
Abstract
Introduction
Despite evidence that adherence to treatment recommendations can lead to blood pressure control, 1 hospitalization prevention, 2 and decreased mortality rates 3 , many patients do not adhere to antihypertensive medications, 2 dietary advice, 4 and physical activity recommendations. 5 Behavioral interventions have been shown to effectively increase adherence and improve blood pressure control in hypertensive patients. 6 –8 In-person counseling to improve adherence can be time-consuming, labor-intensive, and expensive, however. 9
Telephone counseling is a cost-effective method of delivering behavioral interventions to improve adherence. 10 Telephone-delivered interventions can be particularly cost-effective for providing healthcare to patients with complex chronic medical conditions. 11 Patients report that they are satisfied with telephone counseling 11 and that it is more convenient than in-person counseling. 12 Telephone counseling has been used to increase medication adherence, 13,14 promote exercise, 15 improve adherence to dietary advice, 16 and lower blood pressure levels. 13,17 It has been successfully used in Veterans with a variety of complex conditions requiring multiple behavior changes, including hypertension, 18 diabetes, 19 chronic heart failure, 20 and stroke. 21
However, little is known about the characteristics of patients who are best reached by telephone counseling or who benefits the most. Breast cancer patients receiving telephone-delivered counseling improve most if they are in long-term marriages and have no history of depression. 22 Telephone counseling as an adjunct to smoking cessation methods is most effective in patients who are younger, male, and light smokers. 23
To our knowledge, no study has examined the characteristics of hypertensive patients who are most easily reached by telephone-delivered counseling interventions. Hypertension is highly prevalent, affecting approximately 77.9 million Americans. Prevalence rates vary for different ethnic groups: 33.4% for white men, 30.7% for white women, 42.6% for black men, 47.0% for black women, 30.1% for Mexican American men, and 28.8% for Mexican American women. 24 Rates in Hispanic Americans are equivalent or lower than those in white Americans. 24,25 Age and gender also play an interactive role: hypertension is more prevalent in men than women until 45 years of age. Between 45 and 55 years of age, prevalence is about equal in men and women, and then after 55 years of age, it is more common in women than men. 24 Only about half of those with hypertension have it under control. 24,26 Hypertension control requires modification of multiple behaviors, including diet, medication-taking, and exercise. Telephone-delivered interventions for patients with hypertension and other chronic diseases have great promise, but it would help if we could identify patients who would benefit most from such an intervention. The purpose of this study was to describe the baseline characteristics of patients that are predictive of being easily reached for a 6-month, telephone-delivered behavioral intervention to improve treatment adherence among Veterans with uncontrolled hypertension.
Materials and Methods
Participants
Data were collected from patients with hypertension participating in a randomized controlled trial of a telephone-delivered behavioral intervention to improve treatment adherence. Additional details of the study are available elsewhere. 27 Institutional Review Board approval was obtained prior to study initiation. Participants were recruited and screened by a research assistant while at the primary care clinics of two large Veterans Affairs Medical Centers for a routine clinic visit. They were enrolled if they had uncontrolled hypertension as defined by the Joint National Committee's seventh report 28 and were prescribed at least one antihypertensive agent for at least 6 months. Participants also had to be at least 21 years old, have a working telephone (landline or cell), be free of severe comorbid conditions, and plan to remain in the area for the next year.
Procedures
At the time of enrollment, demographic data and telephone numbers were collected from participants via self-report. Participants were encouraged to provide as many telephone numbers as possible (e.g., home, work, cell phone) as well as the one or two best times when they could be reached. They also provided one to two alternate contact numbers for family and friends who could be contacted if staff were unable to reach them for 1 week.
