
Abstract
Introduction
There has been an expansion of the communication infrastructure in many countries. Broadband networks are evolving from research functions to enabling service delivery, including healthcare. Mobile-based broadband connectivity is especially creating new opportunities. The role of advanced network technologies and their relation with healthcare innovation have been widely discussed. 1 –10 There has been an increasing interest in understanding how infrastructure changes will impact on future telehealth applications.
Although most developed countries have, or will soon have, communications infrastructure capable of supplying fixed or mobile connections to broadband connectivity to nearly all of the population, infrastructure costs might limit the level of connectivity for those living furthest from major centers. 11 Other community members might be isolated by economic or lifestyle factors. However, members of this group are seen as the major beneficiaries of telehealth, so telehealth can deliver on its potential only if the communications infrastructure meets certain acceptable criteria. The aim of this research was to provide a background for defining those criteria.
Telehealth brings together a variety of infrastructures, including network communication technologies, computer systems, and diagnostic peripheral devices. We have interpreted infrastructure to include the physical network and its associated standards, protocols, and services. The scope of the study was therefore broadened to a more general view of telehealth trends, with a strong emphasis on infrastructure implications. Although driven by some of the questions raised by the Australian National Broadband Network, 12 the study has attempted to be international in its outlook, respecting the view that telehealth is an open and constantly evolving and adapting science. 13
Materials and Methods
Most of the literature on technology prediction consists of reports of roundtable or think tank discussions. 9,14,15 However, studies have shown that cutting-edge telehealth technologies and pilot applications developed a decade ago are becoming common today, 1 some technologies that will be adopted by telehealth over the next couple of decades could have already been developed in other contexts, 6 and experimental clinical implementations with advanced technologies and infrastructure can provide helpful empirical evidence. 1,8,16 Based on these understandings, we adopted a mixed method for assessing future trends. Details of these approaches are outlined below.
Literature Review
Literature in telehealth was reviewed. We first searched MEDLINE and CINAHL by using the strategy of (“telemedicine” OR “telehealth”) AND (“broadband” OR “broadband network” OR “advanced network”). We limited the search to English language articles published in the last 10 years (the search was conducted in April 2012). This search resulted in 161 articles from MEDLINE and 441 articles from CINAHL. After an initial analysis of these results, a more focused search was conducted in the Journal of Telemedicine and e-Health and the Journal of Telemedicine and Telecare by using the search functions on the publishers' Web sites. We used the terms “broadband,” “next generation,” “future,” and “future infrastructure.” We also refined our search strategy to only include articles from 2007 to 2012. Consequently 449 articles from the Journal of Telemedicine and e-Health and 306 from the Journal of Telemedicine and Telecare were found. Full texts of 34 articles from 2007 to April 2012 were extracted for review from a filtering process using at least one of the following criteria: • At least one bandwidth-critical current application is described. • An application in the frontier of current practice is described. • A technology associated with advanced networks is discussed in the context of telehealth. • There is a substantial discussion of future trends.
Inferences from our Demonstrator Projects
As part of the Centre for Networking Technologies for the Information Economy, several advanced telehealth systems were examined over broadband networks. 17 –20 All were the subject of evaluation in a clinical setting and provided insight into how improved network infrastructure can enhance telehealth applications. All used multiple channels of near-broadcast-quality video and were used in point-of-care situations (apart from the training application). Each application was custom-designed around the application's clinical needs, rather than being based on commercially available devices. They are summarized in Table 1.
Summary of Demonstrator Projects
In these projects, we incorporated design and evaluation approaches from the field of computer-supported cooperative work (CSCW). 17,20 CSCW is a design-oriented academic field that looks at how people collaborate and the impacts of technology on collaborations and work practices. Some of the recent research in CSCW involves collaboration technologies in advance of what are used for telehealth. We briefly reviewed these recent works by searching related journals and conferences in the CSCW field.
Interviews with an Expert Panel
Members for an expert panel consisting 11 international thought leaders in telehealth from Australia and the United States were identified and interviewed over a period of 5 months. Members were chosen based on their perceived eminence in the field, association with advanced applications, and availability for face-to-face meetings followed by an in-depth interview during the period of the study. Members' details are listed in Table 2.
