
Abstract
Introduction
Medical screening is a strategy used in a population to identify an unrecognized disease in individuals in apparently good health, with presymptomatic or unrecognized symptomatic disease. 1 Rare implementations of screening methods in telehealth have been described in ear-nose-throat 2 and ophthalmology. 3,4 Telemedicine-based screening has already been implemented in orthopedics, but its effectiveness was not evaluated. 5 Postural school screening remains a powerful tool that can be used to identify children with scoliosis or sagittal plane deformities. 6 –16 Scoliosis school screening is mandated in several countries. 14
Evidence-based medicine methods require validity, reliability, and quantitativity. There have been several attempts to introduce evidence-based medicine to posture evaluation. The majority of those methods evolved from surface topography, 10,11,15 –19 among which the Moiré method has been the most widely used. Surface topography has a potential to become a gold standard in this field, although in clinically confirmed cases the radiography-based Cobb angles remain still the most common verification measure. Analysis of the results produced by topographic methods has recently become better codified, and several indices have been developed. 16,20,21
Modern three-dimensional (3D) surface imaging methods for scoliosis and posture screening are worth being implemented on a large scale. 5 Reliability, accuracy, and the remaining 3D image for each subject are strong arguments for further use, particularly in cases with detected deformities. 21 –27
The aim of this study was to assess the time effectiveness of the implemented telediagnostic screening procedure and compare it with results for classical examinations present in the literature. The evaluation considered only the assessment part, which can be performed remotely, which makes it possible to limit the participation of a physician or physiotherapist to the final part of the examination.
The developed system operates in “store-and-forward,” as opposed to “real-time,” telemedical systems. Medical data are gathered on-site and can be later accessed remotely by specialists. The main advantage of the implemented procedure is connecting accurate and meaningful medical documentation with the possibility to access and analyze it from an arbitrary location.
The system offers a new approach compared with existing classical examination methods. 15,28,29 3D images produced by the system can be accessed over the Internet in a comparable time to ordinary photographs, which makes it superior to classical documentation methods by supplying more insight into a patient's medical data with similar access cost.
This article does not aim to compare different surface topography systems. A new metrologically accurate system was developed to achieve objectiveness in documentation and analysis. In principle, the presented screening methodology will be valid for any surface topography system that delivers results as point clouds.
The measurement system analyzed and data used in this study are part of the project “Telemedical Automatized System for Three-Directional Measurement, Analysis, Detection and Monitoring of Posture and Body Deformations,” carried out during the years 2008–2012. During the project, in total, 10,000 patients were examined, and over 20,000 measurements were analyzed.
Materials and Methods
Sample Group
The subset from already acquired measurements was randomly selected from the database—100 subjects of both sexes from randomly chosen schools. The study protocol was approved by the institutional Bioethical Committee according to the Declaration of Helsinki. The group analyzed in this study was examined at school. Underaged subjects' parents or legal guardians and adult subjects signed their informed consent forms to participate in the study.
Measurement System and Evaluation Method
By current standards, classical screening examination consists of evaluation of postural deviations ad oculos or with simple measurements. The simple Adam's forward bending test and low-cost scoliometer measurement of the angle of trunk rotation (ATR) remain the most frequent tests. 14,16,30,31 The physical exam assessing the forward bending test and ATR with a scoliometer usually involves palpation of the subject's body. Asymmetries of shoulders, waist, and pelvis are evaluated by observation with or without a grid. Faulty postures as well as scoliotic deformities can be detected. Measured kyphosis and lordosis surface angles and sagittal trunk inclination may show additional variety of deformities. This study was performed using a newly developed back surface topography measurement system for posture and scoliosis screening (hardware and 3D Orthoscreen™ software; Medical University of Warsaw, Wojciech Glinkowski, Jakub Michónski), a product built in-house by the project funded by the National Center for Research and Development.
The system used in this study consists of three modules: 3D measurement system, centralized database, and data analysis software on the client side. 32,33 The 3D measurement module is an optical full-field 3D scanner based on the structured light illumination method. 34 –36 During the measurement process the subject stands still inside a calibrated measurement volume while a series of images is projected onto his or her body surface. The shape of the back of the trunk surface is calculated based on the deformation of the raster. 37 The dataset produced by the measurement system 38 is a set of points in 3D space (cloud of points) that exactly represent the surface of each subject's body (dimensions and angles are preserved). The result of the measurement is correctly oriented in space thanks to calibration of the plumb line. Measurement accuracy is between 0.2 mm and 0.4 mm, depending on specific implementation of the system. Acquisition takes roughly 4 s. A sample measurement is presented in Figure 1.
