
Abstract
Introduction
Over the past several decades, the development of specialized palliative care (SPC) teams (SPCTs) has taken place in Denmark as well as in many other countries. The SPCT, typically placed in close connection with larger hospitals, visits patients in their homes and provides telephone consultations and support to patients, relatives, and professionals working with palliative care.
The work of the SPCT is often challenged by the long distances between the patients and the hospitals and by the substantial amount of time spent driving to and from the patients' homes. A solution to these challenges is telemedicine (i.e., the transmission of information and communication with the possibility of visual contact between the specialist and patient and shared information in electronic files or even chat rooms). 1,2 Additional possibilities of diagnostic or monitoring electronic tools are also available.
A variety of telemedicine is increasingly being used in healthcare—and also in palliative care 3 (e.g., telephone support, videoconferencing for interactive case discussions, consultations and assessments, and healthcare staff education). 4 Also, digital pens for symptom assessments have been tested in palliative care with positive outcomes in relation to symptom control and patient satisfaction. 5,6
In Denmark, however, SPCTs have little or no tradition for using modern telecommunication (in this study defined as communication via technologies other than a common phone [without a visual signal]). Technical, professional, and emotional barriers toward an implementation may exist, particularly in relation to what is regarded as “good communication.” The quality of the communication is an important issue in palliative care.
Previous studies have indicated a positive effect of the implementation of modern telecommunication (e.g., videophones) in palliative care, 7 –13 but only very few, 10,14 –16 and no Scandinavian, studies have to our knowledge been published on the attitudes of professionals toward modern telecommunication in palliative care.
The aim of this study was to gain knowledge of the Danish SPCT professionals' views on the communicative aspects of “modern telecommunication.”
Materials and Methods
This study was based on four semistructured group interviews with 17 health professionals from three different SPCTs in the Central Denmark Region conducted from November 2009 to March 2010.
According to the Scientific Committee for the County of Aarhus, Denmark, the Biomedical Research Ethics Committee System Act does not apply to this study because it does not include implications for patients.
Setting
The Central Denmark Region (1.2 million inhabitants) had at the time of the interviews five SPCTs, each connected to a hospital (one university hospital and four regional hospitals) and covering a geographical area of 13,000 km2.
An SPCT with physicians, nurses, and other healthcare workers is available during business hours in major hospitals in Denmark. Doctors (general practitioners [GPs] or hospital doctors) can refer patients to these teams or ask for advice in specific cases.
Sample
The informants included doctors (n=5), nurses (n=9), and physiotherapists (n=3) in three palliative care teams in Herning, Randers, and Aarhus (Table 1). The teams were chosen according to their distance to the University Hospital: one team was based at the University Hospital in Aarhus, one in a major city (Randers) that is 30 km from the University Hospital, and one team (Herning) was based farther away (85 km) from the University Hospital.
Demographics of Participants in the Interviews
Primary education (i.e., nurse, physiotherapist, medical doctor).
IQR, interquartile range; SPC, specialized palliative care.
We invited all 7 doctors, 12 nurses, and 3 physiotherapists working in the three teams to participate in four interviews. The main reason given by the professionals for not participating was lack of time. One of the authors (M.A.N.) works as a consultant in one of the SPCTs and was therefore not included as an informant.
Group Interviews
All interviews were conducted by J.E.W. and supervised by M.A.N., who is experienced in qualitative research. Data concerning the participants are presented in Table 2. The interviews lasted from 84 to 88 min and were guided by a topic guide designed on the basis of clinical experience, consensus discussions among the authors, and literature studies. The main themes covered in the interview guide and examples of questions inspired by strengths, weaknesses, opportunities, and threats analysis can be seen in Table 3. 17 The topic guides were revised after each group interview to allow the inclusion of new themes. However, no major changes were made in the topic guide during the interview process.
Distribution of Informants in the Group Interviews
Topic Guide Themes in Interviews with Professionals
GP, general practitioner.
The interview began with an introduction of the participants and interviewers, and information about anonymization and publication was given and accepted. Open-ended questions were used. 18 A summary was given at the end of each group interview to obtain an immediate validation of the issues raised.
