regional programs for mental health crisis, critical care, and trauma. Store-and-forward technologies are used to support active teledermatology and teleophthalmology programs.
The Role of Telemedicine
OTN does not deliver any direct clinical services on its own. Rather, OTN supports and facilitates telemedicine delivery by its organizational and individual provider members who use it to support their patients and their business needs. Thus, the role of OTN is limited to providing support for the adoption of the core technologies and services that enable telemedicine. More specifically, this role consists of the following: • Supporting adoption. OTN provides account management, change management, and business planning support for health providers, organizations, payers, government programs, and others who wish to incorporate telemedicine into their activities. • Technologies. Technologies used to deliver clinical care include videoconferencing, various medical devices, and store-and-forward technologies. Nonclinical events (such as educational programming) primarily use multipoint videoconferencing, webconferencing, and webcasting technology. Personal computer videoconferencing services were introduced in FY 2011–2012. Telehomecare uses remote monitoring devices and supporting software. Normally, OTN member providers and organizations provide their own end devices, with OTN providing the core infrastructure and applications, which are housed in mirrored redundant data centers. The network is usually provided by the member, although OTN also supports a large private network that extends to about 700 sites. • Services. Besides providing support for the delivery technologies, OTN provides several key services whose aim is to simplify the use of telemedicine for its users. These include “turnkey technology” support, provisioning, training, scheduling, referral management, and privacy/security support. These services are supported by key secure online applications such as directories, learning centers, and scheduling and referral management services whose aims are to assist users in finding the resources they need and to organize collaborative activities among the parties. The online service is a combination of third-party and proprietary applications that have been developed over the past 7 years.
The OTN Business Model
As previously explained, OTN does not deliver clinical services directly to patients, but aims to make it simple and efficient for OTN's member organizations and providers to do so.
Any organization or provider connected to the healthcare system who wishes to use OTN's services must become a member. Members are required to sign a collaboration agreement that spells out the service level agreement with OTN as well as other conditions to which the member agrees to adhere. Most important is that the member must agree to follow technical standards, business process standards, and privacy/security best practices.
Through this common agreement, many diverse and independent organizations and providers can use the same infrastructure, while accessing only the services they need and collaborating only with the partners they choose without disruption from other parties.
This model has enabled a large and diverse user base. In FY 2011–2012, this included all of the 155 hospitals in the Province as well as: • 65 community care access centers • 62 specialist clinics • 71 clinician offices • 72 community health centers • 111 community support services • 25 educational facilities including medical and nursing schools • 125 primary care teams • 94 long-term care facilities • 335 mental health/addictions agencies • 28 nursing stations on aboriginal reserves (in collaboration with Keewaytinook Okamakanak Telemedicine Network) • 14 professional organizations • 55 public health unit and regional infectious disease units • 14 regional health offices • 15 rehabilitation facilities • 13 federal and provincial prisons.
Using this model, the process of adding new members is accelerating at a fast pace. In FY 2011–2012, for example, 268 organizations joined OTN and 434 videoconferencing systems were added to the network. OTN is primarily funded by the Ontario provincial government through the Ministry of Health and Long-Term Care (MOHLTC). The MOHLTC funding supports membership for any organization that receives more than 50% of its annual revenue from the MOHLTC, as well as for physicians. Besides membership fees, OTN also receives revenue from site and system installations and from a variety of premium services such as complex event management and studio rentals. OTN has a collaboration agreement with Keewaytinook Okamakanak Telemedicine that enables the seamless provision of telemedicine services to many rural and remote First Nations Reserves. Canada Health Infoway, a federal agency established to promote e-health development in Canada, has provided funding for several significant developmental projects over the past 6 years.
Impact of Telemedicine
OTN collects a significant amount of empirical program data and performs periodic surveys and focus groups. Some examples that may be of interest are outlined below.
TRAVEL
• In FY 2011–2012, an estimated 130 million miles of travel was avoided as a result of patients using telemedicine instead of traveling to their usual source of care. This is the equivalent of traveling around the world at the equator 5,150 times. An estimated 23 million liters of fuel (approximately 6.1 million U.S. gallons) were saved, potentially avoiding 57 million kg (approximately 63, 000 tons) of carbon pollutant.
• In Northern Ontario, the provincial government subsidizes travel for healthcare for the approximately 1 million residents in the region. Through the use of telemedicine, it is estimated that the government avoided spending $C 45 million in travel costs in FY 2011–2012.
PATIENT SATISFACTION
• Of 791 patients who responded to a 2012 survey (response rate of 80%):
∘ 92% indicated they were satisfied with their telemedicine visit.
∘ 91% of respondents indicated they would use telemedicine again.
∘ 87% felt as comfortable receiving care through telemedicine as they would have in person.
∘ 82% felt it was more convenient to see the provider by telemedicine than in person.
∘ 74% indicated they saved money using telemedicine, with a calculated average savings of $C 242.
Hospital Admission Reduction
• Self-reported data from 441 congestive heart failure and 377 pulmonary disease patients enrolled in OTN's Phase One Telehomecare Program demonstrated a reduction of over 60% in hospital admissions and over 70% in emergency department visits.
• A regional mental health crisis program using telemedicine demonstrated a 75% avoidance in hospitalization rates for patients managed through the program.
Efficiency and Improved Access
• Evidence from focus group discussions suggests the perception of greater efficiency by providers. For example, several ophthalmologists reported that they can assess and manage patients in less than half the time of similar assessment in-person using store-and-forward technology. Clinicians in Mental Health Assertive Community Treatment Teams reported saving at least 80 min of travel each day.
• The average appointment waiting time for a dermatology consultation in some regions was reduced from months to 5–10 days.
• An estimated $3.5 million (U.S./Canadian dollars are nearly at par) in health system costs were avoided because of a decrease in hospitalization and nursing home care through the delivery of 2,378 telestroke consultations resulting in the safe and timely administration of tissue plasminogen activator for 722 patients.
Looking to the Future
Proponents of telemedicine frequently refer to the “promise of telemedicine” and moving telemedicine to the “next level.” OTN's experience appears to indicate that the diffusion of telemedicine is accelerating rapidly and is en route to reaching the next level—becoming an everyday part of the health system in the Province. Ontario residents appear to be quite receptive to telemedicine, and with the relative ubiquity of computing and particularly smartphones and tablet devices throughout Ontario, providers appear to have entered a new state of mainstream readiness.
As OTN is both a catalyst for telemedicine and a service provider, its role is to continue to provide leadership towards the adoption of telemedicine and to continue to simplify its use for institutions, providers, and patients. This will involve further simplification by OTN in the matters of collaboration among providers, accelerating integration with electronic medical records and lowering the cost of telemedicine technology. The latter will include leveraging lower-cost consumer devices and mobile platforms.
Health system policy and regulation are still not entirely considerate of telemedicine. It would appear that lawmakers and payers in most provincial, regional, and local jurisdictions now understand this, and telemedicine policies and legislation are being adopted at a steady pace. Finally, there is the new frontier of personal digital healthcare, which will leverage remote monitoring further, with advanced capabilities, massive analytics, and other applications to connect patients in the community with their healthcare delivery providers. Digital mobile technology is already creating a new wave of unprecedented opportunities to improve and personalize healthcare. Many innovative ideas are being tested and implemented. It will be exciting to see the practical clinical and business models that develop around these technologies and to see which ones become drivers and mainstream elements of transformed healthcare systems.