
Abstract
Introduction
Chronic disease is a leading cause of morbidity and mortality worldwide. The developing world carries this burden disproportionately, with 80% of deaths attributable to cardiovascular disease and diabetes mellitus and 90% of deaths attributable to chronic obstructive pulmonary disease occurring in low- and middle-income countries (LMIC). 1 By 2030, it has been estimated that 23 million people will die annually from cardiovascular disease, with approximately 85% happening in LMIC. 2 In addition, chronic conditions have become a marker of the increasing health inequalities in LMIC, highlighting the urgent need to implement more effective and cost-effective interventions. 2
Morbidity and mortality due to chronic disease are largely preventable through counseling, risk factor modification, and medication adherence, but implementation of these interventions is difficult in resource-limited settings. 3 These interventions need to be integrated into primary healthcare systems and tailored for LMIC for them to be affordable, effective, and accessible, especially for disadvantaged groups. In this sense, e-health interventions have the potential to support these aims in an economically viable and sustainable way. 4
Mobile health (m-health) refers to the use of mobile telecommunication and multimedia technologies for healthcare delivery. 5,6 M-health has been shown to improve patient–provider communication and assist in disease management, although most studies have focused on communicable diseases and/or developed countries. 7 –9
In 2002, the number of wireless mobile phone owners surpassed the number of landline telephone owners worldwide, and by 2020 analysts predict 50 billion users worldwide. 10 –13 Moreover, it has been predicted that by 2017 there will be “more mobile phones than people” on the planet, 14 and currently three-quarters of the world's population have access to a mobile phone. 15 The World Health Organization (WHO) has announced that m-health has the potential to transform the face of health service delivery across the globe. 16 Within continents, there is country-to-country variability, but penetration in some developing countries exceeds 100%. 17 With the basic infrastructure in place, the integration of mobile technology into the healthcare system may be a feasible way to complement and improve current chronic disease management strategies in LMIC. 3,18
Data from developing countries have highlighted the impact of mobile technology on communicable diseases, such as tuberculosis, human immunodeficiency virus, and malaria. 19 –22 However, to date most of the data on the use of mobile technology in chronic disease and risk factor management are from developed countries. This review aims to study the impact of mobile technology (voice communication and short message service [SMS]) on chronic disease outcomes in LMIC.
Materials and Methods
Systematic literature searches were performed from December 2011 to June 2012 using the following electronic bibliographic databases: Cochrane Central Register of Controlled Trials (CENTRAL), MEDLINE, EMBASE, and the Latin American and Caribbean Health Science Literature Database (LILACS), according to MOOSE and PRISMA guidelines. 23 –25 A search strategy for gray literature was included to retrieve information from relevant sources, like the WHO and the Inter-American Development Bank, reference lists of included studies, and consulting experts related to the topic. In addition, generic and academic Internet searches and meta-searches were performed. Authors were contacted to obtain missing or additional information when needed.
Key words used in these searches included the following: telecommunication, cellular phone, cell phone, mobile phone, short text message, multimedia message, lifestyle, reminder system, risk reduction, patient education, self-management, patient compliance, primary prevention, outcome assessment, developing countries, underserved areas, and the specific LMIC.
Details of the search can be found in Supplementary Tables S1–S4 (Supplementary Data are available online at
Studies were included if they (1) were randomized controlled trials (RCTs) or systematic reviews and meta-analyses of RCTs with original data, conducted in a LMIC as defined by the World Bank published or reported between 1990 and June 2012, 26 (2) included subjects over 18 years of age, (3) addressed the impact of mobile technology, using short messaging system or cellular telephone interventions on a chronic disease (asthma, diabetes, hypertension, tobacco use, cardiovascular disease, chronic respiratory disease, and cancer), and (4) measured outcomes including morbidity, mortality, hospitalization rates, behavioral or lifestyle changes, process of care improvements, clinical outcomes, costs, patient and provider satisfaction, compliance, and health-related quality of life (HRQoL). No language requirement was imposed. Data were limited to studies from the aforementioned databases.