Details of Expert Panel of Thought Leaders
Each semistructured interview lasted around 45 min and was conducted either in person or using Web-based videoconferencing. Participants were asked questions in these categories: their telehealth experience; experience with advanced systems; future developments; success factors and barriers; and new applications. Interviews were audio-recorded, and transcriptions were analyzed using thematic coding. 21 The initial data coding was based on the interview structure, and after several iterations in analysis, major closely related themes were identified.
The interview protocols were drawn up following preliminary analysis of the telehealth literature and demonstrator projects. During the analysis, where appropriate, references from the literature were used to augment, amplify, and verify the interview findings. Related work in CSCW also informed some of the final analysis and in particular prediction of some future trends. Of the methods used in this study, interviews had the greatest impact on our findings, while results from other methods have provided a foundation to understand and analyze interview data. This analysis protocol is shown in Figure 1.
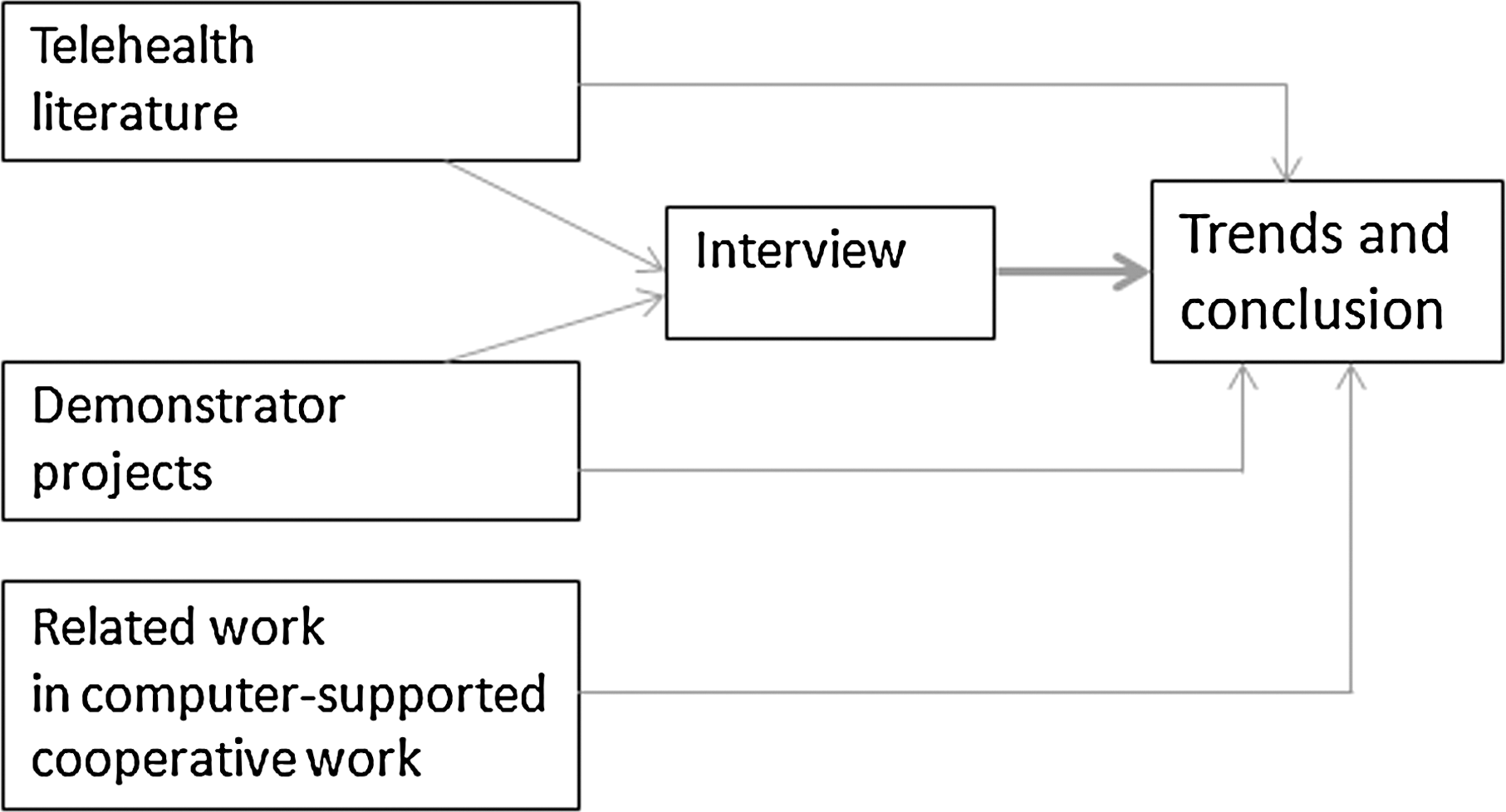
Analysis protocol.
