
Abstract
Introduction
Mental health clinicians in rural settings often lack the educational support and professional development opportunities available to their urban counterparts. 1,2 To provide evidence-based practice to patients in rural settings, mental health clinicians need specialized training in areas such as dual relationships, overlapping and conflicting roles, and challenges in preserving patient confidentiality that are unique to that environment. 1 –3 These issues can be addressed in training offered to providers. Not only are their training needs varied and different from those of urban practitioners, but limited access to continuing education (CE) opportunities contributes to delays in incorporating the latest treatments, techniques, and research findings into clinical practice. Consequently, CE targeting rural providers can address their unique training needs, foster clinical competence, improve patient outcomes, and lead to greater job satisfaction. 4,5
The Veterans Health Administration provides a broad range of medical benefits to Veterans at Department of Veterans Affairs (VA) medical centers (VAMCs) and community-based outpatient clinics (CBOCs) throughout the United States and its territories. CBOCs were established to provide care nearer to a Veteran's home than a tertiary VAMC. 6,7 Today there are over 800 CBOCs, many in rural areas, operating in conjunction with 157 VAMCs. 8 All CBOCs offer primary care, and many offer mental health services as well. 6,7 CBOCs have a primary care physician, and most CBOCs have at least one mental health provider, often a psychologist, social worker, or nurse. 9
An estimated 1.3 million rural Veterans in the United States suffer from a mental health disorder. 10 Mental illness can be one of the most debilitating of diseases. 11 Rural Veterans experience greater severity of mental health symptoms, 12 have higher rates of suicide, 13 and are less likely to receive psychotherapy than urban Veterans. 10,14 Given the magnitude of the problem, addressing the training needs of rural mental health providers warrants attention.
Veterans Integrated Service Network (VISN) 16 is located in one of the most rural areas in the United States, including all or parts of eight southeastern and south-central states. It has over 50 CBOCs associated with 10 VAMCs. 15 VISN 16 serves 445,000 Veterans, over 80,000 with mental health problems, and more than half residing in rural settings. 8,15 The South Central Mental Illness Research, Education and Clinical Center (SC MIRECC), a virtual center within VISN 16, is dedicated to improving the provision of healthcare services to Veterans living with mental illness. 8 Its mission is “…to promote equity in engagement, access, and quality of mental healthcare for Veterans facing barriers to care, especially rural Veterans.”
This article describes the development, implementation and evaluation of a monthly Web conference training program for VA CBOC mental health providers.
Materials and Methods
With the support of VISN 16 leadership, the SC MIRECC developed and sponsored a distance-learning educational program known as the CBOC Mental Health Rounds. Justification for the project was based on the SC MIRECC's work with individual CBOCs and the results of the annual VISN-wide clinical education needs assessment of CBOC mental health providers, a short survey asking clinicians to rank their top training priorities. A strong value of the VA healthcare system is that clinical providers receive CE in new research findings and proven clinical practices. CBOC providers reported limited access to VAMC-based CE opportunities, primarily because of the significant time required for traveling to their parent facility for off-site training. In particular, providers desired educational activities that could help to fulfill their professional license requirements. Face-to-face training was considered optimal, conducive to the learning process and creating opportunities for networking. However, considering the distance to most education programs offered at their parent VAMC, the difficulties canceling clinics or arranging coverage to attend an off-site meeting, and tuition cost for a non–VA-sponsored educational event, clinicians were amenable to distance-learning formats that would allow them to remain in their work setting and have access to free CE opportunities. Also, given CBOC providers' busy schedules, 1-h trainings were preferred. Finally, providers were interested in and enthusiastic about topics pertinent to rural mental health.
To address the lack of CE activities available to rural providers, the CBOC Mental Health Rounds were developed. Using a live Web conferencing platform, the inaugural training was launched in November 2011. This system concurrently uses two separate technologies: (1) the VA National Teleconferencing System to carry the audio and (2) Microsoft® (Redmond, WA) Live Meeting (a subapplication of Outlook) to carry the visual (PowerPoint slides). Participants are able to ask questions and discuss the topic with the presenter, using the audio line. They are able to interact as well via their computer to answer polling questions, use the chat feature, and give feedback about the pace of the session. By agreement of clinical leaders, the VISN 16 clinicians were given release time for participation in the rounds. In July 2012, the series was expanded to VISN 6, the Mid-Atlantic Healthcare Network. VISN 6 has a strong interest in rural mental health and an established process for communicating with its CBOC clinicians. It serves over 320,000 Veterans at its eight medical centers and 27 CBOCs in North Carolina, Virginia, and West Virginia. 16
To ensure that the CBOC Mental Health Rounds address the unique training needs and interests of rural providers, an education planning committee was formed. The committee meets monthly and comprises CBOC providers from a variety of disciplines and VA Employee Education System (EES) staff. CBOC members oversee the planning process. They identify content, select topics, recommend speakers, establish objectives, ensure sessions adhere to licensure board criteria, review evaluations, and suggest areas for improvement. EES is the administrative body in the VA that supports employee training. EES provides guidance on execution of the project's activities, including registration, accreditation, marketing, preparing faculty for using the Live Meeting space, and troubleshooting technical issues. Collectively, members ensure that the sessions are high quality, meet standards for accreditation, and address topics salient to a broad range of rural mental health providers.