Randomly assigned pairs of reviewers independently evaluated selected abstracts. Articles whose abstracts met the inclusion criteria were reviewed by a separate, randomly assigned pair of reviewers. If the article met the inclusion criteria, these reviewers extracted pertinent data and assessed methodological quality using the Cochrane Risk of Bias Assessment Tool. 27 Discrepancies in article inclusion, data extraction, and bias assessment were solved by team consensus. Early Reviewer Organizer Software (EROS) version 2.0 was used by reviewers' for full text evaluations of articles, data abstraction, and quality assessment. 28 –30 Risk of bias graphs and meta-analysis were performed using Review Manager (RevMan) software (version 5.1). 31
Results
We retrieved 1,709 abstracts using the search terms, and 163 articles were selected for full text review. Of these, 154 were excluded because they were conducted in upper-income countries (n=54), did not address m-health (n=56), were not RCTs, systematic reviews, or meta-analyses (n=33), or did not focus on chronic disease (n=11).
Nine studies with 4,604 participants were included in the systematic review (Fig. 1). Included studies came from seven countries: China (n=1), Taiwan (n=1), Malaysia (n=2), Poland (n=1), India (n=2), Croatia (n=1), and Uruguay (n=1). All the studies evaluated more than one outcome. Six studies addressed clinical outcomes, six addressed processes of care, three addressed costs, two examined patient–provider compliance, and two examined HRQoL (Table 1). Risk of bias assessment found that the lack of blinding may have biased the results of three studies, and unclear allocation concealment may have affected seven studies. However, the majority of the risk of bias criteria was classified as low or unclear (Fig. 2).
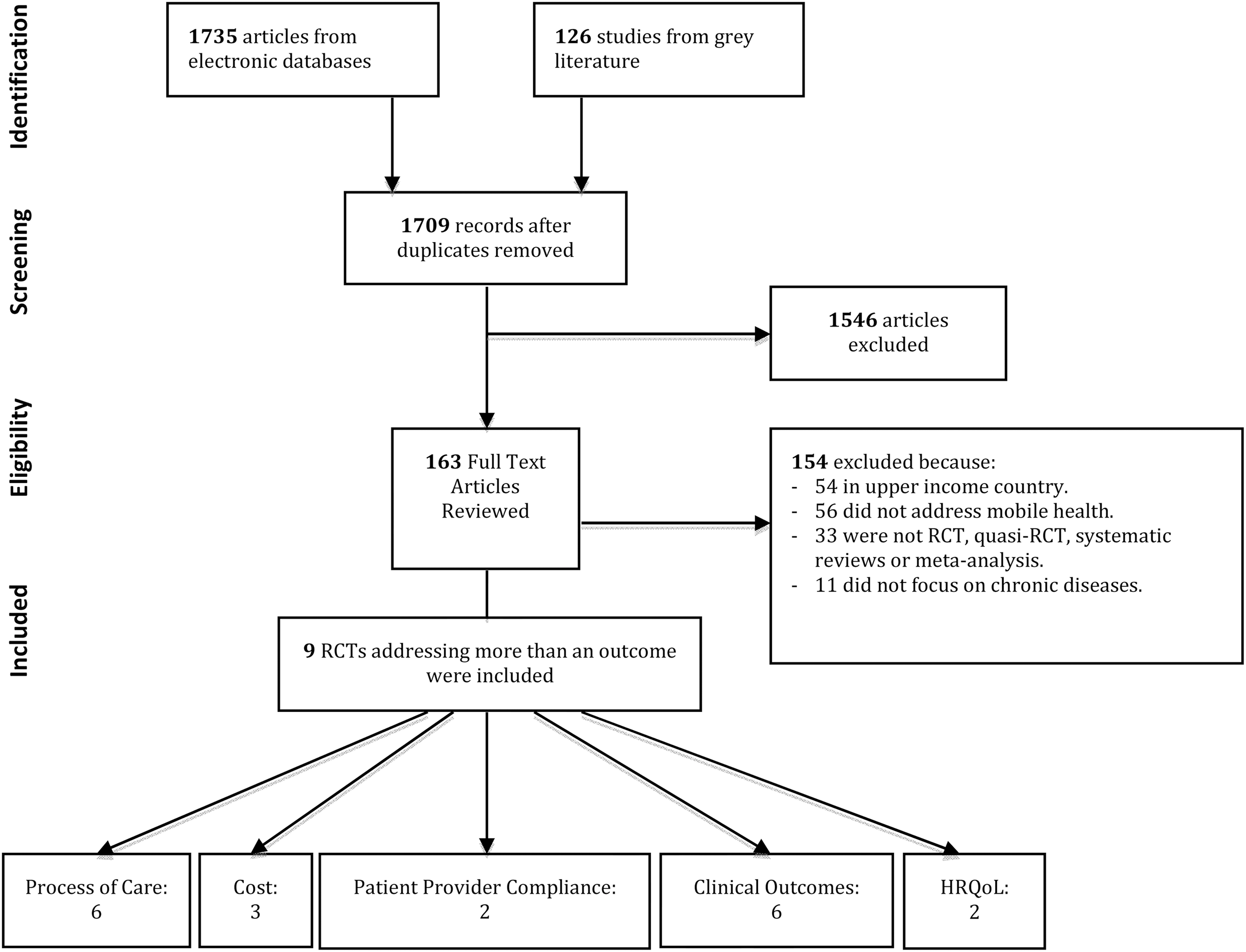
Flow of information through the systematic review. HRQoL, health-related quality of life; RCT, randomized controlled trial.

