
Abstract
Introduction
The American Telemedicine Association (ATA) was established in 1993 as a nonprofit organization to bring together groups from medicine, academia, technology and telecommunications companies, e-health, m-health, medical societies, government, and others to overcome barriers to the advancement of telemedicine. A key activity of the Association is to educate government and the public about telemedicine in order to validate its role as an essential component in the delivery of modern medical care by creating the basis for assuring uniform quality in the delivery of remote healthcare services, particularly via the efforts of the Standards and Guidelines Committee.
The first set of guidelines developed by the ATA was created for Telepathology in 1999. 1 In 2004 the ATA Ocular Telehealth Special Interest Group (SIG) developed and published the first formal set of ATA practice guidelines, addressing diabetic retinopathy. 2 Since then, standards and guidelines documents have been developed for a variety of applications, including teledermatology, telemental health, home telehealth, and general store-and-forward and real-time applications, each addressing technical, administrative, and clinical aspects. 3 The ATA continues to develop standards and guidelines documents based on critical assessments of the field of telemedicine and feedback from its membership base, including SIGs, institutional members, and corporate partners. 4
The Committee's mission does not end with simply developing the standards and guidelines documents. It is incumbent upon each Working Group to create a dissemination plan that will make the documents accessible to as many users as possible and assist practitioners in pursuing a sound course of action to provide effective and safe medical care founded on current information, available resources, and patient needs. Additionally, dissemination efforts include getting the ATA guidelines adopted by national medical societies, federal and state regulators, and payers. Posting the completed Standards and Guidelines documents on the ATA Web site is the key mode of dissemination. Over a 2-year period while collecting data, before being given access (all guidelines are free) to a requested document, it was necessary to fill out a short survey that included questions on how you planned to use the requested guideline, what the most important information you were seeking, whether your telemedicine program was active, what technologies were being used, healthcare sector, healthcare position, and basic demographics (all were optional).
In 2012, the ATA recorded over 500 standards document downloads per month. The Telemental Health Practice Guideline was the most commonly downloaded document, being accessed approximately 100 times/month. Of those who responded to the survey, most were physicians or PhD-level professionals who were not currently using telemedicine but were considering using it in the future. Primarily respondents were from academic health institutions, nonacademic medical centers, and independent practice; however, government agencies were found to download the documents as well. When asked how the guidelines were to be used, the majority of respondents indicated the guidelines would be used for clinical, administrative, and research guidance. The other commonly downloaded ATA guidelines documents included telepresenting, diabetic retinopathy, teledermatology, telerehabilitation, and core standards. These ATA guidelines documents are also being accessed regularly by a broad range of people and are primarily being used for clinical, administrative, and research guidance, in that order.
Although this basic information was useful, it did not provide information about how those engaged in telemedicine regarded standards and guidelines, their utility, or their effectiveness. Periodic review of clinical standards and guidelines is critical and often incorporates feedback from users in addition to the expert opinions of the developers. 5 –8 In order to assess awareness, utilization, and impact of the completed ATA standards and guidelines initiatives on the telemedicine industry, the following survey-based study was conducted.
Materials and Methods
A logic-branching survey was developed by the ATA Standards and Guidelines Committee and distributed via SurveyMonkey. The survey consisted of 26 core questions. The majority of the questions were yes/no or multiple choice (with an “other” option where text could be entered). For the multiple choice questions, respondents could select multiple responses. Three questions were text-entered responses only, and one asked for contact information (optional). An e-mail blast using an ATA database was sent to 13,177 ATA members and nonmembers in November 2011 advertising the survey and providing a link to the SurveyMonkey site. Nonmembers are in the database primarily because they have registered for and attended an ATA meeting in the past, and the registration process includes providing their e-mail address. A reminder blast was sent after 2 weeks. Results were compiled and analyzed after a 90-day open period for responses to be submitted. The response data were analyzed using summary statistics.