During the period between enrollment and baseline, the research assistant placed a phone call to the patient to confirm the visit, remind participants about study obligations, and simulate the experience of telephone counseling sessions by providing patients with brief information based on an American Heart Association pamphlet on hypertension. This call also verified that the participant had a working telephone. Approximately 1 month after enrollment, participants returned for an in-person baseline visit where outcome measures were obtained by the research assistant. Participants received $20 at the end of the visit to reimburse for their time and travel. Although coming for an in-person visit could be a barrier for participation, the research assistant tried to schedule the visit at a time that was convenient for the participant and often scheduled the visits on the same day of another medical appointment. Because participants were Veterans with comorbid medical conditions receiving care at a Veterans Affairs Medical Center, they often received all of their care there and had frequent appointments.
Intervention Arms and Procedure
Postbaseline, all patients whose telephone numbers had been verified were randomized 1:1:1 to receive a telephone-delivered stage-of-change-matched intervention, a telephone-delivered health education intervention, or usual care. Participants randomized to stage-of-change-matched intervention received six monthly tailored sessions, focusing on diet, exercise, and medication recommendations for hypertension based on the transtheoretical model. 29 Counselors used a computerized manual to assess stage of change for each of the behaviors of interest and tailor counseling to participants' current stage of change using the processes of change found to be most useful for each stage of change. 22,23 Counseling also incorporated decisional balance and self-efficacy. Stage-of-change-matched intervention calls were approximately 30 min each month. Participants in the health education intervention received monthly telephone sessions for 6 months consisting of standardized, nontailored information about diet, exercise, and medication recommendations for hypertension. In order to equalize for attention, participants were also encouraged to ask questions and provided information about a different health topic (e.g., sun safety, influenza prevention) each month. Health education intervention calls lasted approximately 15 min. Usual care participants received no counseling.
We included all participants who were randomized to one of the two telephone intervention groups and should have completed the 6-month phone call period as of March 21, 2008 (n=124). We did not examine the data by treatment arm because this was an ongoing, blinded randomized controlled trial.
All counseling sessions were conducted by trained psychologists and social workers (all female) who were not involved in recruitment or assessment. Patients were randomized equally to counselors. Each counselor had an equivalent patient load. Counselors utilized the information about best days and times when the participant could be reached for the first call, which occurred approximately 7 days after the baseline visit. If a participant was reached to complete the monthly session, an appointment was set up at the end of the call for next month's session. Participants were called on weekdays between 8 a.m. and 5 p.m. unless a participant requested a different time (e.g., after 5 p.m.).
Call attempts for the first call were made at the times provided during enrollment and, for subsequent calls, at the times provided during the prior month's phone call. If participants were not reached at that time, counselors attempted to call them at other times of the day with a maximum of two attempts per day. Participants were called for up to a 2-week period following the date of the call appointment scheduled during the previous month's call (or, for the first call, beginning 7 days after randomization). Thus, counselors attempted to reach participants for up to 2 weeks each month. If they were unable to reach a participant after 7 days, counselors began contacting the alternate contact(s). If they were still unable to reach the participant after 10 days, the counselor sent a letter to the participant requesting that he or she call the counselor to set up an appointment. After 2 weeks had elapsed and the participant was not reached, no further call attempts were made for that month, and the session was counted as missed. The counselors called participants again for their next monthly phone call approximately 1 month later. If a participant's telephone number became disconnected, alternate contacts were called, and letters were sent.
Each call attempt made to each participant was logged for the date and time, and the resolution of the call was recorded by the counselors. This contact log was the primary source of data used to determine the number of attempts per completed call and the total number of calls received during the intervention period.
Data Analysis
Percentages and means were used to describe demographic characteristics, which were the independent variables. The dependent variable was the number of call attempts per calls completed for each patient, with a lower value indicating that a participant required fewer phone attempts in order to complete the monthly sessions. In order to have the most general model for the number of call attempts per completed call, we fit a negative binomial model, which allows for the variance to be larger than that of a Poisson model for the number of counts. In the negative binomial regression model, the mean number of call attempts was modeled as a log-linear function of demographic characteristics. Generalized estimating equations 30 were used to account for the repeated measures on the same patient (i.e., the number of call attempts in each of the 6 months). Because we were not interested in the correlation of these measures over time, we fit the model under independence, which gives correct estimates, and used a robust standard error that accounts for the clustering of the repeated measures on the same patient.