Risk of bias of included studies: low (light gray), high (dark gray), or unclear (white).
Details of Included Studies
6MWT, 6-min walk test; ARI, acute respiratory infection; BMI, body mass index; FEV1, forced expiratory volume in 1 s; FVC, forced vital capacity; HbA1c, hemoglobin A1c; HDL-C, high-density lipoprotein cholesterol; HRQoL, health-related quality of life; J-Index, a glucose variability index; LDL-C, low-density lipoprotein cholesterol; MBG, mean blood glucose; MCS, mental component score; NNT, number needed to treat; NS, not significant; NYHA, New York Heart Association; OR, odds ratio; PCS, physical component score; PEF, peak expiratory flow; pred, predicted; SMS, short messaging system; TC, total cholesterol; TG, triglycerides.
Clinical Outcomes
Clinical outcomes are intermediate outcomes or markers of disease severity, such as hemoglobin A1c in diabetes or peak expiratory flow rates in asthma and visits to the emergency room or hospitalization. Clinic outcomes were studied in six articles.
Ostojic et al. 32 studied the impact of SMS on asthma; subjects transmitted home spirometry readings to physicians via SMS and then received telephone counseling. Intervention subjects had six more office visits, two more acute respiratory illnesses, and five fewer hospitalizations than the control group. After 4 months, the study group's forced expiratory volume in 1 s was significantly improved compared with no change in the control group's forced expiratory volume in 1 s. Control subjects had significantly higher rates of cough and night symptoms compared with the SMS group. Liu et al. 33 evaluated the effect of a mobile telephone-based interactive self-care software plus management feedback on pulmonary function, visits to the emergency department, hospitalization, medications used for asthma control, and HRQoL. Patients in the intervention group had improved pulmonary function and HRQoL and decreased unscheduled visits to the emergency department and hospitalizations. Regarding medication use, mean daily dose of systemic or inhaled corticosteroids and the proportion of participants who received leukotriene inhibitors increased significantly in the intervention group.
Ramachandran et al. 34 studied the impact of mobile technology counseling on the New York Heart Association functional class, 6-min walk test distance, physical impairment, and symptoms in congestive heart failure subjects in India. At the end of the study period, significantly more study subjects were categorized as New York Heart Association Class I and II, had a higher mean 6-min walk test distance, and showed greater improvements in 6-min walk test distance from baseline, compared with controls. Study subjects had significantly fewer symptom complaints compared both with initially reported symptoms and with the control group. Finally, the intervention group had a significant improvement in physical impairment scores, whereas the control group had no change.
In two of three studies diabetic clinical outcomes improved with m-health interventions. Wojcicki et al. 35 found that patients who transferred daily glucose readings to physicians using a telematic system and received telephone medication regimen feedback had better diabetic glycemic control, as defined by mean blood glucose and glucose variability indices, than control subjects. Although there was no significant difference in number of hyperglycemic or hypoglycemic episodes in the control or intervention group, the absolute number of either event was lower in the intervention group. Shetty et al. 36 evaluated the use of SMS to ensure adherence to management prescriptions and clinical outcomes in type 2 diabetes compared with standard care. This study showed that patients who received SMS had better glycemic control.
Balsa and Gandelman 37 looked at the impact of a Web-based education program with SMS reminders and updates, comparing it with that of a brochure-educated control group, and found that the intervention had no impact on glucose control.
Process of Care
Process of care outcomes are defined as those that affect patient care by improving healthcare delivery or patient–healthcare interactions. Of the studies included in this systematic review, three processes of care outcomes were identified: clinic attendance, chronic disease monitoring system effectiveness, and compliance with a Web-based and a mobile application.