Results
There were 538 (4%) responses to the survey received, and, in total, 449 (3.4%) were completed. Of those who completed the survey, 73% were ATA members, and 27% were nonmembers. Ninety-six percent were from the United States. Participants were primarily healthcare providers (30.8%) and administrators (24.4%) coming from a wide variety of clinical specialties. Most (21.9%) were in telemedicine programs that had been active for 2–5 years or over 10 years (Fig. 1). Seventy-five percent were not a member of a standards and guidelines committee or work group that works on or is responsible for standards and guidelines in telemedicine, and of those who were a committee member, 31% were on an ATA committee or in an SIG interested in or working on guidelines.
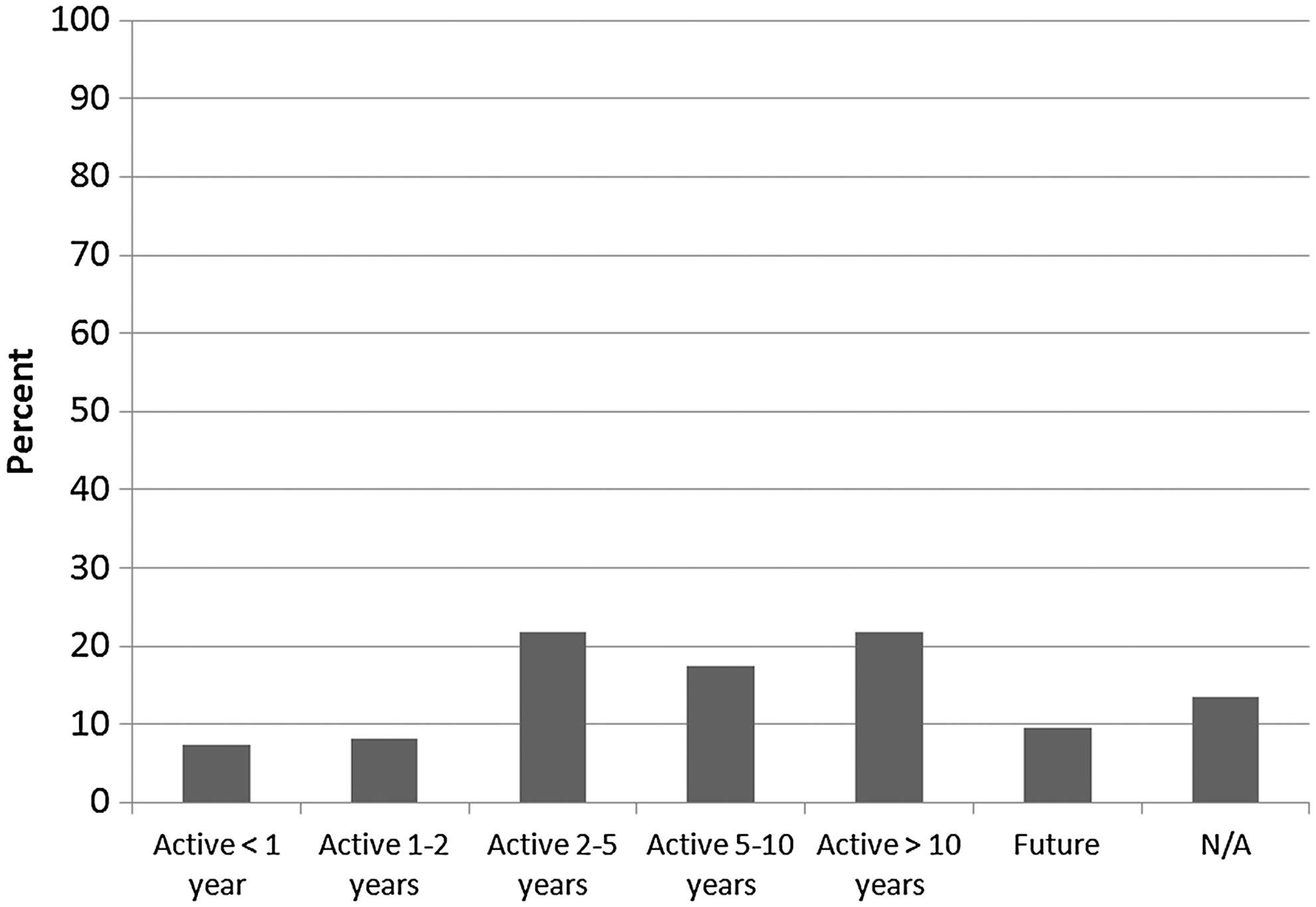
Number of years respondents have been active in telemedicine. N/A, not available.