The regression parameter estimates from the negative binomial regression model were then used to calculate the mean number of call attempts per calls completed, as well as the relative increase in attempts per call when comparing demographic subgroups, using the regression parameter estimates and standard errors, with 95% confidence intervals also being calculated. All tests were two-sided. Data were analyzed using SAS version 9.2 software (SAS Institute, Cary, NC).
Results
Demographic characteristics of the study sample are shown in Table 1. Participants were mainly male because we recruited from Veterans Affairs Medical Centers. Participants completed an average of 5.71 out of a possible 6 sessions (range, 3–6; SD 0.67). Most participants (79.8%) completed all six calls, whereas 14.5% missed one, 2.4% missed two, and 3.2% missed three calls.
SD, standard deviation.
Figure 1 shows the mean number of call attempts per completed call by demographics. Hispanic participants had the lowest mean number of call attempts per completed counseling session relative to participants from other racial/ethnic backgrounds. Retired participants had the lowest mean number of call attempts per completed counseling session relative to employed and unemployed participants. Participants with a college degree had the lowest mean number of call attempts per completed counseling session, whereas participants with a high school education level had the highest. Married participants had a lower mean number of call attempts per completed counseling session than unmarried participants.
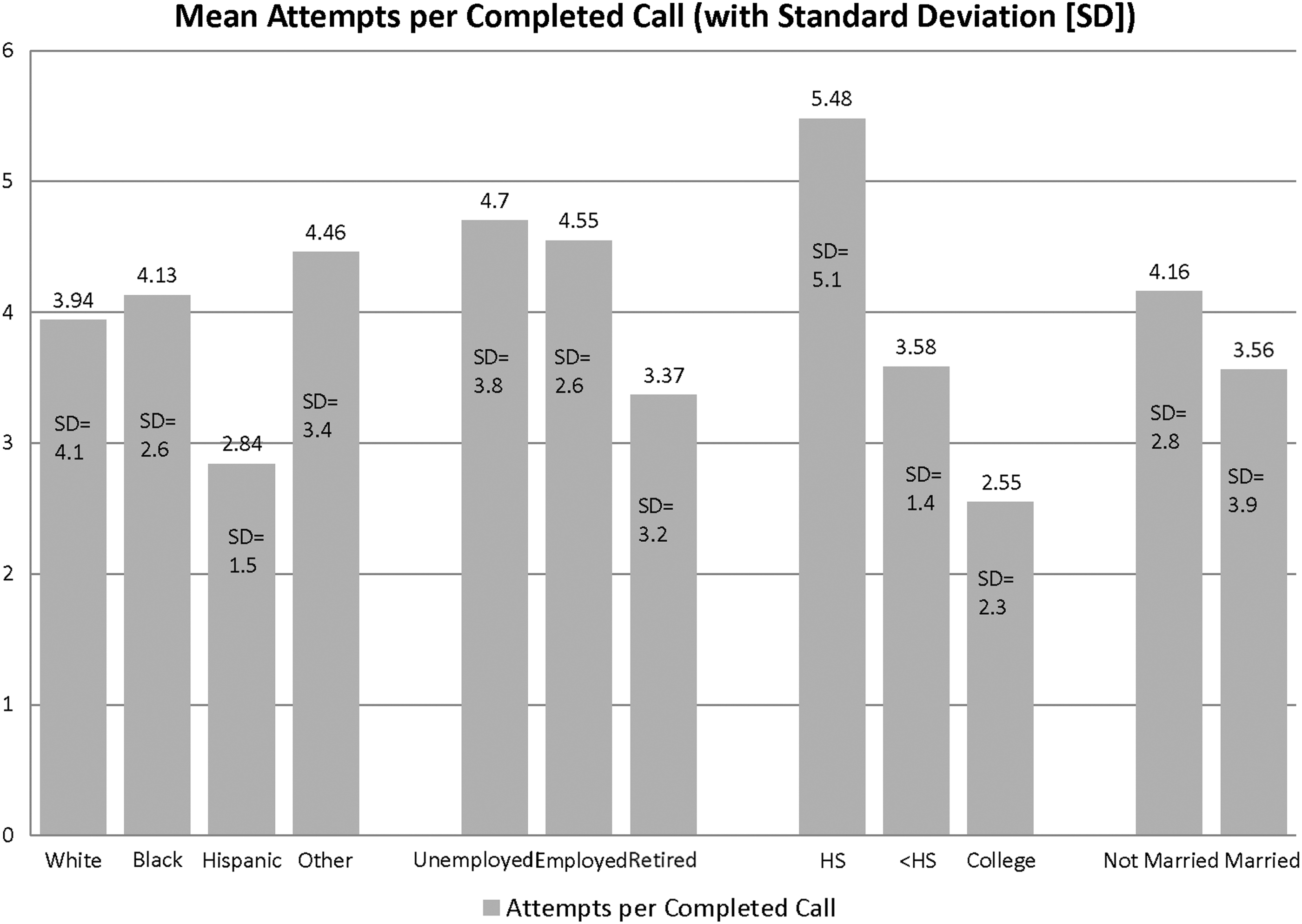