Four studies included in this review evaluated the impact of text messaging on attendance rates to clinic appointments. Three studies demonstrated improvements in clinic attendance with text messaging reminders versus no reminder. In three studies, 38 –40 subjects were randomized to receive an appointment reminder by text message, an appointment reminder by mobile telephone call, or no reminder. Shetty et al. 36 compared the effect of one SMS reminder sent to type 2 diabetes patients every third day for 1 year regarding lifestyle modification, medication adherence, and clinic attendance. No differences were observed in this study toward improvement in frequency of visits and annual check-ups between groups.
Balsa and Gandelman 37 studied the effectiveness of an Internet-based diabetes education program with SMS and e-mail reminders and found that only 77 (39%) of the treatment arm logged-on to the online education program, and of these subjects, 34 (44%) logged-on once, 12 (16%) logged-on twice, and 31 (40%) logged-on more than three times. When subjects were asked about the number of times they logged-on, 22 (14%) stated that they had used the Web site when in fact a log-in was not recorded. Of the subjects who reported never using the Web site, 8% stated they were not interested, 12% reported using other sources of information, 54% claimed they were not frequent Internet users, and 14% believed they already possessed all the diabetes information they required. Sixty-five percent of the participants received periodic SMS reminders about the project. Liu et al. 33 evaluate compliance with the interactive self-care system compared with a written asthma diary booklet to improve asthma control. At 3 and 6 months, respectively, 81.7% and 71.7% patients were still adherent to the interactive self-care system and sent data to the Web site versus 85% and 76.7% in the control group, but differences were not statistically significant.
Costs
Several studies have examined the effects of m-health technology on healthcare costs, and all have found that m-health is cost-effective. Chen et al. 38 and Leong et al., 39 whose studies showed that SMS and telephone reminders improve appointment attendance rates, evaluated cost-effectiveness as a secondary outcome. SMS was found to be 35% and 45% less expensive, respectively, per attendance than telephone reminders. Both noted savings accrued through reductions in the number of work hours required by research assistants and in telecommunications costs in the SMS group. Ostojic et al., 32 whose study showed m-health improves asthma control, found that SMS costs each patient 0.67 Euro and each physician 1 Euro per week.
Patient–Provider Compliance
Ostojic et al. 32 examined the physician or patient compliance rates and found no significant difference between the SMS group and the control group when evaluating patients' compliance with three times per day peak expiratory flow measurement. Patients in the SMS group submitted 99% of their daily messages to their physicians. Shetty el al. 36 found that there were no differences in the annual check-up visit and adherence to diet, physical activity, and drug prescriptions in type 2 diabetes patients.
HRQOL
Two studies evaluated HRQoL. The first included congestive heart failure patients in India who underwent an m-health intervention to adjust congestive heart failure medication, and then HRQoL was evaluated using the Kansas City Cardiomyopathy Questionnaire. 34 The study demonstrated a significant increase in HRQoL in the intervention group and no changes in the control group. Liu et al. 33 found that patients using a mobile telephone–based interactive self-care software for asthma control improved their quality of life. They improved at 3 and 6 months in the SF-12 physical component score compared with controls. There was no significant change of the mental component in the mobile telephone group throughout the study period. However, in the control group it decreased significantly at 4 and 6 months from baseline.
Discussion
M-health is emerging as a useful and promising tool to address several healthcare system constraints in developing countries, such as a limited healthcare workforce, limited financial resources, high burden of disease, high population growth, and difficulties in extending healthcare to hard-to-reach populations. 3 Studies using cell phone voice communication and text messaging were included in our study, as these are the main mobile phone functions currently used in LMIC because of the availability of low-cost handsets, reasonable pricing, and low broadband penetration for interventions that need Internet. 3
Some of the results of this systematic review need to be highlighted within the context of low-resource settings such as those in LMIC. Six articles regarding process of care focused on m-health's impact on appointment attendance rates, and two examined the effectiveness of a mobile application plus feedback advice for disease management. In all attendance rate studies, SMS and mobile phone appointment reminders significantly improved attendance rates. These results are in accordance with two recent systematic reviews that have described a robust evidence base for the use of text message reminders to improve attendance at healthcare appointments. 9,41 A teletransmission system associated with an application and SMS to improve self-care was found to be an effective tool in asthma management, but no significant impact was seen on diabetes. In fact, de Jongh et al. 42 found limited benefit of mobile phone messaging in supporting the self-management for long-term illnesses.