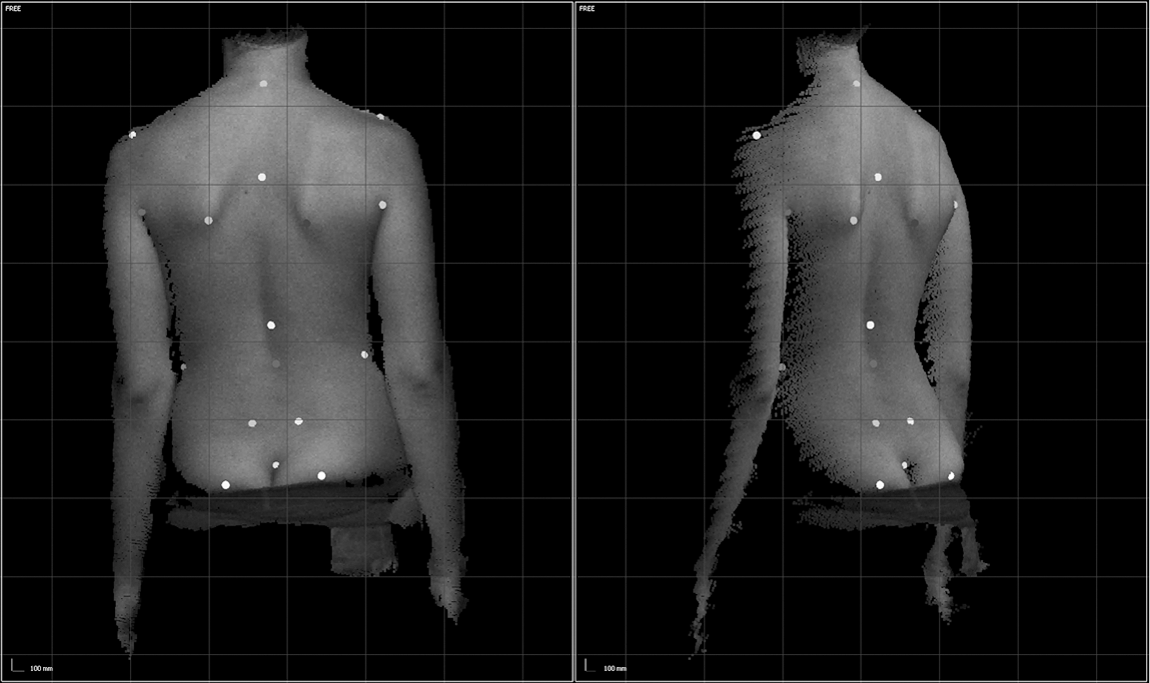
A sample cloud of points for a subject with manually marked anatomical landmarks, seen from the
Measurement data along with corresponding patient information are stored in a centralized database and can be remotely accessed using customized data analysis software. A user account system provides authentication and authorization of the users. The software is used to mark manually required anatomical landmarks on the back surface: • vertebral prominence of spinous process C7 • natal cleft • left and right acromion • left and right apex of axilla • most proximal waist points on both sides • posterior superior iliac spines (left and right) • inferior angles of scapula (left and right)
Based on the positions of landmarks, well-known and commonly used parameters for back surface evaluation are evaluated, including the Posterior Trunk Symmetry Index (POTSI), 39 –41 Deformity in the Axial Plane Index (DAPI), 20,39,40 and Surface Angle of Trunk Rotation, 11,16,42,43 recommended by the Society on Scoliosis Orthopaedic and Rehabilitation Treatment, 14,20,44 along with surface kyphosis and lordosis angles and asymmetries of shoulders, waist, and posterior superior iliac spine.
Examination Procedure
Before the examination, the system operator enters the patient's required personal data (age, date of birth, sex, etc.) into the database. Then, the examination is performed. The subject is asked to expose shoulders, neck, waist, and sacral region below the natal cleft for a complete 3D image of the back and to stand still in the habitual posture for a few seconds. During markerless surface topography no palpation examination is necessary.
The measurement data were archived in the database, from where they could be later remotely accessed by a physician or physiotherapist. After manual marking of the predetermined anatomical landmarks, the measurement is automatically evaluated, and a report is generated. The results are saved in the database for future use.
