
Abstract
Introduction
Access to subspecialty services is one of the challenges faced by patients and clinicians practicing in rural communities. 1 –5 Telemedicine, the use of electronic information and communication technologies to provide healthcare over a distance, 6 has been used to address this challenge for over 10 years. 4 –9 There have been previous reports of high satisfaction and perceived high quality of care in pediatric patients receiving pediatric critical care telemedicine consultations in remote emergency departments (EDs) and adult intensive care units (ICUs). 4,10,11 It has also been shown that telemedicine evaluation has good concordance with in-person evaluation of pediatric patients. 12,13 However, the effectiveness of telemedicine systems for pediatric critical care evaluation has not been thoroughly assessed.
In 2007, Doernbecher Children's Hospital (a tertiary hospital) at Oregon Health and Science University, Portland, OR, partnered with Sacred Heart Medical Center (a community hospital) to create a pediatric critical care telemedicine consultation program. Approximately 1 year after the implementation of the telemedicine program, the community hospital implemented a hospitalist system to assist in the management of inpatient pediatric patients. In this study, we sought to assess the additive impact of the telemedicine program and the hospitalist system on the pediatric patients cared for at the community hospital. We hypothesized that implementation of a telemedicine program for pediatric intensivist consultation and a hospitalist program for community hospital inpatient pediatric care would improve the identification of patients requiring continuing care in an intensive care unit, thus decreasing the rate of transfer to higher levels of care.
Patients and Methods
Sacred Heart Medical Center is located in the Eugene–Springfield metropolitan area (population 351,715), the second largest city in Oregon. During the first 2 years of our study period, Sacred Heart University District Hospital had 104 beds (10 pediatric beds). In August 2008, the newly built RiverBend Hospital replaced Sacred Heart University District Hospital for many services, including inpatient pediatrics. RiverBend Hospital is a Level II trauma center with 386 beds (16 pediatric beds). In addition to board-certified pediatricians and emergency physicians, there are pediatric surgery, infectious disease, and orthopedic surgery specialists available for consultation and care of pediatric patients at the community hospital.
Doernbecher Children's Hospital is a 128-bed pediatric hospital with 20 pediatric intensive care beds in Portland (population 583,776); it is one of only two pediatric subspecialty referral centers in Oregon. In April 2007, a telemedicine program was established between the ED and pediatric ward at the community hospital and the pediatric ICU (PICU) at the tertiary hospital, which are approximately 110 miles apart.
The telemedicine program consists of real-time two-way audiovisual conferencing between the facilities conducted over medical-grade videoconferencing carts. The consulting intensivist has control of the remote camera, allowing full vision around the patient room with excellent resolution even when zooming (e.g., for a pupillary exam). At the conclusion of the telemedicine encounter, a standard consultation form is completed by the intensivist and faxed to the community hospital physician for inclusion in the patient chart. All consulting pediatric intensivists are attending physicians with board certification in pediatric critical care medicine and have physician privileges at the community hospital.
Telephone consultations are initiated when the community hospital physician calls the tertiary hospital's consultation line; they are then connected with the pediatric intensivist. After implementation of telemedicine, telephone consultation was still utilized on a case-by-case basis at the discretion of the referring physician.
At any time after consultation, the patient may either be transferred to the tertiary hospital or continue care at the community hospital. The decision to transfer is a joint clinical decision made by the critical care and community physicians. Most of the patients transferred to the tertiary hospital are transported with a pediatric transport team that is employed by the tertiary hospital. The pediatric transport team consists of a registered nurse and respiratory therapist that are specialty-trained for neonatal and pediatric transport. They act under the supervision of the attending pediatric intensivist and have standard protocols for commonly encountered illnesses such as diabetic ketoacidosis and asthma. After arriving at the community hospital and assessing the patient, the transport team contacts the pediatric intensivist with an update regarding the current status of the patient. At that time or any other time during transport, the transport nurse may suggest that the patient is suitable for the ward based on his or her clinical assessment. If the intensivist agrees with this recommendation, then the patient is admitted to the pediatric ward instead of the PICU upon arrival at the tertiary hospital.