Mean (with standard deviation [SD]) attempts per completed call. HS, high school.
Results from the negative binomial regressions are presented in Figure 2, where only significant results are displayed. No pairwise interactions were found to be significant. Unmarried participants required 1.22 more call attempts per completed call than married participants (95% confidence interval [CI] 1.05, 1.42). Marital status remained significant after controlling whether the participant lived alone or with someone (rate ratio=1.28; 95% CI 1.08, 1.52). African American participants required 1.43 more call attempts per completed call than Hispanic participants (95% CI 1.14, 1.80). There was no significant difference between the number of call attempts required to reach white participants and African American participants (rate ratio=1.13; 95% CI 0.95, 1.34). Unemployed participants required 1.37 more call attempts per completed call than retired participants (95% CI 1.13, 1.67). Employed and retired participants did not differ in call attempts per completed call (rate ratio=1.42; 95% CI 1.18, 1.69). Participants with less than a high school education required 0.74 fewer attempts per completed session than participants with a college degree (95% CI 0.60, 0.91), whereas participants with a high school education required 1.40 more attempts per completed session than those with a college degree (95% CI 1.17, 1.67). There was no difference in attempts per completed session between participants who lived alone and those who lived with someone else (rate ratio=1.00; 95% CI 0.86, 1.16). Age was negatively associated with call attempts per completed session (r=–0.23; p<0.01).