Despite the challenges of designing a curriculum to fit the needs of a diverse group of mental health professionals with varied expertise and work demands, the training series has entered its second year. The program is offered the first Wednesday of every month. Two weeks prior to each month's session an announcement is sent to mental health providers, medical center directors, and other VA employees via e-mail. The message includes a description of that month's educational session, a registration link, and dates and topics of upcoming trainings. This same information is also posted on a Sharepoint site within the VA system and the SC MIRECC Internet Web site. Ongoing reminders are sent during the 2 weeks leading up to the session. The presentations are 1 h in length, including time for questions and discussion.
CE units (CEUs) are available for nurses, physicians, psychologists, social workers, and other healthcare professionals. To receive CEUs, participants are required to pass an online post-test with a minimum score of 80% correct. The post-test comprises 10 multiple-choice and true/false questions, based on that month's topic. In addition, participants are invited to complete an online post-training evaluation. The 26-item questionnaire concentrates on participant satisfaction with the trainings' content, objectives, job impact, and learning environment. Most questions are on a 5-point ordinal scale, ranging from strongly disagree (1) to strongly agree (5). Four questions are open-ended, giving participants an opportunity to give feedback regarding the strengths and weaknesses of the session itself and the technology.
Results
During its first year of implementation, 11 CBOC Mental Health Rounds were offered to 397 unique participants. The sessions were attended by VA employees from various disciplines. Social workers represented the predominant discipline in attendance (Fig. 1).
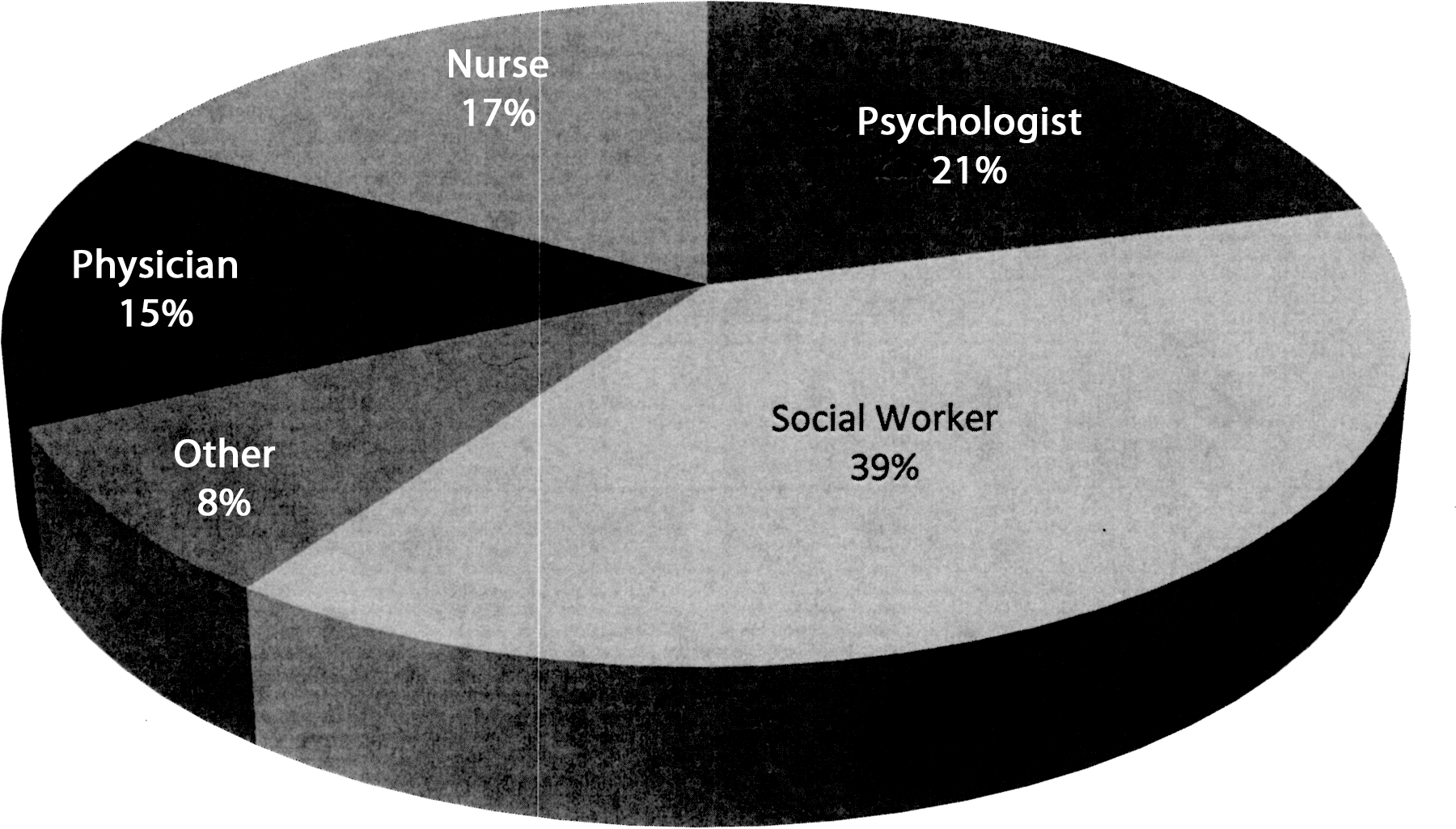
Community-based outpatient clinic Mental Health Rounds participants, by discipline.
Overall, 89–98% of participants agreed that the presentations were a satisfying learning activity that they would recommend to others (Table 1) Most found the content of the trainings appropriate, noting that topics such as ethics met specific CEU needs for licensure renewal.
The learning environment was evaluated primarily through questions about the Web conferencing technology. More than 87% of participants reported overall satisfaction with the technology, and 86% found it easy to use. Being able to access the programs from their workstations was considered a plus by many participants. Despite being generally satisfied, participants often reported that improvements needed to be made in ease of use of the technology. Technical problems included delays dialing into the teleconferencing system, background noise from participants who did not mute their phone during the presentation, and becoming unexpectedly disconnected during a training session. These participants suggested more technical support be made available during the meetings to address system problems (Table 1).