The majority of respondents (96.5%) believe the practice of telemedicine/telehealth should have standards and guidelines. The top three most common reasons were “adds credibility to practice via telehealth,” “standardizes approach to practice via telehealth,” and “decreases liability.” The summary of all responses is shown in Figure 2. The “other” responses were grouped into the following common categories: patient safety, consistency, quality of care, patient/provider satisfaction (n=45); promotion and enhancement of telemedicine (n=17); research, outcomes, evidence-based practice, legitimizes telemedicine (n=11); helps with legal and policy (n=6); helps with reimbursement and cost-effectiveness (n=5); or all of the above (n=3).

Reasons why respondents believe there should be standards and guidelines for the practice of telehealth. Respondents could select more than one answer.
For those who did not believe (3.5%) there should be standards and guidelines for telehealth, the reasons (multiple could be selected) were as follows: don't want outside groups defining quality in telemedicine (58.8%), liability increases when standards are in place (41.2%), too burdensome (41.2%), too complex to create (29.4%), not needed (23.5%), and other (52.9%). Of those selecting other, five noted that telemedicine is no different than traditional practice for which guidelines already exist, and four said standards would be a barrier to innovation and growth.
The majority of respondents indicating a need for standards and guidelines said the ATA (78.7%) and other professional societies/associations (74.5%) should be responsible for development. A summary of all responses is shown in Figure 3.

Responses to who should be responsible for developing standards and guidelines for telehealth. Respondents could select more than one answer. ATA, American Telemedicine Association.
If standards and guidelines were in place, the top uses reported included guidance for clinical practice (87.5%), training (73.5%), gaining reimbursement (54.8%), research purposes (42.2%), and other purposes (19.2%), including product development and interoperability (n=13), quality assurance (n=9), education and certification (n=9), and program development and optimization (n=8).
Sixty-three percent of respondents indicated they were aware of guidelines for the practice of telehealth, including those developed by the ATA (74.6%), professional associations (42.3%), individual organizations (30.9%), federal agencies (27%), state agencies (20.5%), payers/reimbursers (15%), and other (8.8%) such as the military, NATO, and other international bodies. There were 267 entries by respondents when asked to list specific practice guidelines or standards they are using for telehealth. The majority (21.5%) are using in-house (e.g., hospital, company)-developed guidelines, followed by those from professional associations/societies (20.4%) and those developed by the ATA (18.2%). Figure 4 shows all of the guideline categories listed.