Results
We identified the following three broad themes for classifying developments in telehealth, namely
• Care models
• Clinical applications
• Technology developments
Several subthemes emerged, as shown in Figure 2. This is similar to the three-dimensional telemedicine taxonomy (functionality, technology, and applications) defined by Bashshur et al., 22 but we have interpreted care models and technology in a broader sense.
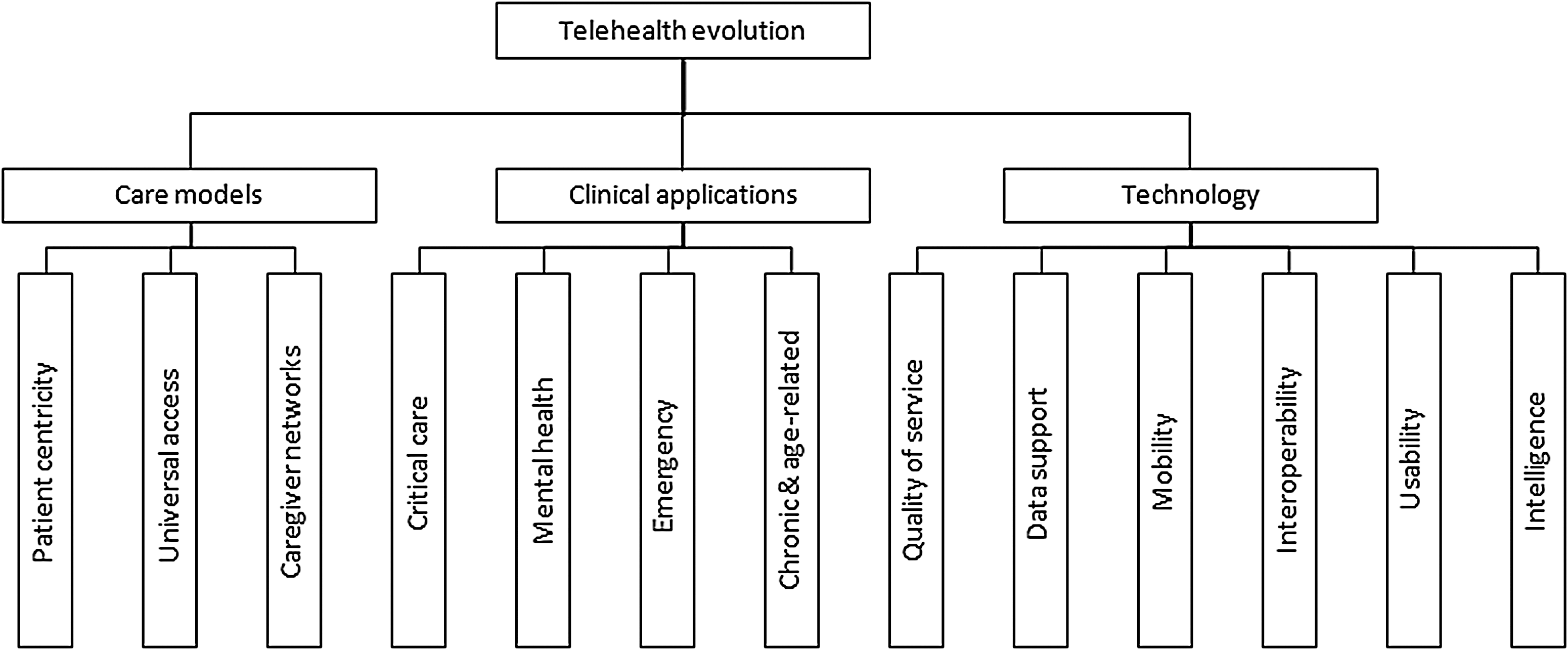
Themes emerging from the study.