Analysis
The research approach chosen was qualitative description, based on the work of Sandelowski, 19 as we wanted to present the facts from the informants' point of view and to stay close to the data. 20,21 The group interviews were transcribed verbatim by a trained secretary, and all transcripts were read repeatedly to gain an overall impression before initial coding. 18 All meaningful text units were identified and coded. We subsequently examined and grouped all the text units into 10 main categories that were labeled with a name (Fig. 1). The information in each main code was then examined and grouped into three main categories. By doing so, we allowed the main categories to evolve from the data instead of imposing a framework a priori. 22
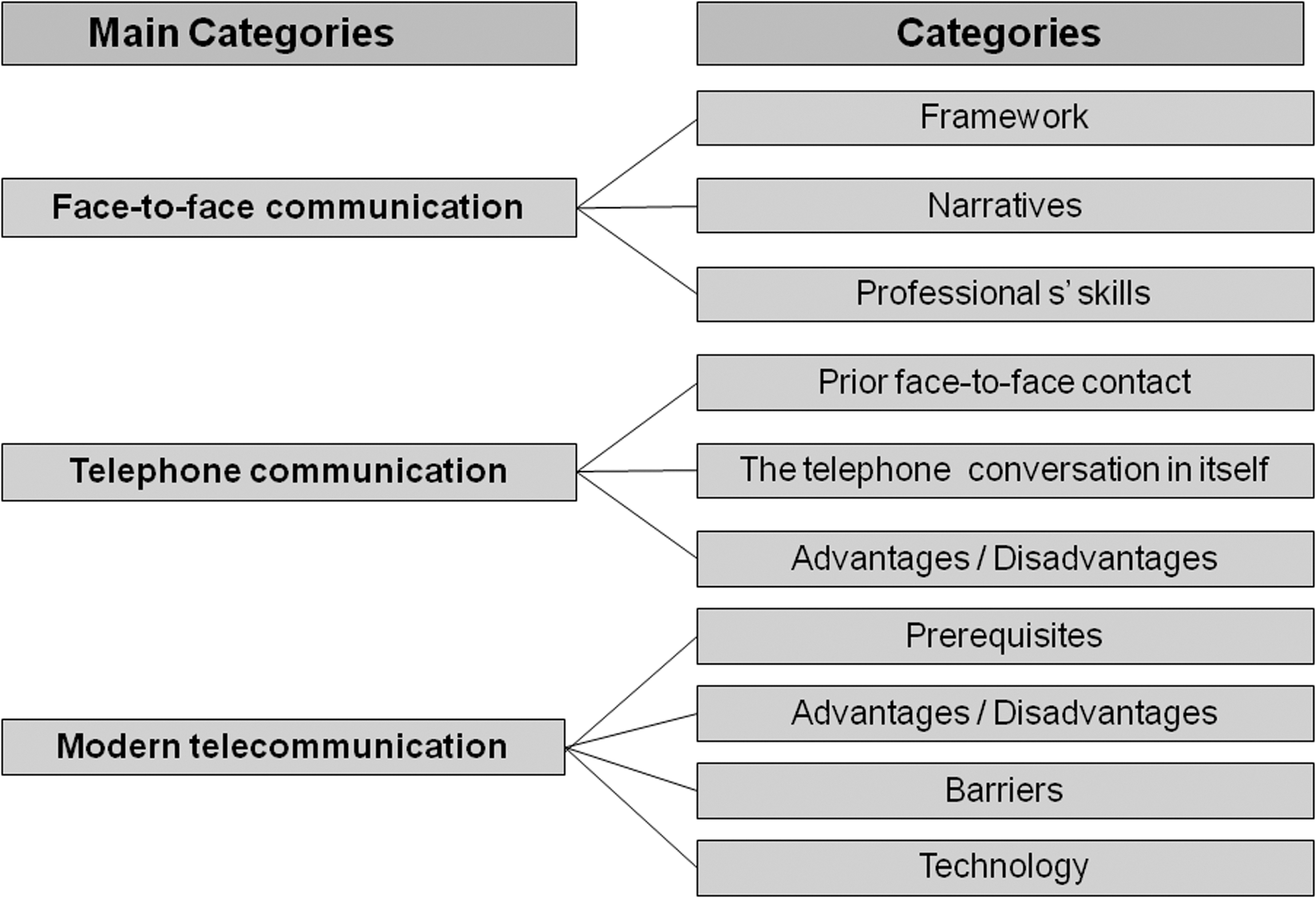
Categories that emerged from the analysis.
Results
In the group interviews, there was overall agreement that good communication is essential for good palliative care:
I find it absolutely essential—because if we don't communicate properly, it doesn't matter how professional we are. (Interview 1)
It was clear in the interviews that none of the respondents had professional experience with telecommunication besides regular telephone consultations. We found three main categories describing different aspects of the investigated issue: “face-to-face communication,” “telephone communication,” and “modern telecommunication” (Fig. 1).