The pediatric hospitalist program at the community hospital was instituted in July 2008. This program is a model in which a core group of community pediatricians are dedicated to hospital duties with no outpatient responsibilities. There are two pediatric hospitalists covering the hospital 24 h/day in an overlap fashion to facilitate patient handoffs. The day hospitalist provides in-house care and generally works several days consecutively to maintain continuity of care. The night hospitalist is in-house until 8 p.m. and then takes home call, returning to the hospital for all admissions and at the request of nurses in response to changes in patients' clinical status. All hospitalists are board-certified in Pediatrics. Prior to July 2008, pediatric patients admitted to the community hospital pediatric ward were cared for by their primary care physician (either a pediatrician or family medicine physician) in a traditional model. All emergency physicians at the community hospital are board-certified in Emergency Medicine; none has additional pediatric training.
This was a retrospective chart review of community hospital pediatric patients receiving critical care consultations from the tertiary hospital over three time periods. Patients were identified from consultation logs capturing some telephone consultations and most telemedicine consultations and transfer logs capturing all patients transferred from the community hospital to the tertiary hospital. It was approved by the PeaceHealth and Oregon Health and Science University Institutional Review Boards. Informed consent and Health Insurance Portability and Accountability Act authorization were waived. All data was de-identified and collected onto approved data collection sheets.
Subjects for this study included pediatric patients (<18 years old) for whom the community hospital physician consulted the tertiary pediatric critical care physician between January 2006 and October 2009. Patients with consultations originating in the month of July 2008 were excluded, as there was a facility move from Sacred Heart University District Hospital to RiverBend Hospital during this time period. Non-critical care consultations (e.g., cardiology, oncology) were excluded. Consultations originating from the pediatric ward were initiated by the primary physician or the hospitalist, depending on the time period of consultation. Consultations originating from the ED were initiated by the ED physician. Consultations from the neonatal ICU, adult ICU, and operating room were initiated by the physician with primary responsibility for the patient (e.g., the neonatologist, intensivist, or surgeon or anesthesiologist, respectively). Comparison groups were divided into three cohorts based on the modality of intensivist consultation (telephone versus telemedicine) and modality of inpatient ward care at the community hospital (primary care physician versus hospitalist).
Patient Cohorts
Cohort 1 consisted of 41 community hospital pediatric patients receiving pediatric intensivist telephone consultation in the 15 months prior to the implementation of the telemedicine system (January 2006–March 2007). All consultations were conducted via telephone. Pediatric inpatient care at the community hospital was by the patients' primary care physician.
Cohort 2 consisted of 56 pediatric critical care consultations from April 2007 to June 2008, which was after the implementation of the telemedicine program for consultation with pediatric intensivists but prior to implementation of the pediatric hospitalist program for community hospital pediatric inpatient ward coverage. Consultations were conducted via telephone or telemedicine at the discretion of the referring physician. All community hospital inpatients were cared for by their primary care physician.
Cohort 3 consisted of 56 pediatric critical care consultations in the 15 months after implementation of the pediatric hospitalist program at the community hospital with telemedicine consultation availability (August 2008–October 2009). Consultations were conducted by either telephone or telemedicine at the discretion of the referring physician. Inpatients on the community hospital pediatric ward were cared for by pediatric hospitalists.
Data
Demographic data, reason for consultation, final diagnosis, lengths of stay, Pediatric Risk of Admission II (PRISA II) scores, 14 and Pediatric Risk of Mortality III (PRISM III) scores 15 were abstracted by chart review. Also noted was whether or not the patient was transferred to the tertiary hospital and, if transferred, to which ward (tertiary pediatric ward or PICU) he or she was transferred. Transfer diagnosis discrepancy, defined as a difference between the transfer diagnosis and discharge diagnosis, and rate of transfer were determined from the data. The proportion of transferred patients who were admitted to the tertiary ward versus PICU was determined and used as a potential measure of appropriateness of triage (e.g., those transferred to the tertiary ward potentially could have stayed at the community hospital).
Our primary analyses compared data among cohorts. Secondary analyses were done to compare those patients who received telephone consultation with those who received telemedicine consultation after implementation of the telemedicine system (Cohorts 2 and 3).
Statistics
Descriptive statistics were used to describe demographic and diagnostic data. Continuous variables were analyzed using Bartlett's analysis of variance and one-way analysis of variance when comparing the means from the three cohorts with each other. Student's t test was used for comparisons of individual means. Pearson's chi-squared test was used to analyze categorical variables. Statistical significance was determined at p<0.05.