Care Models
Advanced network infrastructure is enabling a range of fundamental redesigns of health care processes. 4 We will describe three emerging trends in care models that were particularly mentioned by interview participants.
Patient-centricity
Underlying many of the responses from interview participants is the concept that healthcare should become more patient-focused. Patient-centricity is a worldwide trend in healthcare toward healthcare models able to adapt more to the needs of the patient, who is able to exert more direct control of the nature and location of health service delivery. 4,5 Patient-centric healthcare models are facilitated by e-health and particularly by telehealth technologies through the ability to replace traditional healthcare enterprises with virtual enterprises centered on the patient. 4,23 Technologies supporting such models include patient-accessible electronic health records, 5,24 as well as home-based and mobile portals to health information and expertise. 25 –27 Participants indicated that this new model empowers patients to take a more active role in their healthcare and that this is “turning the health system upside down.” They explained that patient-centricity implies that most interaction between patients and health systems will take place outside health facilities and that the single most significant aspect of patient-centricity will be the rise of home-based and mobile applications. Wide ranges of remote home monitoring applications are increasingly based on high-speed Internet connectivity models: wired broadband, third-generation wireless, or a combination. 28
An important enabling technology will be patient health records accessible by both patients and carers. 5,20 Some of the participants mentioned that there have been national initiatives in the United States and other countries (e.g., the patient-centered medical home in the United States 23 and the personally controlled electronic health record in Australia 29 ). Some of them also pointed out that in the future, patients will be able to share their data with several clinicians who give their opinions asynchronously, and there will be impromptu and flexible access to specialists.
Universal access to quality healthcare
National telecommunication infrastructures or initiatives in some countries and areas have provided universal access to support the development of innovative telehealth (e.g., in northern European countries, 30 the United States, 31 and Australia 12 ). One of the participants described the universal access enabled by advanced network this way: “You got universal access and what that does is empower patients and making the health facilities less important. It suddenly gives you a distributed architecture for healthcare, rather than architecture that is based on provider funded.” Another participant drew on the fact that many other service industries (e.g., entertainment, banking, retail stores) have already brought their services to their customers' homes and argued that medical service can do the same.
Caregiver networks
Current healthcare models are based on a one-to-one relationship between a clinician and a patient. Changes in care models catalyzed by universal access and patient-centricity will change this model in several ways. Participants pointed out that there will be collaborative caregiver networks and that each caregiver can be considered as part of a team. General practitioners or others caregivers can have more informal conversation and interaction with specialists. It will provide peer-to-peer support and education services for health professionals and family carers. Asynchronous (store-and-forward) information sharing can play a role in this to support access to symptom data. 8,32 Future clinical interactions will occur “anytime, anywhere.” 8 This will be enabled by new communication patterns based on advanced telecommunication infrastructure and mobile communication. 27
Clinical Applications
Critical care has been an area of recent rapid advancement. Emergency medicine was considered as an emerging application in 2002, 33 and telepresence and telemedicine in trauma and emergency were identified as new frontiers applications in 2008. 34 Intensive care applications have been increasing since the first commercial system (e-ICU) was installed. 35 Telestroke is an emerging, highly effective application in the telehealth field. 36 Ambulance services and natural disaster telehealth empowered by wireless mobile technologies have emerged recently. 37,38 Our demonstrator projects also showed the efficacy of advanced, multichannel telehealth systems in critical care. 17,19 In some of its more challenging clinical applications, telehealth is moving away from a videoconferencing model toward the actual delivery of health services via technology, with telehealth equipment designed to be used in such point-of-care locations as intensive care unit wards, emergency departments, and operating rooms. 18,34,36
We asked participants to name a couple of potential clinical applications that can make impact in the future. Mental health and chronic disease management have been mentioned by most of the participants and particularly linked to areas of personal healthcare (e.g., homecare and mobile applications). Participants reported from their firsthand experience that chronic disease management is “incredibly powerful and valuable” and that patients are being empowered for managing their own chronic disease at home.