Face-to-Face Communication
The informants underlined that good communication and the patient–professional relationship had to start with face-to-face contact and that this personal meeting was a prerequisite for the future communication in any form:
Because I think that there is a huge difference between whether you are in direct “face-to-face” contact or are in telephone contact. They are two completely different ways of communicating…(Interview 1)
In regard to face-to-face communication, the informants mentioned that three themes were essential for optimal communication: framework, narratives, and professional skills.
Framework
The participants emphasized the importance of creating a framework in which the face-to-face contact can take place, both the outer (setting) and the inner framework.
Outer framework. The outer framework (i.e., the setting) was very important for the professionals. It was often difficult to have the meeting in a busy and crowded hospital ward, as the patient may not feel safe or confident in this atmosphere.
We go into her hospital room and she is sitting behind the bedside table. There is a patient in the bed beside her who is all ears. We sit on the other side of the table and her hearing is not at all good. Needless to say, it wasn't a very good conversation. (Interview 1)
The informants agreed that the preferred location for the initial face-to-face contact was in the patient's home. In doing so, the professionals, in addition to the spoken word, acquired a lot of nonverbal information about the patient's background, life circumstances, coping mechanisms, roles within the family, and the relations among the family members:
You also get a different impression when you go into and see someone's home—the set-up, how well-off is the family, how untidy is it? You can get an idea of how they will tackle their situation. And one should never belittle the significance what is on the shelves and the paintings on the walls or the lack of them. Because they give us an overall picture of the family we are dealing with…. (Interview 4)
Home contacts were regarded as a possibility to establish a more equal balance of power between the patient and the professionals, in comparison with hospital contacts, as the professionals without discussion would be in a superior position at the hospital:
….when they (the patients) are here (in hospital), they feel stressed by the strange surroundings and they feel that they are guests. We are the “guests” when we visit them, i.e. they are the hosts, which implies another balance of power. We are there on their terms and they are more relaxed. (Interview 4)
However, coming into the patients' homes was not without challenges, as the participants mentioned that this “invasion” could be overwhelming in some cases:
…it gets a little too close for comfort—asking us in over the doorstep. (Interview 4)
Inner framework. The significance of the inner framework of the contact was underlined. It was important that the patient and relatives were mentally ready and prepared for the meeting and that they understood the language of the professionals:
They have to be mentally ready for us, to enable us to communicate well. (Interview 1)
The inner frame also entailed the professionals being well prepared and having allocated sufficient time for the meeting:
You must to be well prepared and have read up on the medical notes…to get a good dialogue going…. (Interview 4)
The informants also stressed the importance of everyone present having a joint and openly negotiated agenda for the meeting:
It is important to have a joint agenda—and that no one has a hidden agenda or that we turn up with an agenda that completely takes the relatives by surprise. (Interview 4)
The participants mentioned the following barriers to a good inner framework: certain personality traits (e.g., pedantry), patient's anger, language barriers, patient's previous experiences with poor patient–professional communication, and overly high expectations toward the professionals from the patient/family:
I find it hard to connect with angry people. But it is all part of the training,…one needs to keep training to accommodate the feelings one encounters. (Interview 1)
Narratives
The participants emphasized the importance of patient narratives and the professionals' responsiveness toward them. By allowing the patients to take their time to reveal their life story, the professionals felt that both the patients and professionals could appreciate the patients' situation in a larger context:
As a young woman said—it was nice to meet some people who could see the whole picture and not just the fragmented details. Something she had not experienced on the hospital ward she was in. (Interview 2)
Professional skills
The participants all agreed that good face-to-face contact requires that the professional has specific skills—good technical communication skills, presence in the situation, but also neutrality and not becoming too personally involved:
… making sure that one doesn't get overly involved or the reverse. It really is an art…. Of course one must be able to “like” the patient, but also be the one who can “withdraw.” And the reverse, if you have a patient that you dislike, that you sort of force yourself to connect with the patient in spite of the obstacles. (Interview 1)
Furthermore, good communication requires perseverance and the ability to understand the interaction as a process that takes place over time and several encounters:
There was a sort of despondency about this family—there was something we hadn't managed to cover. And this is where the procedure steps in, to find out what this is all about, this reserve or the eyes full of tears. And we can't start drilling them the first time about what is going on here. This is a question of procedure and the time it takes for it to turn into a good experience. (Interview 1)
Telephone Communication
The participants all agreed that the telephone was an important tool in palliative home care, not only to contact the patient, but also for contacting the other professionals. Four themes were revealed: prior face-to-face contact, the telephone conversation itself, advantages, and disadvantages.