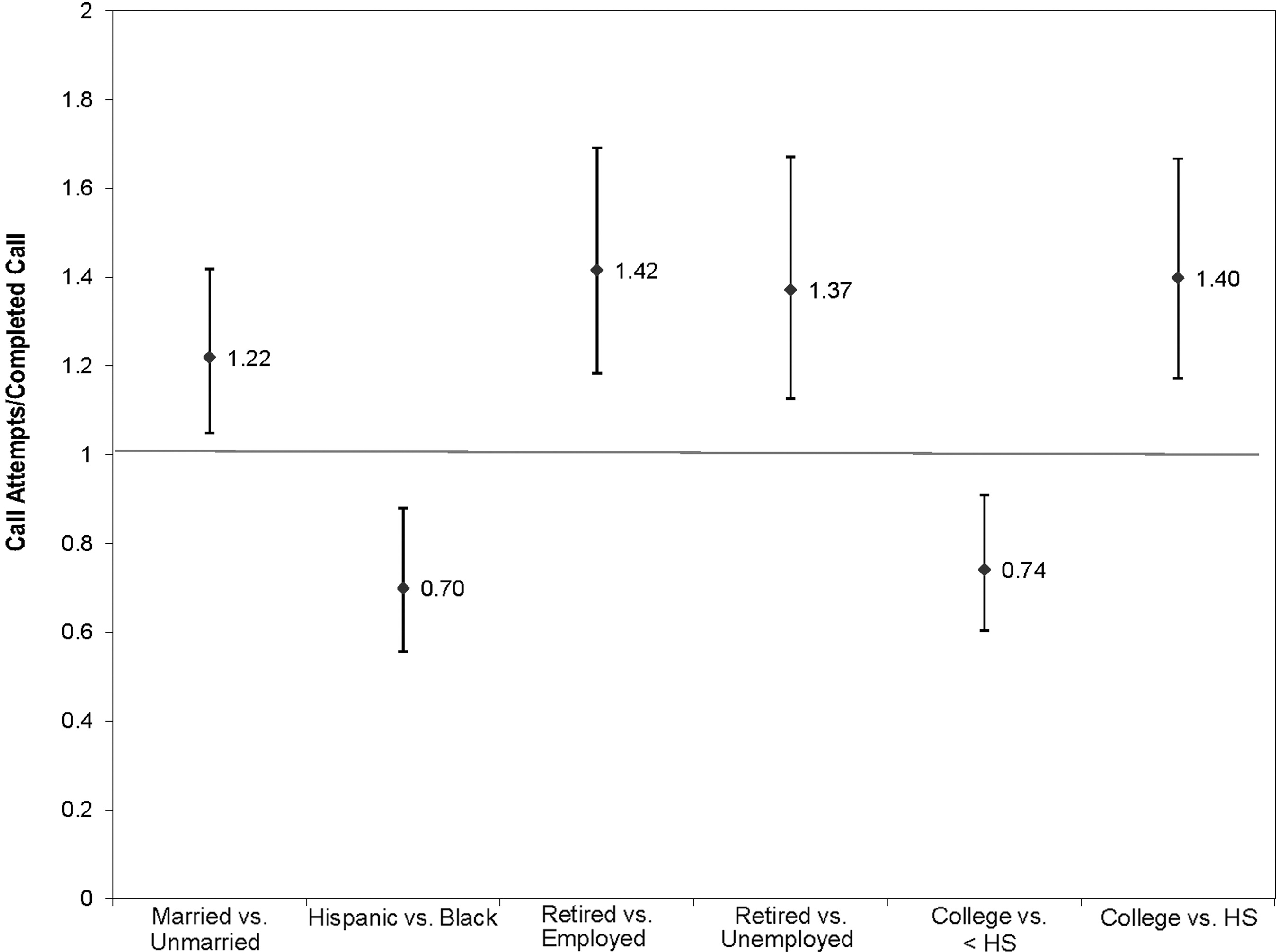
Significant results in the negative binomial regressions for call attempts/completed calls. HS, high school.
Discussion
Overall, we found telephone-delivered counseling to be a viable method of reaching hypertensive patients for a behavioral intervention to improve adherence to treatment recommendations. Nearly 80% of our participants received all six intervention phone calls, with participants completing an average of 5.71 sessions. This is consistent with prior research reporting that telephone-delivered counseling is acceptable and convenient for patients. 11,12
Our results suggest that telephone-delivered counseling may be easier to conduct among certain demographic groups. Participants who were married required fewer call attempts than those who were not married. This finding is consistent with prior research. 31 It is interesting that, even when including living status in the model, married participants continued to be significantly easier to reach than unmarried participants, suggesting that the mere presence of family members, friends, or other roommates is not sufficient to make a person more easily reached via telephone counseling. The presence of a supportive spouse may facilitate treatment via telephone.