Technology Developments
We defined technology developments to broadly include quality of service (bandwidth, latency, etc.), integration with medical record data, mobility (availability on mobile devices for patient and caregiver), interoperability, usability, incorporation of intelligent systems, and adaptability for multiple uses.
Quality of service
All the participants agreed that from an infrastructure perspective, “the more bandwidth the better.” Participants pointed out that it is widely accepted that higher bandwidth allows low latency, smoother interaction, and clearer visualization of images. Higher bandwidth allows a better design of the telehealth systems. Some of the participants argued that until users actually experience a telehealth system, it is hard to hypothesize that they do not need any more bandwidth.
Bandwidth-critical applications. Participants mentioned some applications that will benefit from higher bandwidth and higher resolution, including those requiring direct interactions with patients for diagnosis, physical assessment, real-time diagnostics video, streaming video, or emergency and surgery applications. Examples from the literature include critical and emergency care, 17,19 real-time tele-ultrasound consultations, 39 –41 remote-controlled real-time echocardiographic examination, 42 real-time telesurgery education, 17,43,44 telesurgery mentoring, 39,45 and telesurgery and robotic surgery. 46 Network transmission latency was mentioned by participants as a critical factor for telepsychiatry and robotic telesurgery. For example, network jitter could cause confusions to telepsychiatry because “they do not know whether it is the network problems or the patient has that disease.”
Participants indicated that requirements of bandwidth vary in different clinical applications that have different complexities and situations. As one of the participants stated, “You do need to provide the kind of infrastructure that will be able to embrace all of the medical specialties that you might think someday will be used.”
Telepresence and interacting with data. A sense of presence can be supported by advanced networks, especially in telemedicine where real-time video allows “being-there” interactions. 1 This has been mentioned by participants as important in teleconsultation because it helps develop trust between the clinician and the patient. Applications involving imaging and visualization, collaboration, and sharing also require advanced networks and computing facilities. 1 Video telepresence can be extended by other technologies, such as three-dimensional visualization, three-dimensional immersive environments, and haptic devices. 1,17 Telehealth applications using digital interactive television 47 and multidisplay environment and multitouch mobile devices with a range of interaction techniques have been explored recently by CSCW researchers. 48
Design for enhanced collaborative practice. Participants indicated that higher bandwidth allows more task-oriented design of telehealth systems. This includes supporting multiple channels and shared interaction with data. Our broadband telehealth pilots (Table 1) have demonstrated that multiple, high-quality video channels enhanced the ability to perform complex tasks and clinical practices such as critical care. 17,18 We also found that high-quality communications between teams can positively affect the relationships among teams working across multiple sites. 18,20 Better design can improve perception of the situation in the remote environment. 34,45 Recent CSCW systems have provided rich support for the concurrent display of several different information streams, including live video streams of participants and shared interaction with a range of data in distributed collaborations. 49 This not only reproduces face-to-face telepresence but also improves the user experience of shared interaction with data and coordinating activities among the distributed individuals and teams. 50,51
Symmetry and asymmetry. There was lack of unanimity in our panel on whether the bandwidth needed to be symmetrical (the same in both directions). One participant argued that clinicians can be just a “talking head” to give the patients comfort but that clinicians need higher quality of a patient's image because that image is used as a diagnostic tool. A similar argument is found in the literature that clinicians want telemedicine consultations to give them ample and reliable data and that patients may be concerned whether they can be examined sufficiently by the clinicians. 9 However, another participant felt that it needs to be symmetrical in order to maintain a good interaction between the two. Most CSCW systems are designed to support symmetrical interaction with people and information. Asymmetrical design in telehealth might be essential when network upstream bandwidth is limited (e.g., in satellite, mobile, and wireless communication). 11
Data support
A particular technical challenge for some telehealth applications is the simultaneous availability and appropriate integration of different contents/components, including live video, electronic health record, documenting the encounter, and remote monitoring. 6,52 The challenge also includes seamlessly moving large datasets in real time among hospitals, other medical facilities, and homes.