POSTURE EVALUATION PROCEDURE
The remote assessment was performed on the cloud of points acquired from the subject during the exam. Analysis of the measurements consisted of the following steps: • cloud of points retrieval (extraction of data from the database and transmission to the local computer) • marking predetermined anatomical structures (operator interaction with 3D data) • saving and upload of the result to the server • report generation (contains images and measured indices)
The report was generated automatically and contained patients' personal data, values of indices calculated based on the 3D image, and several traditional images generated from the point cloud for visualization of different features and parameters included in the report (Fig. 2).
In this study the duration of each step of therapist/physician-assisted evaluation of the subject's posture recorded on the 3D image was measured independently with a stopwatch.

Sample report generated for a scoliotic patient. DAPI, Deformity in the Axial Plane Index; POTSI, Posterior Trunk Symmetry Index; PSIS, posterior superior iliac spine; sATR, Surface Angle of Trunk Rotation; SHS, Suzuki's Hump Sum.
Client-Side Configuration
Two configurations with different PC computers and Internet connections were used to test the analysis procedure (Table 1).
Configurations Used for Remote Postural Assessments
Statistics
Statistical analyses were performed with STATISTICA data analysis software (version 10;
Results
Sample Group
Clouds of points belonging to 100 subjects have been retrieved randomly from the database of over 20,000 records without the use of any special selection criterion. The selected results belonged to subjects of both sexes from 12 to 62 years of age (average, 18.56 years; standard deviation, 1.6 years). The group of teenagers examined in this study consisted of 39 girls ranging in age from 13 to 16 years (average, 14.36 years; standard deviation, 0.89 years) and 49 boys in the same age range (average, 14.54 years; standard deviation, 0.89 years). In this random selection 12 sets belonged to adults, teachers who were present at school at the day of image acquisition and wanted to be reassured about the examination safety and results. All these adults were women from 30 to 62 years of age (average, 48.67 years; standard deviation, 9.74 years).
Deformity Assessment
Significant differences among groups (boys, girls, and teachers) were not found for surface topographic parameters relative to scoliosis (POTSI, DAPI, and ATR indices) in one-way analysis of variance. However, surface topographic kyphosis and lordosis angles were significantly different between adolescents and adults. The average surface topographic kyphosis angle was 30.6° for adolescents and 4.25° for adults (significance level p<0.001); the average surface topographic lordosis angle was 10.82° versus 18.05°, respectively (p=0.007). In accordance with the literature, cutoff values for referring patients for orthopedic consultation were set at 7° for thoracic ATR, 27.9% for POTSI, and 3.9% for DAPI. 20,40,41 In the study group, postures showing lateral trunk deviation (scoliotic posture) requiring referral for orthopedic examination were detected in eight girls, five boys, and three teachers, confirming a cosmetic deformity of scoliosis. Detailed average results for the study groups are presented in Table 2.
Selected Surface Topography Examination Results for the Study Group
DAPI, Deformity in the Axial Plane Index; POTSI, Posterior Trunk Symmetry Index; PSIS, posterior superior iliac spine; SATR, Surface Angle of Trunk Rotation; SD, standard deviation.
Efficiency Evaluation
The time effectiveness of the procedure was evaluated using two configurations on the client-side (Table 3).
Results of Duration of Procedures Required for Subjects' Postural Evaluation for Two Hardware and Internet Connection Configurations
SD, standard deviation.
The examination of all subjects consumed 3 h 18 min 59 s using the PC and Internet connection in the first configuration and 2 h 55 min 55 s using the second configuration. Average examination time per subject was 4 min 51 s for the first configuration and 2 min 43 s for the second configuration. Distribution of retrieval, report generation, and overall assessment time was found to be normal. The time of point cloud retrieval showed no significant differences regardless of configuration. Component times for testing locations (clinic and remote) are shown in Table 2. The differences between anatomical landmarking time and saving data time performed at the clinic and remotely were statistically significant (p<0.001 by Wilcoxon test). It should be noted that average time for both places was shorter than 1 min. The differences in the report generation and overall assessment time performed at the clinic and remotely were statistically significant (p<0.001 by t test) owing to the PC configuration.