Mean Program Evaluation Scores and Percentage Agreement, Based on 11 Sessions
The rating scale ranged from 1 (strongly disagree) to 5 (strongly agree). The percentages represent the percentages of participants who agree or strongly agree with each of the statements.
Session titles were as follows: A, Suicide Prevention in Rural Settings; B, Ethics for Rural Providers; C, Tips for Recovery in Rural Settings; D, Providing Recovery Oriented Care in Rural Settings; E, Stress Management for Rural Providers; F, Ethics, Social Media and Rural Practice; G, Managing TBI [Traumatic Brain Injury] Among Veterans in Rural Settings; H, Spirituality and Mental Health in Rural Settings; I, Couples Therapy in Rural Practices; J, Treating Rural Veterans with TBI and PTSD [Posttraumatic Stress Disorder]; and K, Engaging Families in Recovery.
The trainings had a positive impact on participants' jobs. Over 91% reported that they are/will be able to apply the knowledge and skills learned in the sessions to their current position. Additionally, over 81% of participants reported that the learning activity will improve their job performance. Up-to-date information on evidence-based therapies, clarification of VA policies and procedures, and research trends were considered useful by many participants.
The provision of CEUs was a major motivation for the development of the program. Across all 11 sessions, an average of 87 participants registered for the trainings. It is surprising, however, that only 49 participants on average passed the post-test and that even fewer (46 participants) completed the post-test evaluation, which is required to obtain CEUs.
Discussion
The CBOC Mental Health Rounds provide mental health providers with a live Web conferencing training opportunity. The format enables participants to improve their knowledge of evidence-based practices and rural mental health issues, strengthen clinical skills, and receive accredited hours that can be reported toward professional licensure. In addition, distance-learning opportunities reduce cost in staff travel time and absences associated with distant on-site programming.
Participants ranked their overall satisfaction with the trainings in the 89–97% range for each session. Because of the diversity of the learners in terms of discipline and geographic location, the sessions have spanned a variety of rural mental health topics. For example, suicide is a major concern for Veterans in rural areas, where suicide rates and risks exceed those of urban dwellers. 17 The opening presentation, “Suicide Prevention in Rural Settings,” enhanced participants' skills in developing and implementing a safety plan. A later presentation on spirituality compared and contrasted the roles of CBOC mental health providers and local clergy in providing support for Veterans and their families. A range of presenters, including CBOC practitioners and national leaders, may have also contributed to overall satisfaction.