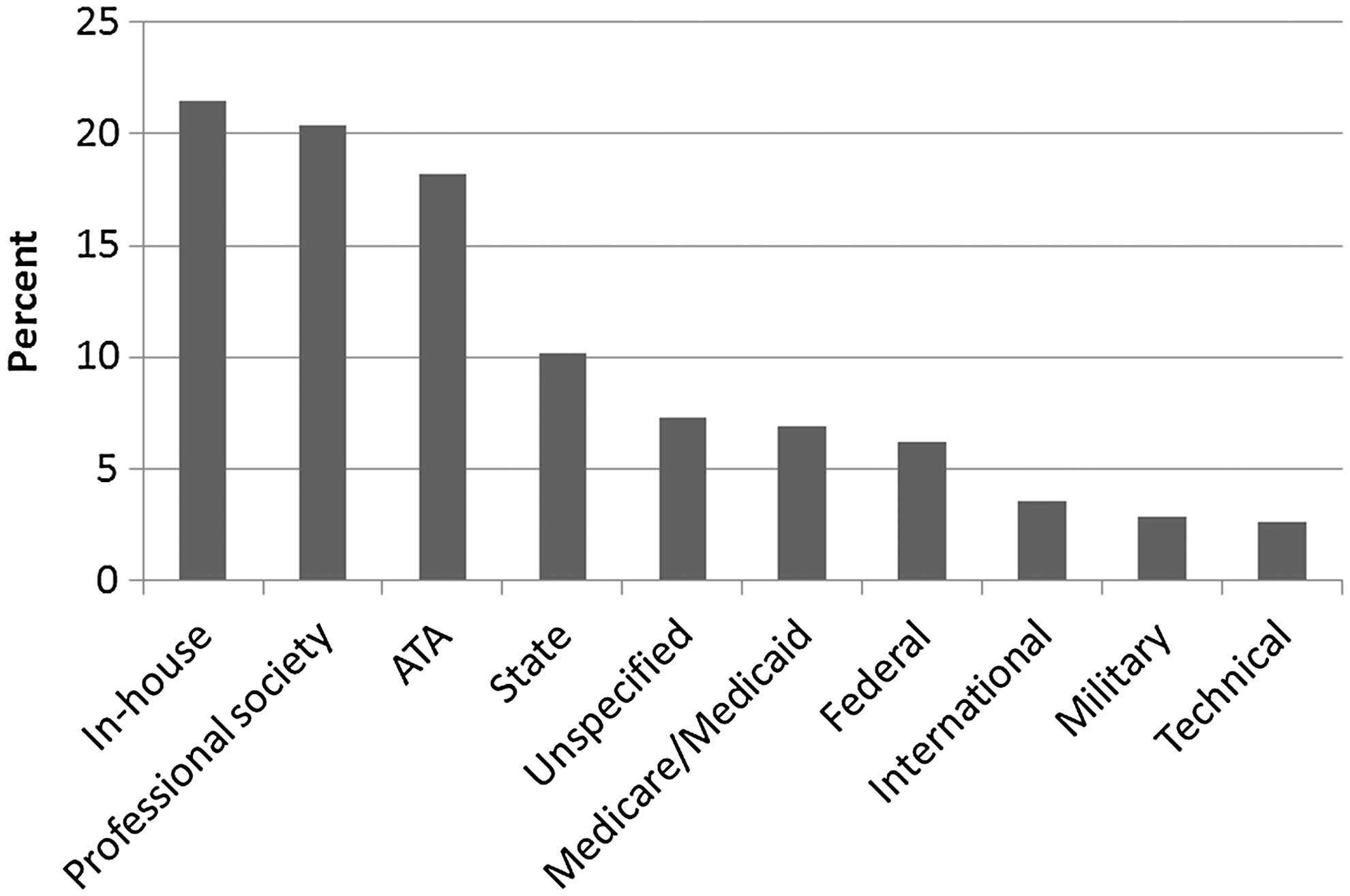
Categories of standards and guidelines respondents listed as currently being used. Respondents could select more than one answer. The following definitions were assumed: In-house, developed internally by a hospital, company, or other organization; Professional society, a professional association or society such as the American Psychological Association; State, developed by a state or state-affiliated organization (State Medical Board); Unspecified, general category such as teleneurology provided without other details; Federal, a federal agency such as the Food and Drug Administration or National Institutes of Health; and Technical, DICOM, Continua, etc. ATA, American Telemedicine Association.
Among respondents, 86.3%were aware that the ATA has a Standards and Guidelines Committee and that ATA has published standards for the clinical practice of telemedicine. Of these respondents, 64.4% indicated they had used ATA's published practice guidelines, with the Core Standards document being the most frequently used (57.7%). The guidelines most commonly used are shown in Figure 5. Guidelines were being used for clinical guidance (70.6%), administrative guidance (61.3%), technical guidance (48.5%), training guidance (48.5%) research guidance (19%), and other (11%).