Prior face-to-face contact
The participants stressed that a prerequisite to good telephone communication was a prior face-to-face contact:
The patients with a longstanding contact, well, we can almost hear how they are on the phone by their tone of voice—but this entails that you actually have seen the patient—it is too difficult otherwise. (Interview 3)
The telephone conversation itself
The participants stated that the telephone could not be used for longer conversations or for solving complicated problems, as it was simply too demanding for the professionals to “do their job” over the phone:
A telephone consultation is really hard work, because you are frantically using all your senses…and you are actually only using your ears to listen with.…I sometimes feel quite shattered after a telephone conversation, just like after a home visit, because something quite unexpected is suddenly brought up during what was supposed to be a follow-up phone call. (Interview 1)
Furthermore, some patients do not benefit from a phone call (e.g., if there are conflicts within the family or if the patient is very anxious):
I am thinking about a patient I have at present, she is so anxious…and I had managed to connect with her, but the exchanges between her and her husband—well, it's just not on—on the phone—and I just have to sit there and wait. So the anxiety, the discord and the hard work put into the process—it can be very difficult to handle on the phone. (Interview 1)
However, the telephone was regarded as a tool for the follow-up procedure and solving minor hitches and as an essential tool for the participants.
Advantages
The obvious advantages of the telephone contact were the time saved compared with home visits and the possibility of being easily available and proactive:
The advantage of the telephone contact is that you can communicate more frequently with the patients, if they need you and they can get hold of you, if this is what they need and you can most certainly can solve any issues they may have much quicker. (Interview 2)
Furthermore, the participants recognized an advantage in telephone communication in that the professionals did not always have to “invade” the patient's home to communicate, thereby increasing the patient's privacy:
…seen from the patient's perspective, it may also be a relief. It may be a little less intrusive for them. It is also very demanding.…We must not overrule the significance of the team invading their home each time. (Interview 1)
Disadvantages
One of the disadvantages of telephone communication was that the participants missed all the nonverbal communication and could not use their “clinical eye.” This may result in the professionals missing out on the patients' deterioration or signs of treatable conditions:
And this is the disadvantage because then we don't get to see the patient…. And he has deteriorated very quickly, although we didn't sense this over the phone. He sounded as fit as a fiddle—so, it can also be very misleading. (Interview 3)
The participants also admitted that it was sometimes difficult to maintain their concentration and stay focused when talking to a patient over the phone:
I have to pull myself together when speaking on the phone…. If it is a very talkative patient, I find myself checking blood tests on the computer.…I get easily distracted. It is much easier to stay focused when you are face-to-face with the patient. (Interview 1)
Later on in the patient's trajectory, the phone calls tend to be more with relatives or professionals in the patient's home, which makes the contact with the patient difficult and sporadic:
A typical course of events starts by our initiating the contact with the patient and this proceeds very well for a while, and then the patient's condition gets worse, after which the spouse takes over. Then the community nurse comes on the scene and eventually takes over completely. So it doesn't matter what the symptom is, it has been “polluted” by two others before I get to know of it. (Interview 2)
Finally, practical procedures and objective observations were obviously not possible over the phone:
I have a lot of home visits and not really very many telephone consultations, because I can't do physiotherapy over the phone. Well, I can follow up on some things—well a few things, but otherwise…(Interview 3)
Modern Telecommunication
The participants had diverging attitudes toward “modern telecommunication.” The five themes that emerged from the interviews were prerequisites, advantages, disadvantages, barriers, and technology.