Several studies indicate that rural providers experience difficulties accessing CE. 1,4,18 Web conferencing has been shown to be an effective alternative to face-to-face training because of its cost-efficiency and convenience for rural providers, who would otherwise need to travel far distances for training. 18,19 Although much data exist to support the cost efficiency of Web conferencing for telehealth, data on the cost efficiency of Web conferencing for CE are scarce. However, some studies indicate that providing CE via a Web conferencing format can save hospitals in travel (for both the speaker and attendees) and loss of productivity of hospital staff, as well as facility costs. 2 By participating in the CBOC rounds, clinicians were able to access CE opportunities at their own sites, eliminating time lost to travel and minimizing disruptions to the care of their patients.
Just as in previous studies, we found that rural providers were satisfied with the Web conferencing format for CE. Like those in other settings that offer Web conferencing, 18 our participants sometimes encountered technical difficulties, including poor audio quality and interfering background noises caused by unmuted microphones from other users. Offering consistent and reliable technical support in troubleshooting issues with technology may help to decrease frustration and, over time, improve ease of use. 1,18 We found that, despite the challenges with technology, participation in trainings remained consistent across all sessions offered, indicating that technology was not a major barrier.
Results indicate that providers have found the CBOC Mental Health Rounds valuable to their job performance. Providing relevant and useful CE opportunities is integral to providing competent and state-of-the-art care. Identifying training needs and selecting content were the responsibility of the planning committee. Perhaps being clinicians themselves helped the committee members select topics of value to their peers.
Only participants interested in obtaining CEUs are required to complete a post-test. Given the lack of educational opportunities frequently reported by rural providers, the low rate of participants who applied for credit is surprising. Several barriers may inhibit completion. First, completing the post-test requires several steps—participants must exit the Live Meeting, log into the EES Web site, locate the course title, click on a link to the post-test, and complete and submit it. Participants would sometimes contact EES or the series coordinator regarding problems with the post-test immediately following a Web conference. Some problems encountered when attempting to access the post-test immediately following the Web conference included unavailability of the post-test and incomplete display of questions. Participants who do not immediately complete the post-test may find it difficult to later fit it into their full clinical schedules. Although participants can retake the test until a passing score is attained, waiting several days or even weeks to take the test may contribute to failing scores. Finally, post-tests are available for completion for only 4 weeks following training. Efforts to increase the rate of post-test completion are being investigated. Post-training e-mail messages are now being sent to registrants encouraging them to complete the evaluation and obtain CEUs. In addition, training slides are made available for review and download before the training, during the training session itself, and post-training. EES is exploring ways to streamline the process.
Although this study provides insight into the implementation of and satisfaction with a Web-based CE program, it had several limitations. One limitation is that data were based only on responses from participants who elected to respond to the survey. Additionally, because participants were evaluated one time post-training, there were no means of tracking knowledge transfer. Likewise, because of the anonymity of the survey, no information is available as to who completed the evaluations, and there is no information as to provider overlap. Furthermore, because we lack follow-up data reporting on the effectiveness of the training, we cannot make judgments as to how effective the trainings were.
Conclusions
Evaluations of the CBOC Mental Health Rounds indicate that the program has been well received. Using a Web conferencing platform, it has delivered relevant and convenient training to rural mental health providers. However, continued attention must be paid to providing responsive technical support to users experiencing problems and mechanisms to obtain CEUs.
The program's early success and the needs of its unique audience have prompted the VA Office of Mental Health Services to recommend national expansion. The program has incrementally grown to now include 5 of 21 VISNs and 20 states. As its reach extends to a national audience, the live educational sessions will be offered twice, on two different days of the week and at two different times of day, providing easier access to providers. Continued efforts to evaluate the merits of the program will be made, particularly its impact on patient care.
Interest in Web conferencing is expected to continue to grow. Although the platform can be cumbersome, it has several advantages, including easy access and an interactive learning environment. With many governmental agencies reducing travel budgets for face-to-face meetings, Web conferencing provides a lower-cost mechanism for education and training in large community-based public healthcare systems.
Footnotes
Acknowledgments
This work was partly supported by the Office of Research and Development, Veterans Health Administration, Department of Veterans Affairs, and the Houston VA Health Services Research and Development Center of Excellence (HFP90-020) and the South Central MIRECC.
Disclosure Statement
No competing financial interests exist.