Results
Table 1 summarizes demographic, diagnostic, and physiologic data for the three cohorts. Baseline data were similar among groups. Median age was 2 years (range, 2 days–17 years). Mortality rates were similar among cohorts; no demographic or physiologic parameters were significantly different among cohorts. There was a trend toward higher mean PRISA II scores in Cohorts 2 and 3 compared with Cohort 1 (18.1, 23.7, and 22.8 in Cohorts 1–3, respectively; p=0.06). There were differences in the reason for consultation among cohorts that did not reach statistical significance.
Demographic, Diagnostic, and Physiologic Data Among Cohorts
Data are mean±standard deviation values or number (%) as indicated.
Only includes patients transferred to the pediatric intensive care unit.
Operating room, adult intensive care unit, or neonatal intensive care unit (telemedicine not available).
Only includes patients transferred to the tertiary hospital.
ED, emergency department; PRISA, Pediatric Risk of Admission; PRISM, Pediatric Risk of Mortality.
In total, 155 community hospital patients received pediatric critical care consultation from January 2006 to October 2009. Two patients were excluded because of consultation during the month of a facility move for the community hospital. Cohort 1 consisted of 41 community hospital patients receiving critical care consultation, all of whom received telephone consultation. Cohort 2 consisted of 56 patients, of whom 44.6% received telemedicine consultation with the remainder receiving telephone consultation. Cohort 3 consisted of 56 patients with 53.6% receiving critical care consultation via telemedicine. Figure 1 illustrates the disposition of patients by cohort and mode of consultation.

Cohort flow diagram. PICU, pediatric intensive care unit.
Table 2 summarizes outcomes of consultation in the three cohorts. The rates of transfer were lower in Cohorts 2 and 3 with 85.7% and 87.5% transferred, respectively, compared with a 100% transport rate in Cohort 1 (p=0.04). When independently compared (Supplementary Table S1; Supplementary Data are available online at
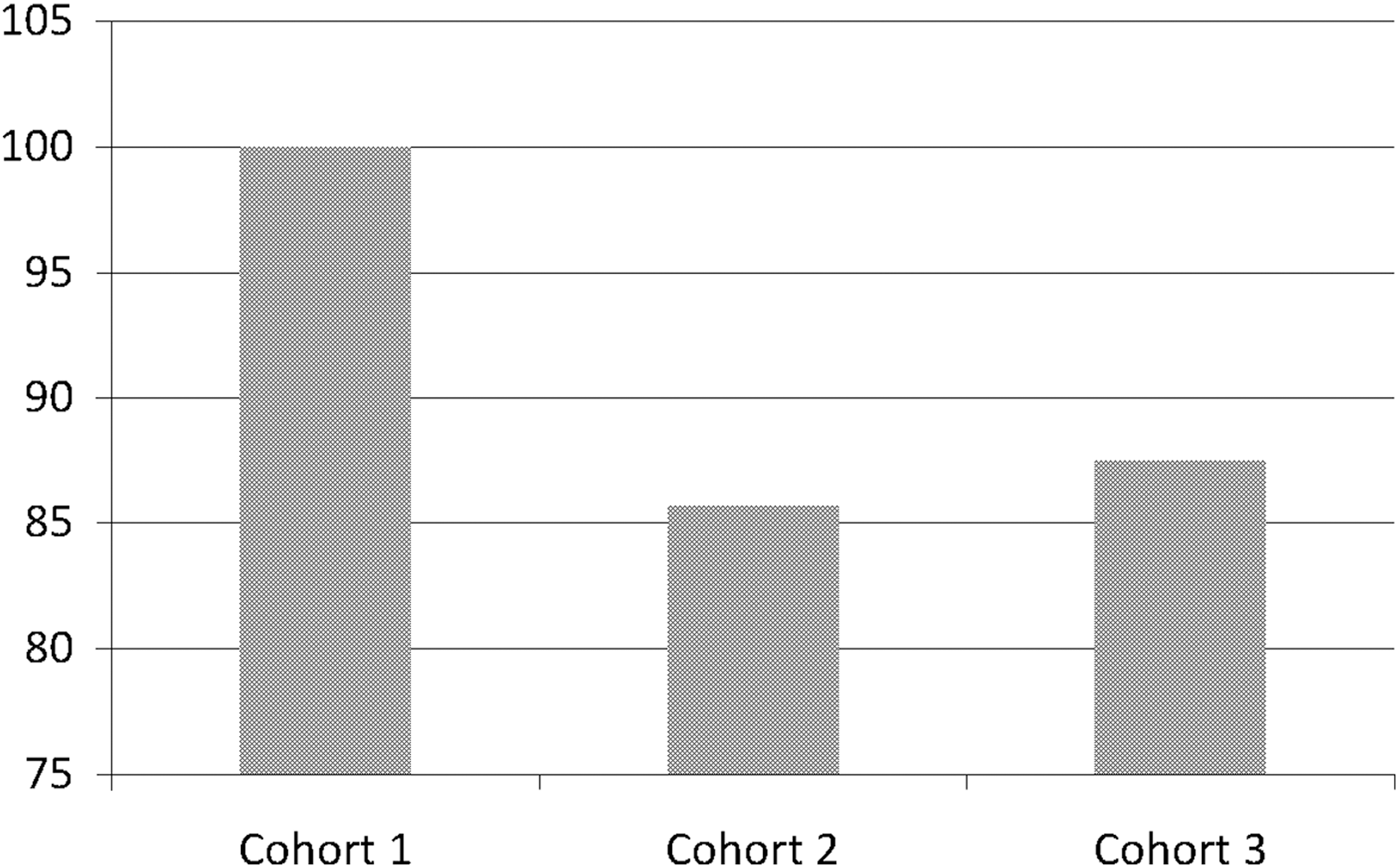
Rates of transfer by cohort (percentage of all patients).
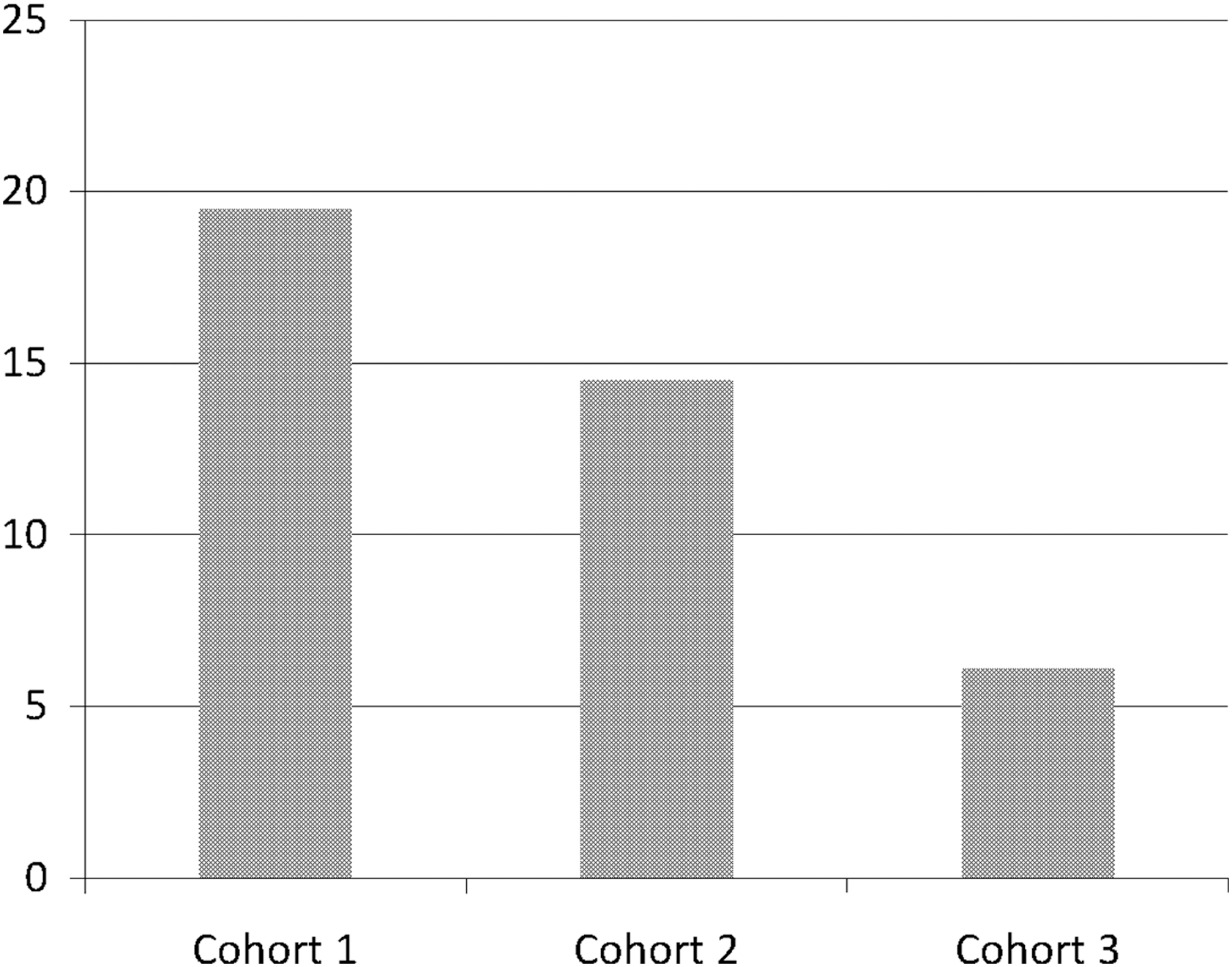
Rates of diversion to the tertiary ward by cohort (percentage of transferred patients).