Prerequisites
One prerequisite mentioned by the participants was the familiarity between patient and professional:
It has something to do with trust—it would be completely different if I visited you. No one else can see it…(Interview 3)
Another prerequisite was the expectations to using this kind of technology (e.g., young people are more confident with technology and sending personal information and pictures via the Internet):
One day it will be a routine procedure. Everyone's using Skype these days, so I believe that it will happen sooner or later. (Interview 3)
They also stressed the importance of a reliable technique that is easy to use in general, also in collaboration with the primary care sector:
In some ways I feel that we are more peripheral than the community nurses and home carers who visit every day…. And this is where it must function first and foremost. (Interview 1)
Additionally, the camera equipment should be able to be moved around in the patient's home:
If we have a patient who says, I just can't get up…. Well, then—try to film it. That would be ingenious. (Interview 3)
The participants mentioned that using a camera (visual contact) should be offered as an option and not be a requirement:
It would always be something we could suggest, and then it is up to them to say, well, I would like to try it out. (Interview 3)
The participants predicted that it could be difficult to know when to introduce the technology in a palliative trajectory:
A patient of mine died on Friday—after 3 years. We had short intervals of very close contact. It would be wrong to have the equipment in a home where it is not being used. But how we get to know that, I don't know. (Interview 3)
Advantages
One of the major advantages that the participants could see was the add-on value compared with the conventional phone call. The participants talked about “adding a dimension more” in order to achieve nonverbal communication and get more information about the patient's physical status and the tension within the family:
Communication reaches another dimension when you can see each other. You can see and read each other's body language. You can see what is going on in the home. How much commotion is going on or how peaceful the home is. (Interview 4)
Furthermore, it would help the professionals to be more attentive and focused on the communication compared with a regular phone call, and consequently it was seen as more demanding for the professionals than conventional phone calls:
In a video consultation, you will be more prepared and have familiarized yourself with the task and you will be more concentrated on the process. If the patient says: I am very well—well, then you have already moved on to the next task and are finding the notes. You don't do that on a video because the patient will then see that you are concentrating or not. I believe that there is much more intimacy in a video consultation. (Interview 4)
This participant also added that there would be an opportunity for more than just a two-way communication and involvement of family members, but also other professionals. The participants perceived an opportunity to share information and to educate and support primary care professionals (i.e., homecare nurses and general practitioners):
Well, it could be the GP, who was there and if we had a video conference, then the GP could see the patient alongside us, the specialists, exchanging advice and instructions, and finding solutions together about what the best intervention would be, what the problem is…. So that it involves knowledge exchange as well. (Interview 2)
Disadvantages
Compared with face-to-face contacts, the informants were concerned about an increased focus on physical problems:
I am worried that the focus will be on physiological problems…instead of the intimacy, which is alpha and omega in this situation—and something that video cameras cannot replace. (Interview 4)
The higher cost-effectiveness of telecommunication compared with face-to-face contact was also a concern as it may encourage SPC professionals to skip face-to-face contacts and use telecommunication instead.
Barriers
We found several barriers toward using telecommunication. First of all, the participants were very concerned about the ethical issues in the use of telecommunication, especially when the patient's death is imminent:
This is also a question of ethics. How long should the camera be kept operative at the bedside? Should it be during the final days, or even when the patient is anxious about the situation, or do we close down there? (Interview 2)
Some participants also had concerns about whether the elderly patients would be able to use the new technology. However, they did not agree on this issue:
There are some elderly people, who simply cannot handle the technology. Some have absolutely no idea about it and can hardly turn on their TV. (Interview 4)
But there are some 90-year-olds who are on line and very much more in tune than you can imagine. (Interview 1)
The interviews also revealed barriers against the technology within the professional group, regarding video technology as an intrusion of the professionals' privacy:
It is somewhat undefinable…for me, being visual would be too private. The fact that other people would be able to see it, etc. (Interview 3)
It also has something to do with being seen with morning hair, or what about the people who usually use make up? How would you feel about others seeing you like that? (Interview 3)
Technology: talking about “modern telecommunication.”
Opinions concerning other telemedicine devices also came up, and opinions were more varied on this subject. A few participants could see the advantages of teletransmission of blood pressure and oxygen saturation data, whereas most informants could not see the need for this option in a palliative care setting and were concerned about the negative effect it may have on the contact with the patient. Both nurses and doctors were of these opinions:
My worry is that there will be more focus on physiological things—there is a danger of this. (Interview 4)
Opinions were more positive when discussing the possibility of screening and symptom scoring:
Apparently, you can get electronic cards and you can ask the patient to tick off how much pain he/she is in today and the result appears on the screen. (Interview 4)
However, in general, permanent monitoring at home was not something the participants considered as a positive thing:
And this is not how we monitor the patients….at that stage of life, they are on their way out of the monitoring stage and into something else. So perhaps this would mean holding on to something untimely by starting to monitor them too much. (Interview 1)
Discussion
Main Findings
We found that the SPC professionals perceived many advantages in telecommunication with a camera device, but mainly as a substitute or supplement to conventional telephone communication. They could not imagine that telecommunication could replace face-to-face communication because they found the physical encounter essential for establishing the necessary relationship with the patients, underlining that good communication is indispensible for high-quality palliative care.