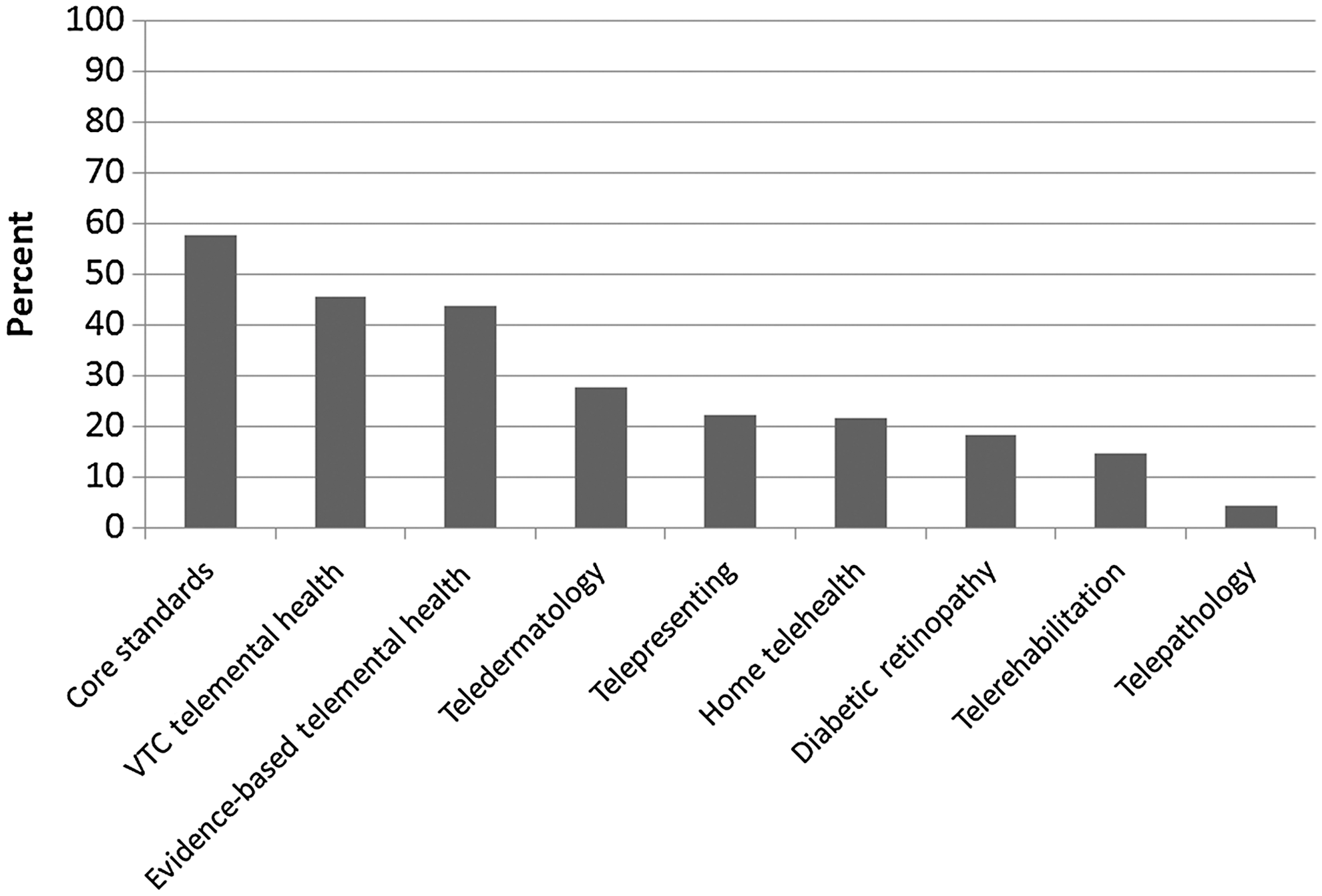
American Telemedicine Association standards and guidelines that respondents listed as currently being used. Respondents could select more than one answer. VTC, videoteleconferencing.