Comparison of average examination time between the two test procedures (Table 3) shows an almost two times smaller result for the remote site. Figure 3 shows that the main input to the total time is introduced by landmarking and report generation; components that depend on the operator and remote machine configuration, however, are not influenced by network transport. The time involved in data retrieval and saving results is negligible when compared with other components. This leads to the conclusion that remote assessment is almost as efficient as evaluation performed locally. Moreover, the type of network connection used has very little influence on process duration.
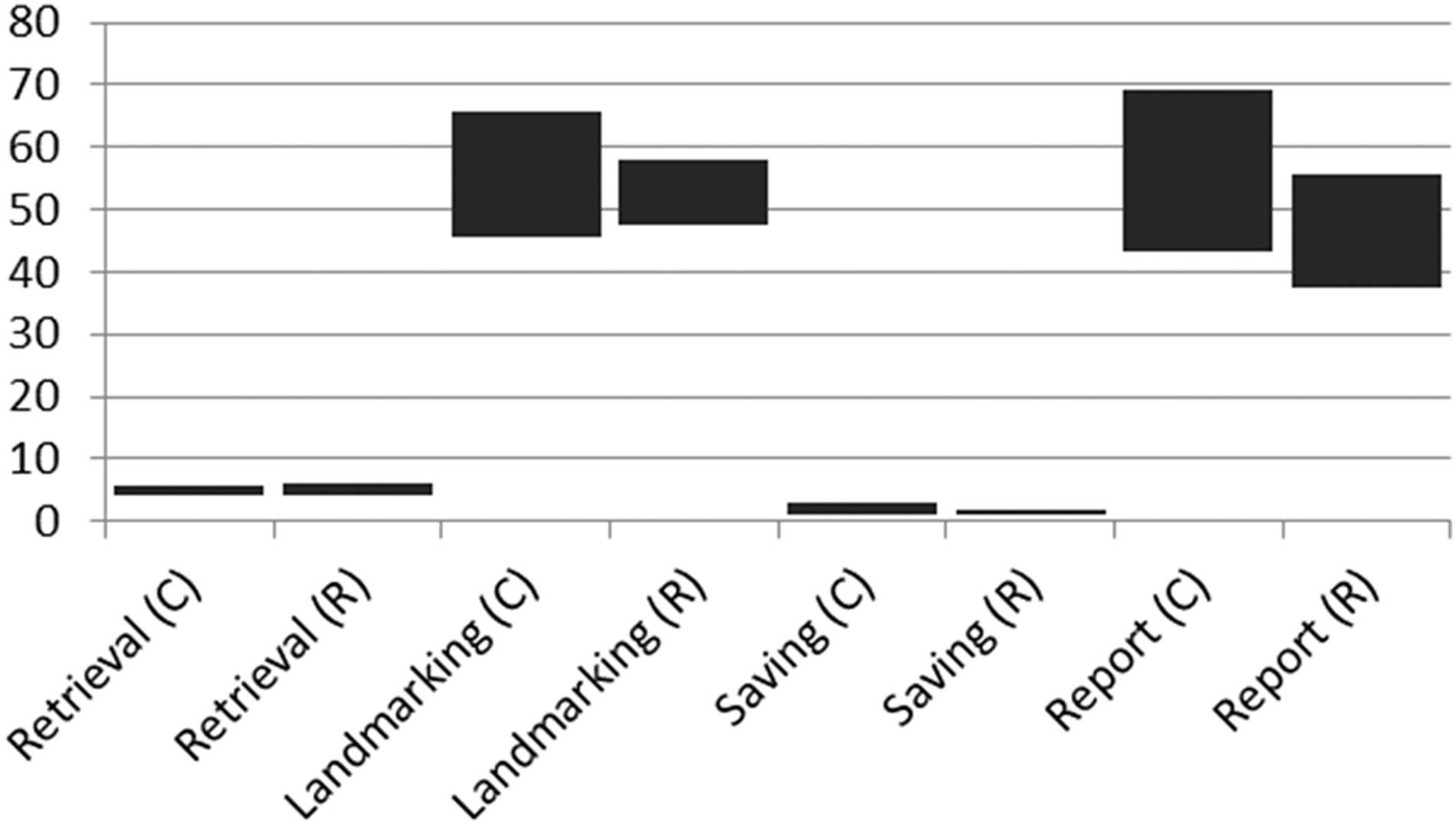
Component times (in s) for clinic (C) and remote (R) tests. Each column represents the average value±1 standard deviation.