There were also ethical and practical concerns in relation to telecommunication. When it came to teletransmission of measurements or the permanent monitoring of the patient in the patient's home, almost all the participants expressed strong reservations.
Strengths and Weakness
Interview studies are an appropriate method for exploring the informants' perspectives and experiences concerning a specific topic. The advantage of group interviews is the interaction within the group that can facilitate the emergence of new themes, and the group discussion can deepen the understanding as a more detailed reflection is facilitated by this method. 23 Furthermore, the health services and the delivery of palliative care vary considerably between different countries.
Considering the barriers for implementing telecommunication in palliative care in our study, one has to take the inexperience and limited knowledge about application of telemedicine into consideration since a priori knowledge and experience may modulate those perceptions. Furthermore, we only interviewed doctors, nurses, and physiotherapists, and there are indications that modern technology may be more readily accepted by, for example, nursing and administrative staff, whereas those employees who address primarily psychosocial issues may be more reluctant toward such technology. 24
However, the findings of this study seem relevant to the well-developed healthcare services in the majority of countries and a division in specialized and basic palliative healthcare levels because most countries have a low level of telemedicine implementation, especially in palliative care. With respect to generalizability of the study, the low-inference analytic approach “qualitative description” reduces the possibility of generalization.
Comparison with Existing Literature
Most published articles concerning telemedicine have in general focused on diagnostic accuracy, patient satisfaction, and technological evaluation. Clinical feasibility, effectiveness, and cost-effectiveness have received limited attention. 25 Hence, few studies have explored the views of SPC professionals on telecommunication before the implementation of the new technology, despite previous studies showing that provider participation in the design of telehealthcare systems was necessary for a successful implementation. 26 –28 In general, professionals seem to have a positive attitude toward the use of “modern telecommunication.” 14,16,29 “Modern telecommunication” has been described as a possibility of reassurance for patients and relatives because skilled professionals can be “present” despite long distances. 30 However, in line with our findings most studies reported that a primary concern was that the technology might be used as a substitute for traditional face-to-face interaction by substituting telecommunication with actual visits, yielding a major concern of a lesser quality in communication as a result. Johnston et al. 15 interviewed SPC professionals in Scotland and stressed that telehealth initiatives should be offered as a supplement to the existing practice and accessed based on personal choice rather than being offered as a standard care approach.
Oliver and Demiris 10 looked into hospice staff's readiness for implementation of telemedicine technology and found variations in the perceived usefulness of videophones for hospice care. They concluded that the introduction of this equipment would require substantial user involvement.
Perspectives
This study shows that despite healthcare providers seeing the potential benefit of novel communication technology, they also have strong reservations. The professionals see advantages in the technology, as it can replace and optimize conventional telephony and represents quality improvement. However, they are more reluctant when it comes to replacing face-to-face contact with communication technology. The professionals fear that the new technology will hamper the contact and reduce quality of communication, which is essential in delivering high-quality care. This creates a dilemma because if the new technology is to move resources from transport costs and the time spent with the patient, it must be able to replace some of the face-to-face contacts. Two studies have concluded that many home visits in palliative trajectories, both in SPC and in primary care, were considered appropriate for video contacts, which further brings matters to a head. 31,32 It is crucial for future technology initiatives in palliative care that the huge significance of the quality of communication between patient and professional is taken into account. The success of future telemedicine programs in palliative care will be strongly related to the professionals' involvement in the development and the implementation to enhance the quality of the communication with the patients and their families, and not just a technical device to reduce costs. 33
Conclusions
Our study underlines that face-to-face contacts are necessary for optimal palliative care and that home visits are preferred. The participants were generally positive toward telecommunication, although several reservations and prerequisites were voiced.
If “modern telecommunication” is to be implemented in palliative care, it is necessary to initiate a process where the professionals are involved in the development and implementation of the technology and where the form and use of the technology is individualized, in relation to both the patients and the setting, where also cultural and legal differences may exist.
Footnotes
Acknowledgments
Profound gratitude is extended to the participating informants from The Palliative Teams in Herning, Randers, and Aarhus, Denmark. Furthermore, we thank The Palliative Team at Aarhus University Hospital and The Research Unit for General Practice at Aarhus University for providing employment with time and practical help to conduct the study.
Disclosure Statement
No competing financial interests exist.