The main reasons respondents found the ATA standards and guidelines to be helpful are shown in Figure 6. When asked about what impact ATA's standards and guidelines were having on the way they provide healthcare, the responses were improved provider acceptance and understanding of telehealth (79.8%), improved patient outcomes and quality of care (63.2%), improved access (44.8%), provides information to justify reimbursement for payers (37.4%), and reduces costs (26.4%).
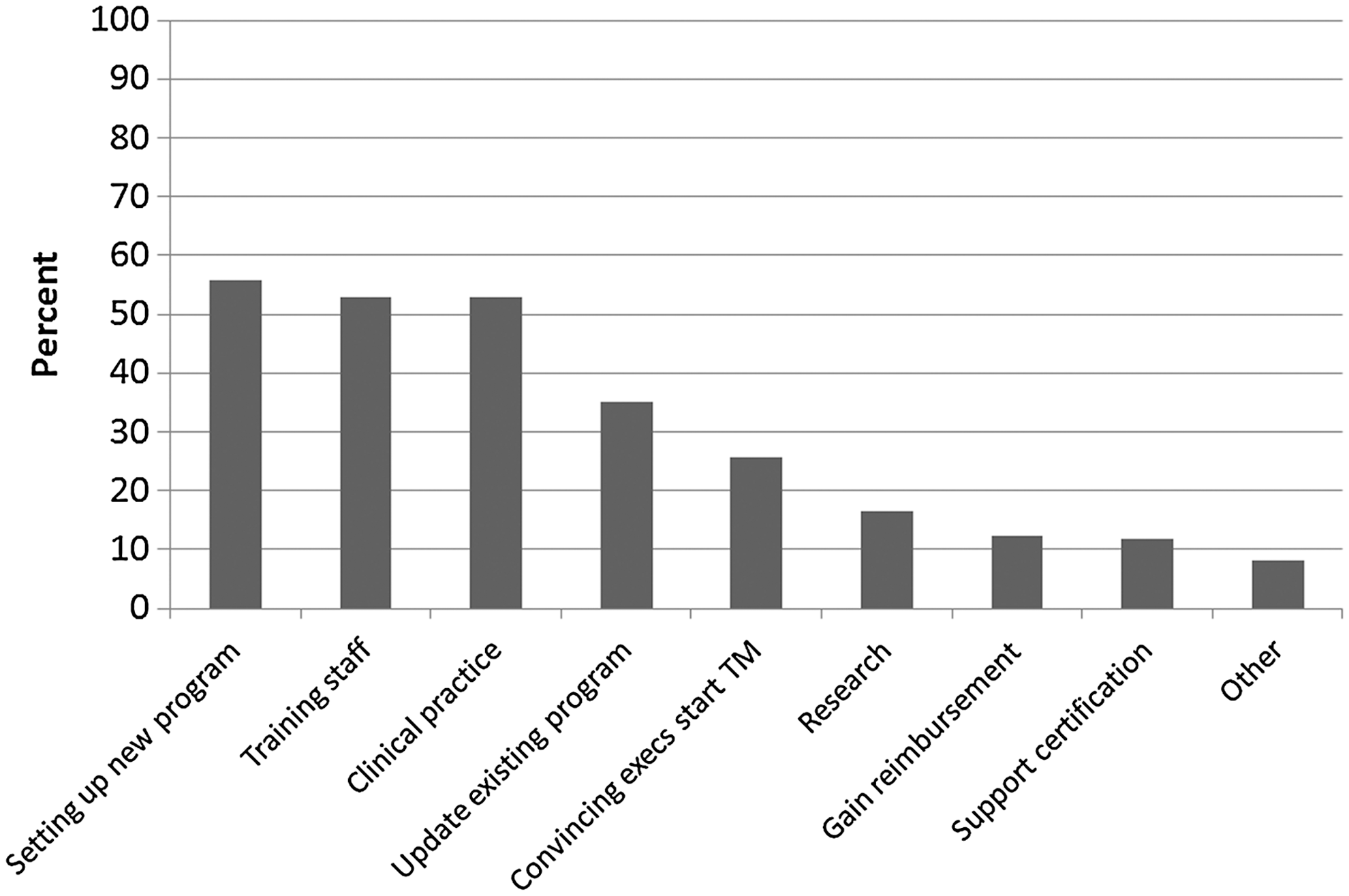
The main reasons respondents found the American Telemedicine Association standards and guidelines to be helpful. Respondents could select more than one answer. TM, telemedicine.