Discussion
Although similar, the implemented examination method introduces new aspects with respect to the traditional procedure. The standard procedure requires a highly trained professional to be present during the whole examination, whereas an operator with basic training is able to acquire 3D data for clinical analysis. A physician or skilled physiotherapist is still required to perform the final analysis and produce the report; however, the time of his or her engagement is much shorter.
Lee et al.
45
listed the following screening items that generate the overall costs of school screening: • screening by a medical professional (skilled nurse or physician) without reporting time—3 min per session/subject • screening of ATR and clinical signs—5 min per session/subject • performing Moiré topography—10 min per session/subject
According to these data, time required to obtain a simple “yes/no” decision about patient's status (medical examination) takes 3 min. More detailed examination, which gives quantitative results comparable in time, takes 5 min. Measurement using the developed system takes around 5 min and requires another 3–5 min, depending on the configuration, to perform in-depth analysis of the results and deliver a report. The first part of the examination does not require the presence of a physician/physiotherapist, so the time of engagement of a skilled professional is comparable to or shorter than for the classical examination. At the same time the system offers a high degree of objectiveness and rich, accurate documentation.
Future development of the method is predicted in automatic anatomical landmark recognition to shorten the physician/physiotherapist's engagement time. The development of new systems allowing for reliable automatic detection 38 may significantly lower the costs of medical personnel. These costs were considered the main source of expenses mentioned in articles recommending against school screening. 46
Owing to economic reasons, screening for scoliosis has often been described as controversial. 45,47,48 However, the need for secure assessment of the scoliosis seems to arise again in the community, 47 particularly among parents, school administrators, and educators. The recommendation for conducting scoliosis screening has recently changed because of the change in methodology of rating the existing evidence. 46 Arguments against school screening also consisted of the relatively increased screening cost due to unnecessary follow-up of students with insignificant curves and the high over-referral and false-positive rates. 49,50
In any screening procedure, a unified report containing images and several parameterized measures of the subject exam used in the traditional method should be provided. The results of the examination produced by the developed system are reported in an accessible form for subjects (patients) and parents. Reports containing postural screening results can be printed and delivered or e-mailed to parents and their children. Traditional screening may consume additional time for reporting and produce no results accessible for an independent, second opinion. Quantitative evaluation becomes crucial in the case of development of the curvature (usually painless), which may remain unnoticed by both the parent and child. Parents could potentially see their children's back asymmetry. However, minor deformities could be easily missed by an untrained observer. Adolescents can hardly inspect their own backs, particularly having no good reason for doing this (no pain). Surface topography assessment can be performed with no risk as frequently as required and much more often than radiography (because of lack of radiation exposure).
A 3D calibrated measurement system has the potential to significantly improve existing examination standards. Additionally, it can be used as a monitoring method besides (or sometimes instead of) any other measures applied to patients treated conservatively (i.e., bracing or rehabilitation).
Regardless of the method (traditional or surface topography), screening requires similar logistics to organize and perform examinations. In both methods subjects are asked to expose their undressed backs during examination. 6 –8,11,14,16,17,31,51,52 Introduction of the screening program requires explanation of all the details of the screening to the subjects, regardless of the method used for examination. The examination requires securing the confidence, understanding, and cooperation of the persons participating in the screening process because subjects may be shy and anxious. 6,53 A system like the one presented here does not require any palpation, which may improve the subject's perception of the screening procedure. Finally, all aspects of the subject's privacy can be easily protected.
Conclusions
Our study confirmed satisfactory time effectiveness for the implemented telediagnostic postural screening procedure. New methodologies allowing for 3D assessment of the human body may improve efficiency and quality of the screening for scoliosis and faulty postures. We assume that it may influence the cost-effectiveness of the screening, which is usually mentioned as an important factor for recommendations against postural school screening. Relatively fast Internet connection and a medium-level PC configuration is sufficient for achieving a reasonably short time of 3D posture assessment. Electronic version of the reports can effectively supplement the electronic health record for each subject. Using such assessments may supplement or even potentially replace current standards with posture-describing metrics. The efficiency of remote assessment of exact 3D surface topography promises future implementations in large-scale studies for posture and scoliosis epidemiology. It may improve parents' and subjects' awareness through posture monitoring based on noninvasive measurements and storage of data in an interoperable electronic health record.
Footnotes
Acknowledgments
The work described in this article was funded by the National Center for Research and Development (project NR13-0020-04/2008).
Disclosure Statement
No competing financial interests exist.