Outcomes Among Cohorts
Data are number (%) or mean±standard deviation values as indicated.
Data available only for transferred patients.
PICU, pediatric intensive care unit.
Because telemedicine was not exclusively utilized after its implementation, we further analyzed Cohorts 2 and 3 based on whether or not patients had received telephone or telemedicine consultations. If a patient received telemedicine consultation at any time (e.g., initial consultation was via telephone and subsequently follow-up was via telemedicine, or vice versa), it was categorized as a telemedicine consultation. The results of this subanalysis are summarized in Table 3. There was no difference in age, gender, race, or ethnicity among the groups. Of those with telemedicine consultations, 72.7% were transferred with 7.5% diverting to the tertiary ward, while all patients receiving telephone consultations were transferred with 12.3% diverting to the tertiary ward (p<0.001). The reason for consultation differed, especially in the categories of trauma, respiratory distress, and sepsis, with more trauma consultations in the telephone group and more respiratory distress and sepsis consultations in the telemedicine group (p=0.003). The majority of telephone consultations came from the ED (64.9% and 34.9% from the ED and ward, respectively; p<0.001). Consultations from the operating room, neonatal ICU, and adult ICU all used telephone communication as telemedicine was not available in those units.
Demographic, Diagnostic, Physiologic, and Outcomes Data Based on Mode of Consultation Used in Cohorts 2 and 3
Data are number (%) or mean±standard deviation as indicated.
Data available only for transferred patients.
Only includes those transferred to the pediatric intensive care unit (PICU).
Operating room, adult intensive care unit, or neonatal intensive care unit (telemedicine not available).
ED, emergency department; PRISA, Pediatric Risk of Admission; PRISM, Pediatric Risk of Mortality.
Discussion
This study demonstrated that a PICU-based telemedicine program can provide interactive consultation to a remote referring community hospital for the stabilization of pediatric patients. After the implementation of the pediatric critical care telemedicine consultation program, both the rate of transfer and diversion of transfers to the tertiary hospital ward decreased. The additional implementation of a pediatric hospitalist program in the community hospital further improved triage of patients requiring critical care, as demonstrated by the reduction in the number of patients diverted from the PICU to the tertiary ward. Based on the presence of these programs, some unnecessary transfers were likely avoided.
Telemedicine is increasingly being used to provide care to patients in geographical areas that do not have access to subspecialty care. 5,16 In the outpatient setting, telemedicine can prevent unnecessary lengthy travel for families requiring subspecialty consultation. 5,7,8 In the inpatient setting, several studies have demonstrated improved outcomes with oversight of adult ICU patients by a remote intensivist using telemedicine. 17 –19 Pediatric literature has reported improved mortality when telemedicine is used for critical care consultation on pediatric trauma patients cared for in adult ICU settings. 20 In addition, there have been multiple studies showing high satisfaction of both providers and families with the use of telemedicine for inpatient and ED pediatric critical care consultation. 4,11,20,21 Ours is the first study demonstrating the ability of telemedicine to improve triage of critically ill pediatric patients and enable a proportion of patients to remain at the referring hospital, thus avoiding lengthy, costly, and potentially dangerous transports.