Respondents were asked to identify gaps or areas where standards and guidelines were needed. The top response (n=113) was guidelines for specialty applications such as stroke, home health, teleprescribing/pharmacy, mobile health, primary care, pediatrics, emergency medicine, acute and urgent care, and tele-intensive care unit (a complete list is given in Table 1). Other areas included reimbursement (n=18), technical (n=23), interstate practice (n=10), and other (n=27).
Specialty Application Responses to What Practice Standards or Guidelines, If Any, Do You Feel Are Lacking in the Current List of Available Standards and Guidelines Developed Through the American Telemedicine Association or Other Organizations?
COPD, chronic obstructive pulmonary disease; EMR, electronic medical records; ICU, intensive care unit; SNF, skilled nursing facility.
Discussion
Overall, the survey results indicate the ATA clinical practice guidelines documents are being regularly accessed and used in both public and private sectors. It is interesting to note that the majority of respondents are using guidelines that have been developed in-house. There are likely several reasons for this, even given the fact that guidelines from the ATA and professional societies account for a substantial number of guidelines used (see Fig. 4) and nearly 97% of respondents indicated that the practice of telemedicine/telehealth should have standards and guidelines. One reason could be that published guidelines for every clinical scenario and telemedicine application simply do not exist (and likely do not even exist for the traditional form of a given application) so by necessity they are developed in-house. It may also be that, despite the fact that respondents feel there is a need for guidelines in telemedicine, traditionally clinical practice guidelines have had only a limited effect of changing clinicians' behaviors so users may feel wary of guidelines developed outside of their organization that may only be applicable in a general sense or difficult to integrate into the local environment and workflow. 9 –12 One way that has been found to be effective for promoting adoption of clinical practice guidelines is to adapt them to the local context and situation, 13 and that seems to be what many practitioners of telemedicine are doing by developing or adapting existing standards to in-house practice and use applications.
Clinical guidelines development has increased in recent years, and the field of telemedicine is no exception. It can, however, be quite difficult as noted to determine whether or not developed and published standards and guidelines are actually being implemented. For example, a recent review was designed to evaluate the effectiveness of strategies to implement clinical guidelines for chronic disease management in primary care in European Union member states. 14 The authors searched five databases for studies focusing on the management of chronic diseases in adults in primary care and found a total of 21 studies that fit their selection criteria. They found that the implementation strategy was fully effective in only four (19%), partially effective in eight (38%), and not effective in nine (43%) of the reports. Only one study provided data on barriers to implementing guidelines, noting a lack of awareness and agreement about clinical guidelines.
In some circumstances, the use of clinical guidelines is affected by the nature of the guidelines and their attributes. For example, Grol et al. 15 assessed the use of 47 different guidelines and found that recommendations were followed overall in about 61% of decisions. Controversial recommendations were followed less often (35%), as were vague and nonspecific recommendations (36%). Recommendations that required a change in existing practice routines were followed only 44% of the time, and evidence-based recommendations were used more than those not based on research evidence (71%). It is important to note that the ATA standards and guidelines development process 4 includes a rigorous review of the literature on the topic under development that involves scoring the literature according to the well-established American Psychiatric Association's 16 practice guideline development process, which codes studies on an A–G scale where A is a randomized, double-blind clinical trial and G is other (opinion-like essays, case reports). These study codes are then used to formulate the language used in the guidelines, where the key word “shall” indicates a mandatory requirement, statement, or action, whereas “should” indicates a statement or action that is very highly recommended and “may” indicates a statement or action that is recommended but optional based on specific scenarios and applications.