Multiple functionalities and ubiquitous data. Participants discussed the particular feature of ubiquitous data from multiple sources in telehomecare systems. Data can come from sophisticated reminder systems, tracking systems, and physiological monitoring systems. 53 One participant predicted that future telehomecare will be part of the integrated services that have multiple functionalities (including non–health-related) and that bandwidth can be an issue if involving multiple home users doing multiple Internet tasks at the same time.
Supporting advance multimedia data. Participants pointed out that advanced high-resolution multimedia data will be increasingly used in telehealth. Examples include uncompressed high-definition video (e.g., teledermatology) to detect color change and tissue dynamics, high-definition computed tomography scans and magnetic resonance imaging images, and three-dimensional immersive and haptic technologies in training applications. Our demonstrator projects have explored some of these technologies. 17 Trials of high-definition three-dimensional technologies have been reported in areas of telewound, tele-oncology, and telepsychiatry and that some of these applications (wound management, teledermatology) can be used in the home environment. 54
Integrating with medical record systems. This has been considered as desirable but often very difficult to implement because of the issue of different medical record systems and communication between them, according to all of the participants. A trend highlighted by one participant is the capability to capture telehealth-session video and store it into the electronic record system for asynchronous late access, and there have been studies showed the efficiency of this disruptive way of practice. 8
Mobility
As mentioned by our participants, tablet devices are being increasingly used by clinicians, for example, when they are on call and need to access medical images or remotely observe a patient to make a decision. Mobility is also regarded by participants as important in home applications. The use of mobile communication and devices has been reported in remote monitoring, 28 chronic disease management, 25 and emergency natural disaster. 37,38 Fourth-generation (e.g., WiMAX) mobile networks and technology can provide up to 100–200 megabits/s speed and have been used to support teleconsultation for rural areas and countries with little wired infrastructure. 2 But, interestingly, participants ranked mobility as less important than other issues because it is only “important for those parts of the care model that require mobility,” as commented by one participant. They explained that some applications require a more reliable or fixed data platform, particularly when communicating complex medical information.
Interoperability
Interoperability can be interpreted at one level across different devices and at another level across organizational boundaries according to our participants. Device-level interoperability is especially important for peer-to-peer systems in homecare. Development of technical standards ensures that interoperability among equipment and software products, including personal health record, is transparent to the end user. 29 At a higher level, organizational and human aspects were considered by the participants as an issue of interoperability. Other findings from interviews include the call for interoperability at an international level due to the increasing international collaborations in disease campaigns and global public health and the issue of internationally mobile population.
Usability
End-user adoption of next-generation telehealth technologies is challenged by the need for the integration of new technologies in clinical practice workflow and daily activities. 9 Usability has been described as a “fundamental” and “extremely” important technology need according to the majority of the participants. Some ranked it as one of the most important needs. This is echoed by our broadband telehealth experience, which shows the importance of design for application and task focus, especially in complex applications. 17 –19 CSCW researchers also particularly emphasize the need of understanding “the communication and cooperation mechanisms” when designing technology to support collaboration in healthcare. 55
Intelligence
System intelligence has been considered as “one of the key things missing” in current telehealth applications by some participants. Learning and intelligence will be important features of future telehealth systems. Existing and future technologies, including sensor, smart house, and robot supervision, will allow devices to interact using intuitive interfaces. 56 By using an example of remote monitoring, one participant explained that a reliable intelligent risk assessment is required to overcome the large numbers of patients and large data overload, efficiently assess the patient's status, and make accurate decisions. Another participant predicted that “intelligent use of information, sophisticated use of information and decision making based around solid evidence and solid rules will be the future, but it will take a while to get there.”