The primary limitation of this study was the manner in which telephone consultations were identified. Patients receiving consultation in the 15 months prior to piloting the telemedicine system were logged at the community hospital as part of the pilot project; we used this log to identify Cohort 1 patients. However, there was no such log of telephone consultations in Cohorts 2 and 3; therefore, we relied solely on transfer records to identify patients receiving telephone critical care consultations, thus limiting our ability to capture advice calls from the community hospital that did not result in transfer of care. As there are no call logs documenting telephone consultation on patients who remained at the community hospital, it is likely that we have overestimated the actual transfer rate for this population in Cohorts 2 and 3. Because of this limitation, we cannot fully interpret the difference in transfer rates between consultations using telemedicine and telephone in Cohorts 2 and 3. However, there was a decrease in transfer rate after the implementation of telemedicine that is not negated by the fact that there may have also been a decrease in transfer rate of patients receiving telephone consultations. In addition, it is reasonable to presume that most critical care consultations via telephone result in transfer of the patient as Cohort 1 had a 100% transfer rate.
It is notable that in Cohort 2, a similar proportion of patients diverted to the tertiary ward in the telephone and telemedicine groups (Fig. 1). The reason for this difference is unclear, as the overall rate of diversion decreased from Cohort 1 to Cohort 2. It is possible that the high rate of diversion in the telemedicine group of Cohort 2 might be explained by the time it takes personnel to become familiar with a new system after its implementation. In Cohort 3, the diversion rate is further decreased, making it unlikely that the decrease in diversion rate over time is coincidental. As the diversion rate of patients receiving telemedicine consultations in Cohort 3 is zero, it is improbable that the decreased diversion rate across cohorts is solely attributable to the implementation of the hospitalist program. It is likely that the improved triage of patients was due to the combination of the telemedicine and hospitalist programs. Additionally, when individually compared, the decreased diversion rate was only statistically different between Cohorts 1 and 3. This may be due to insufficient sample size, as the power of this study was calculated to detect a difference in transfer rate, not the diversion rate.
The results of this study show that critical care telemedicine consultations coupled with a pediatric hospitalist program have the potential to improve triage of critically ill children in outlying hospitals and reduce the need to transfer patients to a higher level of care. This has important implications, as unnecessary transfers were able to be avoided, allowing families to remain closer to their homes and support systems. This system also has the potential to reduce costs by reducing expensive and sometimes risky transports. Our study was not designed to investigate cost-effectiveness; future research should be directed toward examining cost savings from reduced transport compared with costs of the telemedicine and hospitalist programs.
Conclusions
Based on our review of patients before and after the implementation of a telemedicine partnership between a community non-pediatric hospital and a tertiary PICU, telemedicine critical care consultations combined with a pediatric hospitalist program at the community hospital have the potential to reduce the unnecessary transfer of patients to a higher level of care by improving triage of those patients requiring critical care. The potential cost-effectiveness of telemedicine consultation and pediatric inpatient hospitalist care systems should be the focus of future research.
Footnotes
Acknowledgments
We would like to acknowledge Mark Lovgren, Danielle Williard, and Jan Freitas-Nichols at Oregon Health and Science University–Doernbecher Children's Hospital for technical support with the telemedicine program. We would like to acknowledge the Jackson Foundation, the Friends of Doernbecher, and the Charlotte Coleman Frey Fellowship fund for financial support of the telemedicine equipment, telemedicine program, and travel related to this research. We would also like to acknowledge Dan Reece at Sacred Heart Medical Center RiverBend for his assistance with access to patient charts and navigating the computer system.
Disclosure Statement
J.M.L. received approximately $800 for travel expenses related to this research project from the Charlotte Coleman Frey Fellowship Fund. M.S.E. at Doernbecher Children's Hospital received approximately $7,000 from the Jackson Foundation for initial purchasing of telemedicine equipment, prior to this study's conception. Doernbecher Children's Hospital also receives ongoing support from the Friends of Doernbecher for continuing telemedicine program logistical support (approximately $7,500/year). P.B., J.B., H.R.F., and J.P.M. declare no competing financial interests exist. None of the foundations that funded the telemedicine program or research efforts was involved with conceptualization, design, data acquisition, data analysis, or interpretation of results for this study.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.