Three studies looked at cost-effectiveness, of which two were clinical trials on appointment reminders and one involved asthma control via peak expiratory flow reporting. SMS reminders were more cost-effective than telephone interventions and were equally efficacious. M-health improved asthma control, and the additional cost of monitoring was minimal.
Four of five trials studying the effect of m-health on clinic outcomes found that mobile interventions improved outcomes. With regard to diabetes, two studies found improved glycemic control in the study group compared with the control. A study of usual heart failure care compared with weekly mobile telephone disease counseling and access to a telephone helpline showed improved quality of life, functional capacity, symptoms, and physical impairment. Finally, transmission of daily spirometry readings with physician feedback improved asthma control.
These results are in accordance with previous reviews that investigated the impact of m-health on chronic disease in developed countries and showed that this intervention improved behavioral and clinical outcomes, HRQoL, and cost-effectiveness. 7,43 –48
We decided to include in our review only RCTs, systematic reviews, and meta-analyses of RCTs, and not intervention trials using less rigorous methods, such as quasi-experimental studies or reviews containing nonrandomized studies, because RCTs provide stronger and more unbiased estimations of the impact of interventions. This restriction clearly limited the number of articles eligible for this review as our search criteria returned only nine RCTs with 4,604 participants from developing countries. However, despite a recent World Bank report that identified more than 500 m-health pilot studies in LMIC, little evidence was found about the likely uptake, best strategies for engagement, efficacy, or effectiveness. 49,50
Evidence regarding efficacy, effectiveness, safety, cost, and social, institutional, legal, and ethical implications of new technology adoption should guide priority setting, especially among LMIC where resources are scarce and demand for health services is unlimited. 51
Actually, controversy still exists for scaling up m-health interventions as they lack a foundation that would permit evidence-based scale-up. 50,52
Study Limitations
When interpreting the results of this study, some limitations should be taken into consideration.
First, the small number of RCTs using m-health to address chronic diseases in LMIC underscore the need of more rigorous implementation research on m-health in these countries, and second, the small study size of most of the studies included makes it difficult to interpret the applicability of study results to larger LMIC populations.
Moreover, the appropriateness of extrapolating these data to the developing world context is unclear as we were only able to find articles from seven countries, most of them upper-middle-income countries. Furthermore, we found no studies from low-income countries, and since the date studies were conducted, Poland and Croatia were reclassified by the World Bank as developed economies.
Implications for Practice
Developing countries must improve access to and delivery of interventions in order to counter the rising morbidity and mortality of chronic disease. Cellular phones are an established means of communication in developing countries and have been shown to be an effective complement to usual chronic disease management in the developed world.
The integration of mobile interventions into the healthcare system in LMIC may be a feasible way to complement and improve strategies toward prevention and control of chronic diseases, but success in scaling up and sustainability depends on other factors besides mobile phone technology, such as the healthcare context, social values, and culture. In fact, public health and/or healthcare issues vary among LMIC (e.g., the prevalences of diabetes in Poland and India are similar, but Poland has developed national programs for chronic disease management making this intervention easier to implement). 53,54
In conclusion, although only nine articles were found addressing the impact of m-health on chronic disease outcomes in LMIC, m-health was found to be cost-effective and had positive impacts on processes of care, clinical outcomes, and HRQoL. These findings are similar to those found in developed countries and in studies involving communicable disease outcomes in LMIC.
This review suggests that m-health has the potential to use an existing and growing mobile phone network to provide an accessible and cost-effective tool to bridge the equity gap and improve current chronic disease care in developing countries. Further research, preferably large, multicountry, RCTs focusing on a variety of chronic diseases with long-term follow-up, is needed to better understand the impact of mobile technology in LMIC.
Footnotes
Acknowledgments
A.G.L., J.M.W., and E.J. received funding as a Fogarty International Clinical Research Fellow, a program that is supported by the National Institutes of Health, Office of the Director, Fogarty International Center, Office of AIDS Research, National Cancer Center, National Eye Institute, National Heart, Blood, and Lung Institute, National Institute of Dental and Craniofacial Research, National Institute on Drug Abuse, National Institute of Mental Health, National Institute of Allergy and Infectious Diseases, and National Institutes of Health Office of Women's Health and Research through the International Clinical Research Scholars and Fellows Program at Vanderbilt University (R24 TW007988) and the American Relief and Recovery Act.
Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.