Adaptability
Our interview results showed that adaptability will be imposed on future telehealth systems in two ways. First, as telehealth becomes more embedded in healthcare, systems will need to be multipurpose in order to avoid requiring a series of peripheral devices at any location in the health system. This will obviously produce design challenges as telehealth is used for more specialized clinical purposes. Conversely, users of healthcare systems will access information via a range of peripheral devices, ranging from tablets to multiscreen high-definition interfaces, with information tailored to match the peripheral device as well as their workflow.
Discussion
From this study, it is likely that there will be simultaneous (and indeed coupled) evolution of telehealth through the space spanned by care models, clinical applications, and technology (Fig. 3 , left). These three dimensions are interrelated: elements in one axis can drive elements in other axis, and technical developments in healthcare will be coupled with developments in models of care and needs of clinical applications. It is possible that the relatively slow uptake of telehealth results from the mutual interdependency of these three axes.
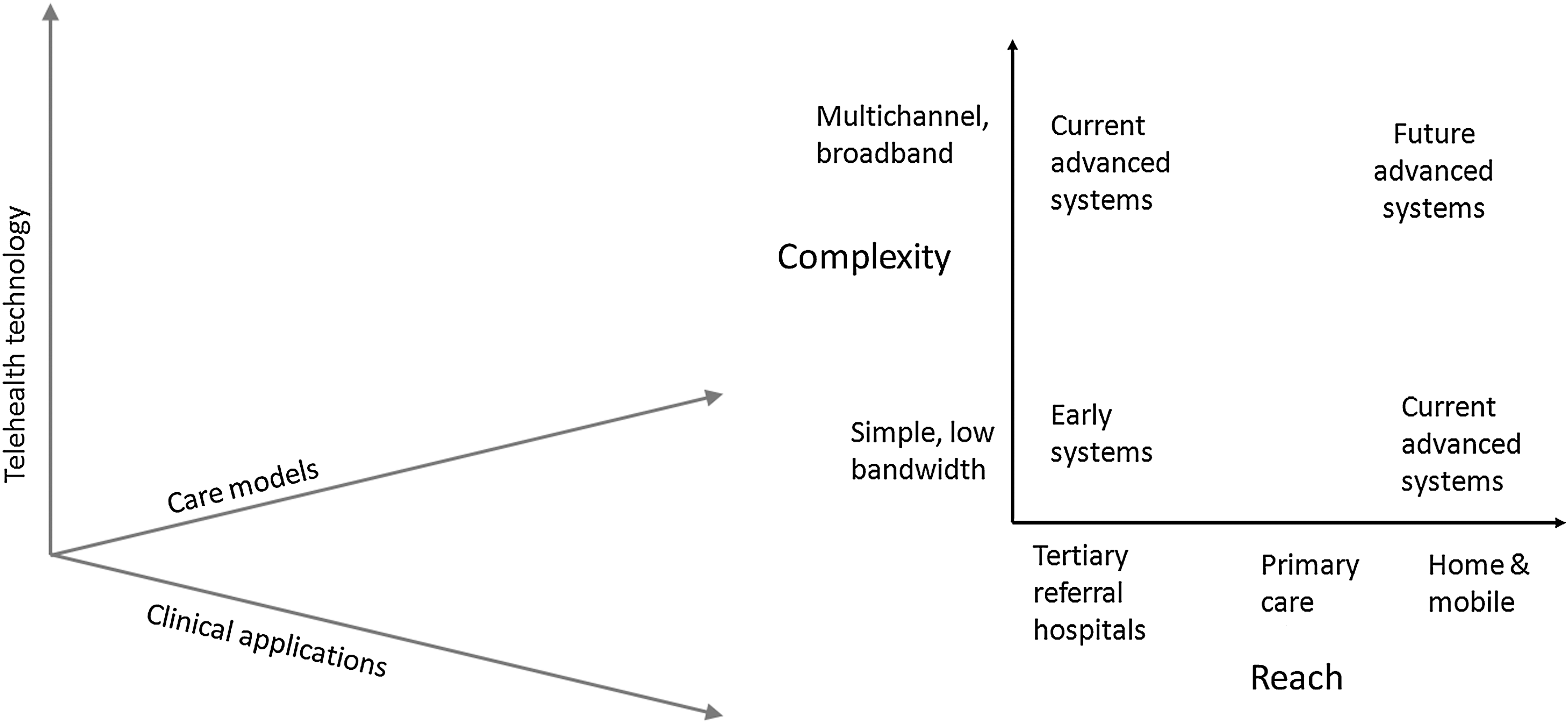
For describing future telehealth trends, we consider a two-dimensional subspace of our three-dimensional model defining the reach and the complexity of the application (Fig. 3, right). We define reach in terms of the parts of the health system linked together (ranging from tertiary referral hospitals at one extreme to an individual patient at the other) and complexity as the amount and structural complexity of the information transferred in the interaction: • The Care model and Clinical application axes in our three-dimensional model can be considered as collapsing onto the single dimension we have labeled Reach. One of the aims of telehealth is to move healthcare to the right of the plot in Figure 3, right, resulting in a decentralization of health services. • Another dimension is the Complexity trend—what an application could potentially do when more bandwidth is available. Multiple-channel videoconferencing for critical care and emergency care have been examples of current advanced systems along the complexity axis. • Advanced network infrastructure will make possible applications toward the top right of this graph. For example, multichannel broadband telehealth into homes will be the convergence of diagnostic, communication technologies, and health record systems; telehealth systems will need to seamlessly move large datasets in real time among hospitals, other medical facilities, and homes—a recently demonstrated example of this trend was a wound management project that makes use of high-definition three-dimensional video.
54
Some of the infrastructure-specific findings are: • It is not advisable to suggest an upper limit on bandwidth or other measures of quality of service for telehealth infrastructure. But if there are severe constraints, support of two channels of high-quality video information should be seen as a minimum. • As the health system becomes more decentralized and applications become more diverse, these requirements will need to be extended to smaller healthcare centers and even the home. • Infrastructure standards need to incorporate mobility, interoperability, usability, intelligence, and adaptability features, which need to be supported in future telehealth systems.