We also found that Hispanic/Latino participants were more easily reached than participants from other ethnic backgrounds. Previous research suggests that Hispanics/Latinos may have more family social support than individuals from other backgrounds, and this may translate into better physical health. 32 Moreover, children and extended family members may have fulfilled some of the functions for our Hispanic/Latino participants that spouses fulfilled in participants from other backgrounds, such as encouraging individuals to keep medical appointments and passing along messages from counselors. This is a particularly interesting finding given the body of research suggesting that Hispanics/Latinos typically underutilize mental health services. 33 Our results suggest that telehealth may be a promising method for the delivery of behavioral interventions to Hispanic Americans.
Employment status also played a role in reaching participants, with retired participants being easiest to reach. It seems logical that employed participants would be more difficult to reach than retired participants, as retired individuals would be home more than employed people, and even if employed participants provided us with their work numbers, they may have more work-related time constraints. Unemployed participants may have a less regular schedule than retired participants because they may be seeking a job. Additionally, participants may be unemployed because of mental health, physical health, or personality factors that would make them more difficult to reach for telephone counseling.
Participants with a college degree required fewer attempts than those with a high school or less than high school education. This is consistent with findings that socioeconomic status is negatively associated with mental healthcare utilization. 34 However, we unexpectedly found that participants with less than a high school education were easier to reach than those with a high school degree. This may be a function of participants' type of employment; perhaps individuals with a high school education have a less flexible type of job or job schedule than those with less than a high school education.
Certain potential limitations are worth noting. First, our results may be limited by self-selection. Because the telephone counseling is provided as part of a research study testing its effectiveness, only participants who were interested in participating in the study received counseling. Individuals who elect to participate in a research study may be different than those who elect not to participate, and therefore it is unclear how well our findings would generalize to a telephone counseling program implemented in a medical facility. Furthermore, the inclusion of a run-in period may have resulted in the screening out of participants with certain characteristics, in particular screening out individuals with lower levels of education, 35,36 although analyses of our own run-in period do not suggest that this is the case. 27 One of the primary purposes of our run-in period was to filter out participants who did not have a working telephone number; participants who were not reached by phone at least once to verify the existence of a working number were not randomized. This procedure may have resulted in the exclusion of individuals who were particularly hard to reach by phone. However, patients who are not willing or able to be contacted by phone may not be good candidates for telephone counseling, so our sample is likely to be representative of those who are willing to receive such an intervention.
Second, our study was done in two Veteran outpatient clinics, and thus our sample comprised all Veterans, most of whom were older males, raising the concern about how well our findings generalize to other patient groups. However, hypertensive patients are likely to be older, suggesting that our findings may be generalizable to other hypertensive patients. More research should be conducted to determine which patients in other healthcare settings or with other medical conditions are difficult to reach for telephone counseling. Finally, our sample size is small, so the conclusions we are able to make from these findings are limited.
Our results suggest that telephone counselors may need to devote more time and resources to reach individuals with other sociodemographic characteristics. Possible ways of improving our ability to reach such patients include placing reminder phone calls in the days prior to a scheduled appointment and sending handwritten 37 reminder letters to confirm the appointment made during the previous session. Because our study is a blinded randomized controlled trial, the telephone counselors do not participate in outcome assessment. Participants meet with a separate research assistant for all study visits and never meet the telephone counselor in person. In addition, it may be easier to reach certain patients if they have an in-person meeting with their counselor at the beginning of the study to build rapport and personal commitment.
Conclusions
Telephone-delivered counseling is a viable method of delivering behavioral interventions to improve adherence to treatment recommendations. Our findings suggest that individuals who are of Hispanic/Latino descent, married, or retired or have a college degree are easier to reach than those with other characteristics and accordingly may be more likely to benefit from such telephone-delivered counseling.
Footnotes
Acknowledgment
This material is based upon work supported by the U.S. Department of Veterans Affairs, Veterans Health Administration, Office of Research and Development, Health Services Research and Development (IIR 04-0170 and CDA 08-009).
Disclosure Statement
No competing financial interests exist.