It is also interesting to note that although overall the respondents reported that they are aware of the various guidelines available, Table 1 shows that this awareness may not be as high as reported. Table 1 shows the gaps or areas where standards and guidelines were needed according to respondents. It is surprising that responses included gaps for which standards and guidelines are already available! For example, the ATA already has guidelines for the general practice of telemedicine, telemental health, teledermatology, home telehealth, telerehabilitation, and teleophthalmology. The American College of Radiology has guidelines for teleradiology, and the Centers for Medicare and Medicaid Services have some guidelines for e-prescribing. All of these were listed as guidelines people feel are needed. It may be that users are indeed unaware of these existing guidelines, but it also may be that they are aware of them but feel they do not address a particular aspect of an application in which they are interested. For example, telerehabilitation covers a very broad spectrum of applications, and the existing ATA guideline provides a rather global set of guidelines not specific, for example, to speech pathology. The ATA and other professional societies continue to develop guidelines for an ever-increasing number of applications so it seems likely that most of these gaps will be addressed in future guideline and standards documents.
In summary, ATA's standards and guidelines are being accessed and utilized by providers and programs in the United States and abroad. In general, these guidelines are being used to improve practice and quality, guide the development of new programs, and train staff. Professionals in the field are aware of ATA's practice guidelines, and ATA is regarded as the leader in the development and publication of these for telemedicine/telehealth practice.
Users of these guidelines primarily use them for clinical practice, administrative rules, technical specifications, and research guidance, to train staff, and to convince practitioners to use telehealth and for organizations to implement enterprise telemedicine/telehealth initiatives.
Practitioners of telemedicine believe that standards and guidelines are needed for guidance for clinical practice, training, gaining reimbursement, and research, and they use those developed by professional organizations such as the ATA as well as those developed by their own institutions. There are several specialty areas that respondents identified as applications where new standards and guidelines would be useful, and the ATA is actively seeking support and volunteers to work on the development of new standards and guidelines documents.
It should be noted that this study does have limitations. One limitation is that it is survey-based, and thus the data are self-reports. Another limitation is that although we asked users if and how they are using the various guidelines available for telemedicine applications, we did not ask them about whether or not these guidelines actually impact patient care, the process of providing care, or patient outcomes as a result of the telemedicine interventions using the guidelines. This would be any interesting topic for a future study. The low response rate (4%) is also a limitation. Ideally we would have liked a response rate of at least 10%, but even with follow-up reminders we did not reach this goal. There are several reasons why this might have occurred. One may be that not all requests on the e-mail blast reached the intended audience—some e-mails might have been incorrectly recorded in the database, some may not have been current, and so on. Another reason may be that the ATA has a very diverse membership, including clinical practitioners, technologists, engineers, business managers, researchers, and many others. Not all those involved with telemedicine may use or even be aware of the use of standards and guidelines that are more clinical application-oriented so they may not have wanted to or felt it was appropriate to respond to a survey on this topic.
A possible confound may be that 25% of the respondents reported that they had been part of a guidelines development process or committee. This does not mean that they are necessarily involved in the ATA development process, but they could be involved in any guideline development process in some other professional society or within their own institution. Given the nature of the field of telemedicine and the fact that so many applications are being initiated at so many institutions, it is actually not surprising that numbers of respondents were/are involved in guidelines development. Given the data, it seems likely that the majority of the respondents who said they were involved in a committee were involved in a local institutional committee, as the majority (21.5%) are using in-house (e.g., hospital, company)-developed guidelines.
The current ATA guidelines can be found online (
Footnotes
Disclosure Statement
No competing financial interests exist.