Telehealth services for the most remote users should not be compromised by inadequate infrastructure. Compromising the infrastructure by limitations on quality of service (especially bandwidth, latency, and symmetry) will deny high-quality healthcare to those who stand to receive the greatest benefit from telehealth.
We also suggest that future telehealth research can integrate the work done outside telehealth (especially CSCW) as clinical applications become more complex. Some of the benefits of broadband telehealth (as opposed to some current implications) are in the “social” domain, such as relationship, trust, and interaction experience, rather than clinical diagnosis. 57 There are implications in the consequences of providing differing levels of quality in the infrastructure. Future work can also include understanding the benefits of telehealth. Advanced systems usually involve higher costs, but the benefits of this expenditure (which might not be immediately realized) are rarely quantified.
The study has some limitations. We acknowledge a degree of subjectivity of the analysis, due to the qualitative nature of much of this research. Also, for logistical reasons, the interview participants were restricted to experts from Australia and the United States, so the findings may be biased toward solutions applicable in these two countries. Some countries are evolving their health systems much more rapidly because of lack of legacy systems, and studies of regions such as China or India might reveal some different findings.
Conclusions
In conclusion, over the next two decades, telehealth will evolve along three interdependent “axes”: care models, clinical applications, and technology, with perhaps care model evolution bringing the greatest changes. A current barrier is (in most countries) the lack of a suitable network infrastructure. However, provision of such infrastructure will not alone bring about change. It is important that it is very difficult to extrapolate from current telehealth delivery models as most of these lack the scale that makes system-wide change possible. Universal access to good communications will itself drive change.
Footnotes
Acknowledgements
We would like to thank the expert panel of thought leaders: Michael Ackerman, Dale Alverson, Colin Carati, Branko Celler, Patrick Cregan, Yogesan Kanagasingam, Mohamed Khadra, George Margelis, Jay Sanders, Yulun Wang, and Peter Yellowlees. We also thank Gary Doherty from the CSIRO ICT Centre for his support of this study and Dr. Iain Collings from the CSIRO ICT Centre for a useful discussion on technology developments. The demonstrator projects were supported by the Australian Government through the Advanced Networks Program of the Australian Department of Broadband, Communications and the Digital Economy.
Disclosure Statement
No competing financial interests exist.